

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
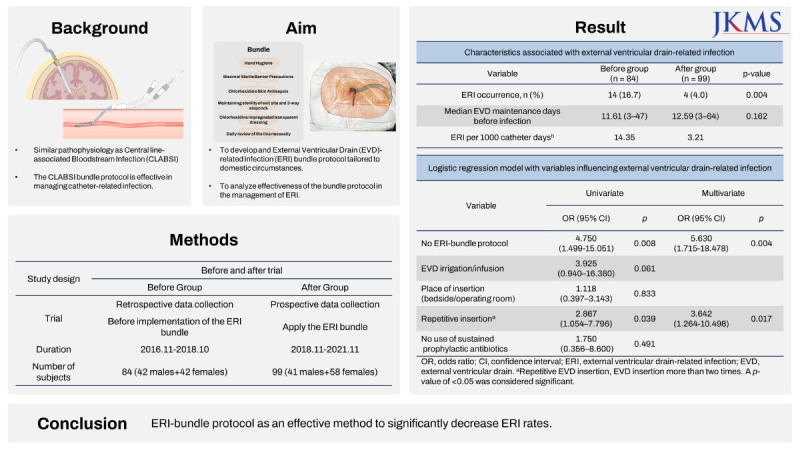
External ventricular drains (EVDs) are commonly used for temporarily diverting cerebrospinal fluid (CSF) and monitoring intracranial pressure. EVD-related infections (ERIs) are mainly caused by microorganisms from the skin flora, similar to central line-associated bloodstream infections (CLABSIs).12 The incidence rate of ERIs is considerable, ranging from 5 to 20 per 1,000 EVD catheter days and 9–20% of the patients with EVDs.345 EVD insertion using anatomical landmarks is universally well established. Although ERI can result in significant morbidity and mortality due to ERI, and several risk factors have been identified,6 there are currently no evidence-based guidelines for managing EVDs after insertion.7
The CLABSI care bundle, based on guidelines published by the Centers for Disease Control and Prevention, was shown to be effective in reducing CLABSI rates.18 Given the pathogenic similarities between infections associated with EVDs and CLABSIs, we developed and introduced a new ERI care bundle protocol based on the CLABSI care bundle. In the context of bundle management, ‘bundle’ refers to the holistic management of all maneuvers related to a catheter in an integrated manner, going beyond the individual management of elements that pose infection risks, from catheter insertion to removal, in order to minimize the risk of catheter-related infection. We subsequently conducted a before-and-after trial to evaluate the effect of the new ERI care bundle on ERI rates.
METHODS
This study was a before-and-after trial of the new ERI-bundle protocol conducted in the intensive care unit (ICU) of a tertiary hospital in South Korea from November 2016 to November 2021. Retrospective data were collected for the period before the introduction of the newly developed ERI-bundle protocol, which performed from November 2016 to October 2018, and this period is referred to as the ‘before group.’ Data for the ‘after group,’ which involved the introduction of the protocol from November 2018 to November 2021, were collected prospectively.
The study included patients who were admitted to the surgical ICU or emergency ICU after EVD insertion at the study site hospital. Exclusion criteria were previous central nervous system infections, such as ventriculitis, encephalitis, or brain abscess; skull base surgery; EVD insertion performed at a different hospital; and EVD removal within 3 days of insertion.
Conventional management before ERI-bundle protocol introduction
Prior to the introduction of the ERI-bundle protocol, the type and maintenance period of prophylactic antibiotics differed according to the attending physician. First- or third-generation cephalosporin were selected, and antibiotics were maintained in most cases during the catheter maintenance period. EVD insertion site was dressed daily using povidone–iodine or chlorhexidine cotton balls and aseptic adhesive dressing pads. The EVD catheter was replaced prophylactically at regular intervals, typically every 7 days, even if there is no evidence of infection. CSF was collected through a 3-way stopcock with sterile gloves without a full drape, and a daily CSF profile study was performed focusing on red blood cell count; white blood cell count; white blood cell differential count; and protein, glucose, and chloride level measurement. CSF was cultured when an infection was suspected based on the results of the CSF profile study or when the EVD was removed.
