

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The term “transgender” broadly includes people whose gender identity differs from their birth-assigned sex, such as trans-men, trans-women, and may also include intersex individuals that do not match the typical notions of male or female bodies. Transgenders began to appear as a population in the Korean community in the early 1990s when people sought to change their gender on their legal documents after undergoing gender-affirming surgery.1 The social and health disparities faced by transgender individuals in South Korea (Korea hereafter) remain under-documented. This is largely attributed to the absence of comprehensive epidemiological data on the transgender population and information related to gender identity.2 Since transgender status is not always visible and doesn't necessarily need to be disclosed, transgender individuals are often less visible in data compared to other demographic groups.3
Research on sexual minorities, particularly the transgender community in Asian countries, has been limited due to cultural and societal stigmas.4 Much of the existing data is rooted in Western populations, predominantly focusing on Caucasians. In Korea, studies on transgender health disparities have often been web-based, sourced from media-driven surveys.567 The exact size of the transgender population in Korea remains undetermined. However, using U.S. estimates, where 0.6% of adults identify as transgender, it is projected that Korea has over 200,000 transgender individuals in its 50 million population.18
For effective healthcare planning and policy-making, it is vital to ascertain the number of at-risk individuals. Transgender individuals reportedly face greater challenges, including limited healthcare access, heightened mental health issues, discrimination, and higher vulnerability to HIV/AIDS.910 Furthermore, feelings of alienation may also contribute to adverse health outcomes.11 A comprehensive study can reveal the depth of these risks within the transgender community. Addressing their needs is crucial to bridging health disparities. Epidemiological studies highlight these, facilitating evidence-based interventions and targeted support.
To the best of our knowledge, no study has been conducted in Korea to quantify the prevalence and clinical attributes of the transgender populations. Earlier research often relied on limited surveys or interviews. However, with the majority of Koreans enrolled in the National Health Insurance (NHI) and the Health Insurance Review and Assessment Service (HIRA) cataloging comprehensive medical data, there’s potential for detailed transgender research. Our objective is to harness this extensive data to understand the challenges faced by transgender individuals and shape targeted healthcare interventions for their well-being.
This study is pioneering in its use of the HIRA Big Data Hub to estimate the current population of transgender individuals in Korea, track clinical patterns, and shed light on experiences and barriers to transition-related healthcare.
METHODS
Data
The HIRA is a quasi-governmental institution that reviews and assesses healthcare costs and quality in Korea. Because all Korean citizens are automatically enrolled in the NHI system at birth, the HIRA database contains all relevant data once a medical provider has filed a claim. Since 2007, transgender individuals have been categorized under F64.9 for “gender identity disorder” or F64.0 for “Transsexualism” according to the International Classification of Diseases, Tenth Revision. This retrospective study, based on extensive data, encompasses patients diagnosed with any of the F64 codes from January 2007 to December 2021. Demographics including age, sex assigned at birth, the initial diagnosing institution, and intersex characteristics were extracted from the HIRA database. Psychotropic medications were evaluated and classified by HIRA into sedatives or anxiolytics. Additionally, data on patients displaying "intersex" traits was compiled, and indications of gender-affirmative care were discerned through hormone therapy prescription records. We randomly divided the population into ten 10-year groups (“0–10” to “100–) and determined the average duration, in days, between initiation of psychotropic medication and the F64 diagnosis.
Statistical analysis
This study utilized data obtained from the HIRA Big Data Hub and analyzed the demographics and medical profiles of transgender and intersex individuals. Univariate descriptive statistics were presented as the mean, median, frequency, and ratio of several items. SPSS (version 9.3 SAS Institute, Cary, NC, USA) was used to perform all statistical analyses.