Newly developed ERI-bundle protocol
A multidisciplinary team, consisting of an infectious disease specialist, neurosurgeons, and ICU nurses, developed the ERI-bundle protocol based on the CLABSI management bundle and introduced the protocol hospital-wide. The protocol consisted of three parts, each introducing standard methods for placement, dressing, and manipulation of the EVD (Table 1). The protocol emphasized the following points: 1) skin preparation using 2% chlorhexidine instead of povidone–iodine; 2) avoiding routine prophylactic antibiotics usage for the entire period of having catheterization—first generation cephalosporin were given only once prior to the skin incision; 3) applying a transparent adhesive chlorhexidine gluconate (CHG) gel pad instead of daily dressing, which was checked daily without breaking the seal—if no abnormalities were observed at the insertion and connection sites, the dressing was changed once a week (Fig. 1) conducting CSF sampling using sterile technique.
Table 1
Newly developed EVD-related infection bundle protocol
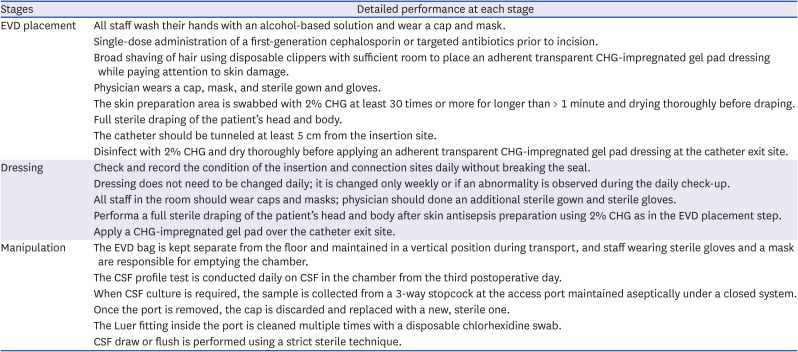
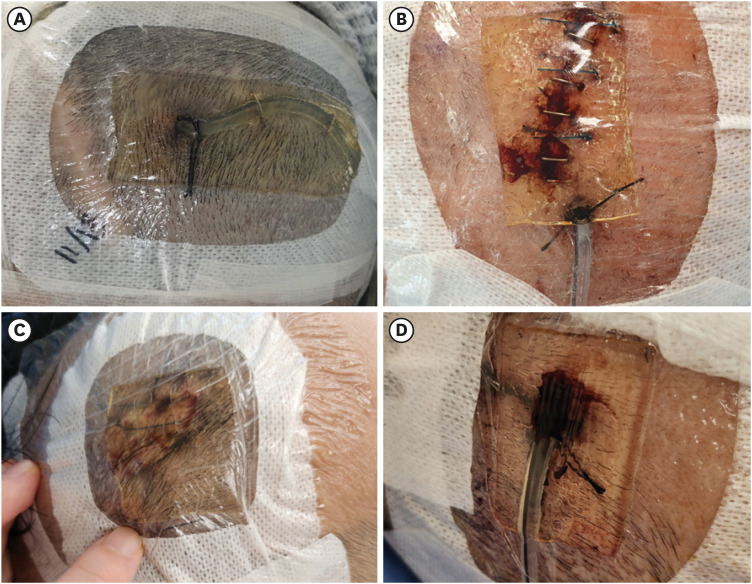
Fig. 1
Application of chlorhexidine-impregnated gel pad dressing. The transparent chlorhexidine-impregnated gel pad dressing is applied to the exit zone of the EVD catheter. Place the exit zone in the center of the chlorhexidine-impregnated gel pad (A). If the exit site of the catheter is not located in the center of the gel pad (B), or the pad dressing did not adhere well due to hair, or there was oozing/hematoma (C, D), a new dressing should be applied.
EVD = external ventricular drain.
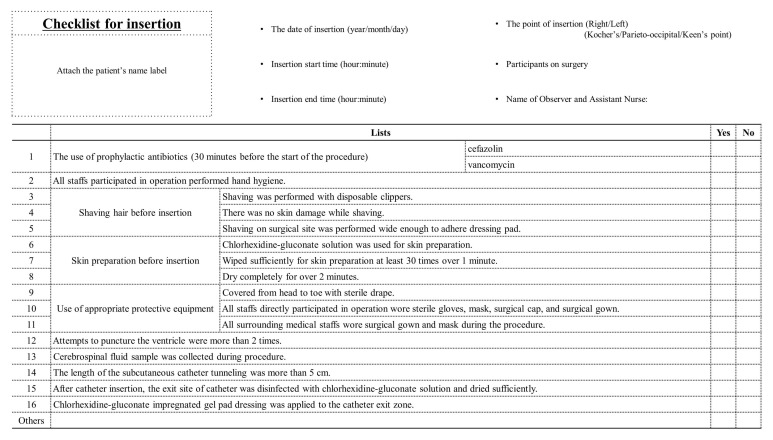
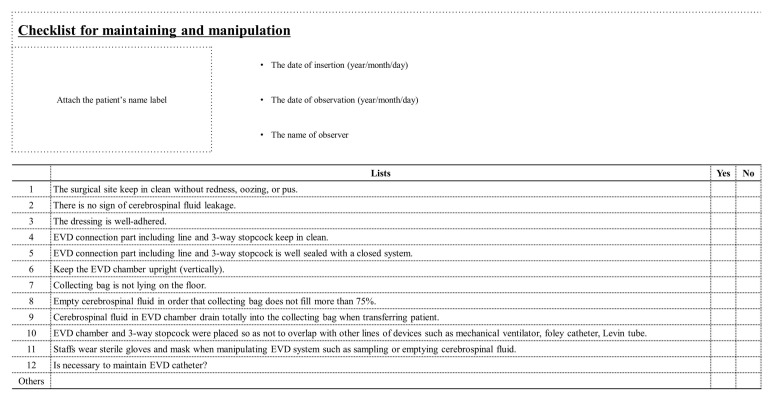
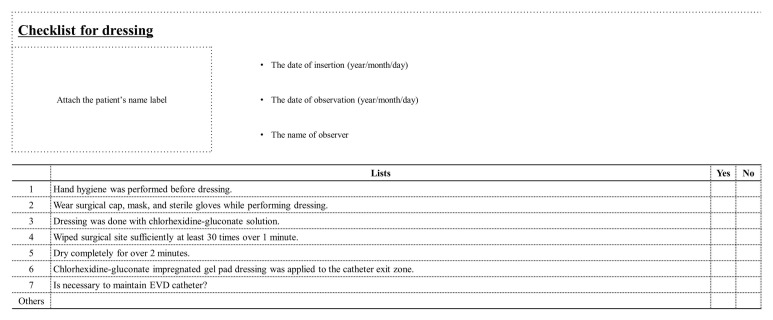
Education on the ERI-bundle protocol was provided through face-to-face meetings with physicians and nurses involved in EVD placement, dressing, and manipulation. Additionally, checklists were developed for EVD insertion, daily management, and dressing (Figs. 2-4). All staff completed the checklists to ensure that the EVD was managed in compliance with the protocol. Furthermore, daily surveillance was carried out through the checklists to confirm compliance rate. All EVD catheters used during both study periods were regular catheters, not antibiotic-impregnated catheters (AICs).
Definition of CSF infection
In defining the diagnostic criteria for CSF infection, we adopted a multidisciplinary approach. This criterion was deliberated in consultation with an infectious disease specialist and the infection management team. It also references the standards set by the Centers for Disease Control and Prevention, which specify meningitis/ventriculitis (code CNS-MEN), as well as findings from previous neurosurgical studies.679101112 Additionally, we endeavored to enhance sensitivity in line with the objectives of surveillance.