RESULTS
Demographics
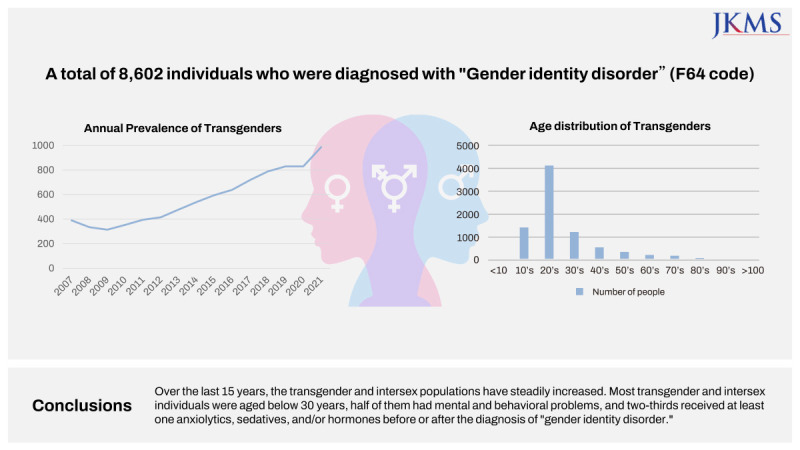
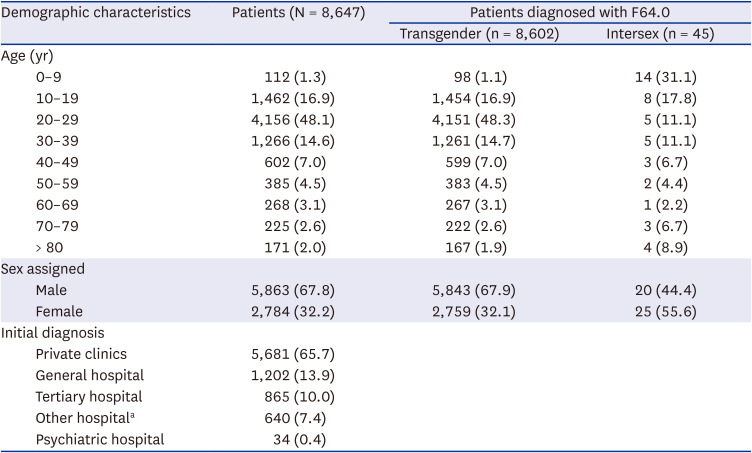
Table 1 shows the demographic characteristics of the study population. Between January 1, 2007, and December 31, 2021. The total number of patients studied is 8,647, of which 8,602 are transgender and 45 are intersex. The age group with the highest prevalence of transgender individuals is 20–29 years, accounting for a significant 48.3% of the transgender population. Intersex individuals, however, are more dispersed across age groups with the 0–9 age group having the highest percentage of 31.1%. The least prevalent age group for both transgender and intersex populations is 60–69 years, representing only 3.1% and 2.2%, respectively. The majority (67.8%) were assigned male at birth, while 32.2% were assigned female. Notably, among intersex patients, 55.6% were assigned female at birth, slightly more than those assigned male (44.4%). The majority of patients (65.7%) received their initial F64 diagnosis in private clinics. General hospitals and tertiary hospitals were the next most common institutions for diagnosis, accounting for 13.9% and 10.0% of the patients, respectively. Fewer patients received their diagnosis at standard hospitals (7.4%) and an even smaller fraction, only 0.4%, were diagnosed at psychiatric hospitals.
Table 1
Demographic characteristics of patients diagnosed with F64 codes
Temporal trends in patient numbers
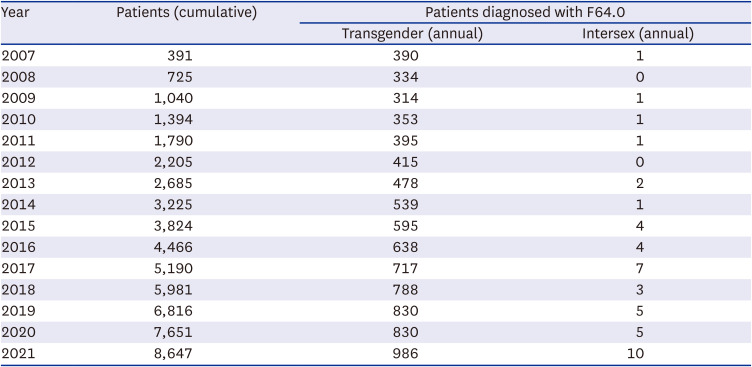
The data spanning 2007 to 2021 shows an evident increase in the cumulative number of patients diagnosed with F64 codes as shown in Table 2. Annual figures for transgender individuals show progressively increasing trend. From an initial 390 cases in 2007, there is a noticeable growth with 2021 recording a substantial 986 new cases. Periods between 2016 to 2021 saw more substantial annual increases than previous years and a surge of 156 cases from 2020 to 2021. The intersex population, although significantly lower, display sporadic variations over the years. Starting with one case in 2007, there is no uniform pattern discernible across the years. However, 2021 notes a noticeable spike with 10 new cases, the highest over the provided time span.