CSF infection was defined as positive if organisms were cultured from CSF or the removed catheter tip, or at least one of the following CSF abnormalities was detected671112: 1) low glucose level < 40 mg/dL or 50% serum glucose, 2) high protein level > 50 mg/dL, and 3) high cell count (white blood cell) > 1,000/mm3 with 50% or more polymorphonuclear leukocytes. Additionally, at least two of the following symptoms without another clear source of infection should be detected: 1) fever > 38°C, 2) one meningeal sign, including headache, neck stiffness, new onset or more frequent than before, uncontrolled, exhibiting a different nature of headache, new onset of seizure, Kerning’s sign, and Brudzinski’s sign, and 3) new or worsening deterioration of consciousness.
Data collection
Variables included in the analysis were age, gender, cerebral primary diagnosis, underlying disease, place of EVD insertion, number of repeated EVD insertions, co-operation during EVD insertion, whether extended tunneling over 5 cm is performed, duration of operation, and whether irrigation or infusion of tissue plasminogen activator or nimodipine was performed through EVD. In order to analyze the relationship between the implementation of the ERI-bundle protocol and the occurrence of ERI, we checked the total number of EVD insertions, total catheter days with EVD, and number of days with EVD before infection. The infection rate was expressed as infections per 1,000 catheter days. Additionally, the checklist items shown in Figs. 2-4 were collected simultaneously.
Statistical methods
Continuous measurements were summarized with median values and analyzed with the non-parametric Kruskal–Wallis equality-of-populations rank test. Categorical data were analyzed with the Fisher exact test. Multivariate regression analysis was performed with predictors entered if the significance level was P < 0.05 in the univariate regression analysis. Statistical analysis was performed using IBM SPSS Statistics software (version 20.0; IBM Corp., Armonk, NY, USA).
Ethics statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The Institutional Review Board (IRB) of our institute approved this study (IRB Number from Seoul National University Hospital: 1905-184-1037). Informed consent was waived for the retrospectively studied subjects because our study did not adversely affect their rights and welfare. Participants or the legal guardians of participants in the newly developed bundle protocol group provided written informed consent prior to study enrolment.
RESULTS
Participants and operation related factors
Baseline characteristics of patients before and after the ERI protocol implementation were similar. Eighty-four patients (42 males and 42 females) with a median age of 57 (range, 17–88) years were included in the patient cohort before the ERI bundle protocol introduction. Data after introduction of the ERI bundle were prospectively collected from November 2018 to November 2021. Ninety-nine patients (41 males and 58 females) with a median age of 59 (range, 16–88) years were included in the patient cohort after the ERI bundle protocol introduction. The most common primary diagnoses included intra-cerebral hemorrhage/intra-ventricular hemorrhage (44.0% and 46.5%, respectively), followed by subarachnoid hemorrhage and tumor/mass. No significant differences in diagnoses were observed between the two groups (P = 0.166). Additionally, no significant differences were observed in factors related to ERI, such as EVD insertion site, repetitive EVD insertion, extended tunneling of the catheter, and urokinase/tissue plasminogen activator irrigation or antibiotics/artificial CSF infusion through the EVD (Table 2).
Table 2
Patient’s baseline characteristics and factors related to operation

Values are presented as number (%) or median (range). P values for comparison of continuous measures were calculated using the non-parametric Kruskal–Wallis equality-of-populations rank test, and for comparison of categorical measures, Fisher’s exact test was used. A P value of < 0.05 was considered significant.
ERI = external ventricular drain-related infection, BMI = body mass index, ICH = intra-cerebral hemorrhage, IVH = intra-ventricular hemorrhage, SAH = subarachnoid hemorrhage, TBI = traumatic brain injury, CNS = central nervous system, RTx = any kind of brain radiotherapy, EVD = external ventricular drain.
aAlcohol abuse, > 112 g of alcohol for males and > 54 g for females.
Primary outcome: ERI rate
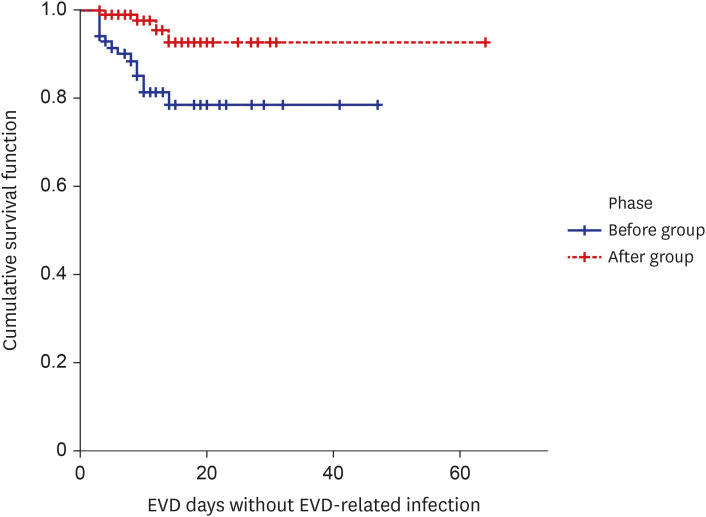
The ERI rate decreased significantly from 16.7% (14 of 84; 14.35 per 1,000 catheter days) to 4.0% (4 of 99; 3.21 per 1,000 catheter days) after the ERI-bundle protocol introduction (P = 0.004). Although the difference was not statistically significant, the EVD catheter tended to be maintained longer after the ERI-bundle protocol introduction compared to before the protocol introduction, (median [range]: 12.59 [3–64] vs. 11.61 [3–47] days, P = 0.162) (Table 3). Based on the daily surveillance data with checklists (Figs. 2-4), the compliance rate of the ERI-bundle protocol was 94%. In addition, the Kaplan-Meier curves for infection to compare the timing of infection. Before the introduction of the ERI-bundle protocol, the 7-day ERI-free rate was 79.2%, and the 14-day ERI-free rate was 78.6%. In comparison, after the introduction of the ERI-bundle protocol, the rates significantly increased to 98.9% at 7-day and 92.6% at 14-day (P = 0.004) (Fig. 5).
Table 3
Characteristics associated with ERI

Values are presented as number (%) or median (range). P values for comparison of continuous measures were calculated using the non-parametric Kruskal–Wallis equality-of-populations rank test, and for comparison of categorical measures, Fisher’s exact test was used. A P value of < 0.05 was considered significant.
ERI = external ventricular drain-related infection, EVD = external ventricular drain.
aTotal Catheter Days = Sum of Total EVD Maintenance Days for Each Patient.
bERI per 1,000 Catheter Days = (ERI Occurrence/Total EVD Maintenance Days without Infection) × 1,000.
Fig. 5
The Kaplan-Meier curves for ERI. Before the introduction of the ERI-bundle protocol, the 7-day ERI-free rate was 79.2%, and the 14-day ERI-free rate was 78.6%. In comparison, after the introduction of the ERI-bundle protocol, the rates significantly increased to 98.9% at 7-day and 92.6% at 14-day (P = 0.004).
ERI = external ventricular drain-related infection, EVD = external ventricular drain.
Factors associated with ERI
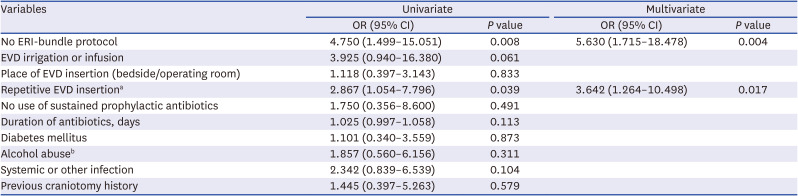
In the univariate analysis, absence of the ERI-bundle protocol (odds ratio [OR], 4.750; 95% confidence interval [CI], 1.499–15.051; P = 0.008), and repetitive EVD insertion (OR, 2.867; 95% CI, 1.054–7.796; P = 0.039) were significant risk factors for ERI. Other factors, including not maintaining prophylactic antibiotics, were not significant risk factors for ERI. In the multivariate analysis, absence of the ERI-bundle protocol (OR, 5.630; 95% CI, 1.715–18.478; P = 0.004) and repetitive EVD insertion (OR, 3.642; 95% CI, 1.264–10.498; P = 0.017) were both significant risk factors for ERI (Table 4).
Table 4
Logistic regression model with variables influencing the risk of ERI
A P value of < 0.05 was considered significant.
ERI = external ventricular drain-related infection, OR = odds ratio, CI = confidence interval, EVD = external ventricular drain.
aRepetitive EVD insertion, EVD insertion more than two times.
bAlcohol abuse, > 112 g of alcohol for males and > 54 g for females.
DISCUSSION
This study is significant in that it proposes an ERI management protocol for the first time in South Korea. There are no standardized guidelines for ERI management tailored to the unique healthcare environment in South Korea and the existing management principles have been inconsistently applied across physicians and institutes. This study was conducted to empirically verify whether the ERI rate can be reduced using the newly developed ERI-bundle protocol. In 2013, Flint et al.13 in the United States first presented a protocol, based on evidence, with the aim of reducing ERI, and its effectiveness in preventing ERI was found to be significant. For this study, certain aspects of the protocol, such as the insertion of antibiotics-coated EVD catheters, the use of chlorhexidine patches, and the application of staple lines, as suggested in Flint’s protocol, were modified to align with the specific insurance coverage and medical supply situation in South Korea. Additionally, for central nervous system infection, the sensitivity of organisms cultured in CSF is not high. Therefore, even if the CSF culture is negative, ERI was defined considering the CSF profile and meningeal signs together, as the primary diagnosis of neurosurgical disease may affect the CSF profile.
The management of CLABSI from insertion to removal has been shown to significantly reduce catheter-related infections.1415161718 The pathophysiology of ERI is similar to that of CLABSI as both are often caused by skin-derived bacterial colonization.19 As ERI is also a catheter-related infection, we hypothesized that the implementation of a comprehensive bundle encompassing all processes would be more effective in reducing ERI compared to individually managing each distinct risk factors. Therefore, using the CLABSI bundle management as a guide, we proposed an ERI-bundle protocol that includes guidelines for managing EVD catheter insertion, maintenance, and manipulation, as well as a daily checklist and infection surveillance by a multidisciplinary team. These points are described in detail below.
To maintain a maximal sterile barrier during catheter insertion, several measures were taken. All staff practiced hand hygiene and wore surgical caps and masks. The staff directly participating in EVD insertion also wore surgical gowns and full draping was applied.
A CHG solution was used for skin antisepsis preparation instead of povidone–iodine, as the CLEAN randomized control trial published in 2015 demonstrated a significant reduction in surgical site infections with CHG compared to povidone–iodine. Therefore, CHG is considered to be more effective in preventing infections.2021
Extended tunneling has been shown to reduce ERI rates.2223 A meta-analysis has demonstrated that a tunnel length of 5–10 cm is associated with the lowest risk of ERI.23 However, the effects of extended tunneling, longer than 5 cm, could not be analyzed in this study due to the lack of medical records.
The use of AICs is recommended for ERI bundles introduced in other countries based on several studies showing that they can reduce ERI rates.324 However, in the domestic version of the bundle, AICs were excluded due to costs and insurance coverage. The domestic version bundle proposed by this manuscript did not include AIC. However, if the insurance issue is resolved and AIC could be applied, it has the potential to considerably more reduce ERI. However, AICs should initially be used in patients with compromised immunity or those who need intensive management.
Maintenance of prophylactic antibiotics administration without evidence of infection does not significantly reduce the ERI rate but increases the occurrence of antibiotic-resistant bacteria.25262728 Therefore, prophylactic antibiotics were not administered in the ERI-bundle protocol presented in this study. No significant difference in the ERI rates was observed with and without prophylactic antibiotics administration in the before and after groups, respectively (OR, 1.750; 95% CI, 0.356–8.600; P = 0.491). In other words, prophylactic antibiotics administration is not essential.
A randomized controlled trial showed that CHG-impregnated sponges prevent catheter-related infections in critically ill patients.129 Therefore, a widely available transparent adhesive CHG-impregnated gel pad dressing was applied. The purpose of this ERI-bundle protocol is to maintain a sterile environment with a closed system. Thus, a transparent and waterproof CHG-impregnated dressing was applied to minimize infection at the insertion site.19 If the pad dressing did not adhere well due to hair or there was oozing, or if the exit site of the catheter was not located in the center of the gel pad, the dressing was reapplied (Fig. 1).
To minimize the risk of infection through the lumen, CSF sampling was performed using a cylinder in which drained CSF is collected with sterile gloves and disposable chlorhexidine swabs. When a CSF culture was required, samples were collected through a 3-way stopcock in a fully draped, sterile environment. To maintain a continuous sterile environment, the stopcock port cap was replaced with a new sterile cap once it was opened.
Having a single catheter for an extended period, particularly longer than 7 days, significantly increases the risk of ERI.4530 Therefore, physicians periodically exchange EVD catheters as a prophylactic measure to reduce the ERI rate with a new catheter. However, we have shown that repetitive EVD insertion is a significant risk factor for ERI (OR, 2.867; 95% CI, 1.054–7.796; P = 0.039) in line with past studies.3132 Therefore, the ERI-bundle protocol proposed in this study does not include periodic prophylactic catheter exchange without evidence of an ERI.
Daily surveillance with a checklist was performed to ensure the maintenance of a sterile closed system.33 Additionally, the duration of catheter indwelling was minimized through daily reviews. Since the introduction of the CLABSI bundle protocol, infection rates reach almost zero as the execution rate of the bundle protocol approaches 100%.3435 Accordingly, to increase the compliance rate of the ERI-bundle protocol, various occupations involved in EVD management and manipulation were educated, and daily surveillance was conducted through checklists (Figs. 2-4). The compliance rate for the ERI-bundle protocol was about 94%; increasing this rate to 100% should further reduce the ERI rate. The group that first proposed the ERI-bundle protocol also announced that the EVD rate was almost zero 7 years after the protocol’s introduction.12
A significant limitation of our study is the controversial ERI diagnostic criteria. While bacterial identification is definitive, the low yield of cerebrospinal fluid cultures complicates this. Our criteria, designed for infection surveillance, may overestimate infection rates by including “gray zone” patients. We prioritized sensitivity to reduce false negatives and enhance infection prevention. This, however, poses a risk of unnecessary tests and treatments in false positive cases. Future studies should incorporate PCR or advanced diagnostics for clearer bacterial identification.
There are several well-known factors related to the processes of ERI insertion, maintenance, and manipulation, including extended tunneling, irrigation, and infusion through the EVD catheter, and the use of AIC.324 However, in this study, irrigation/infusion through the EVD catheter and extended tunneling were not found to be significant factors in reducing infection. It is worth noting that the sample size of this study was small (11 cases of irrigation/infusion) and there was missing data for extended tunneling (62 cases, 33.9%). Further studies with a larger number of subjects are necessary to validate these findings. Also, it is important to note that this study was conducted in a single institution with a small number of subjects, and larger multicenter studies are needed to confirm the effectiveness of the ERI-bundle protocol.
We suggest the ERI-bundle protocol as an effective method to significantly decrease ERI rates.
 XML Download
XML Download