Table 2
Annual prevalence of patients diagnosed with F64 codes between 2007 and 2021
Psychotropic medication and hormones
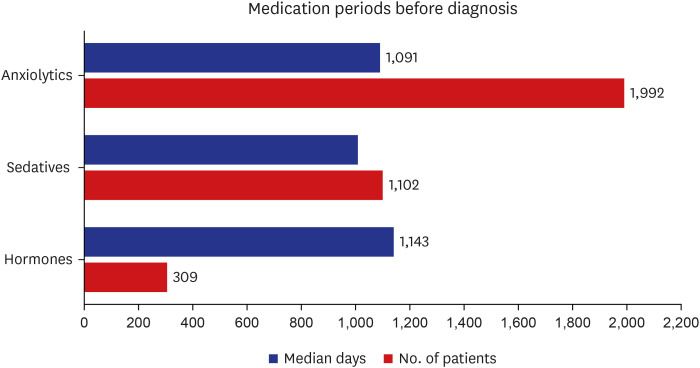
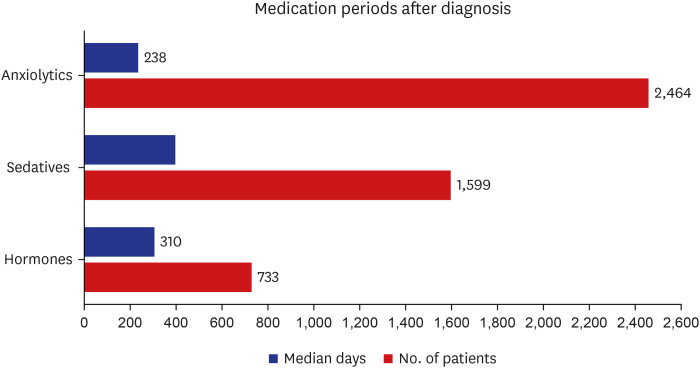
Figs. 1 and 2 show medication types and periods before and after the diagnosis of F64 codes. Anxiolytics (51.8%) were the most commonly administered medication both before and after the diagnosis, followed by sedatives (31.4%) and hormone therapy (12.1%). Hormone therapy (1,143 days), anxiolytics (1,091 days), and sedatives (1,010 days) had the longest median drug administration before diagnosis. Sedatives (401 days), hormones (310 days), and anxiolytics (238 days) had the longest median drug administration after diagnosis. Approximately half (53.2%) of F64 patients were initially diagnosed with “mental and behavioral disorders” with a median period of 1,458 days.
DISCUSSION
Our study, harnessing comprehensive data from the HIRA Big Data Hub, unveils the significant growth of the “transgender” and “intersex” population in Korea over the past 15 years. The possible reasons for this surge could range from enhanced healthcare accessibility to broader societal acceptance, leading to a heightened cumulative identification of cases.12
Interestingly, despite this increase, a significant number of transgender patients in Korea abstain from transitional therapy.13 A potential rationale is the limited national healthcare service coverage for transitional treatments, compelling many to opt for out-of-pocket medical services. This is evident in our findings where a mere 12.1% accessed hormone therapy covered by health insurance. Previous studies resonate with these findings, shedding light on high medical costs, unfavorable interactions with healthcare providers, and a general paucity of transition-related knowledge among both clinicians and transgender individuals.1415
It is well-documented that transgender individuals grapple with persistent gender dysphoria and the burdens of chronic minority stress.16 Mental health disparities in our study align with global research. While a national mental health survey by the Korean Ministry of Health and Welfare in 2016 reported a 5.0% prevalence of major depressive disorder,17 our study showed 19.2% of transgender individuals suffered from mental health disorders. Similarly, an Australian study discovered a staggering 57.2% lifetime depression prevalence among transgender individuals.18 The elevated mental health disorder prevalence in our cohort (53.2%) corroborates existing literature suggesting heightened mental health vulnerabilities among transgender individuals compared to the broader population.192021
To our knowledge, this is the first endeavor to quantify the demographics of transgender and intersex communities in Korea via a nationwide database. The study discerns a consistent upward trajectory of individuals diagnosed with F64 codes over the past decade and a half, predominantly among those below the age of 30. These findings accentuate the need for specialized mental health provisions, policy amendments, and early interventions tailored to this community. The widespread prescription of anxiolytics and sedatives, either before or after diagnosis, underscores the significant psychological stress experienced by those facing gender identity challenges.
Furthermore, an insight into transgender and intersex communities in East Asian countries were offered. While Western societies, such as the U.S. and Canada, have made strides in recognizing transgender rights and implementing legislation for the legal acknowledgment of gender identity changes,21 East Asian nations remain anchored to rigid traditional gender norms. Such norms exacerbate the stigmatization and discrimination endured by transgender individuals.
While our study offers critical insights, it is not without limitations. Sole reliance on the F64 code might not capture the true prevalence, as not everyone with gender dysphoria seeks or receives a diagnosis. The retrospective nature of the study means that causal relationships between observed trends and other factors cannot be determined. However, the findings hold paramount importance for healthcare providers, policymakers, and researchers.
In conclusion, this large-scale, retrospective study provides previously unavailable baseline data on the prevalence of the transgender and intersex population in Korea, emphasizing the critical need for specialized mental health services, early interventions, and comprehensive support tailored to their unique challenges. The stark contrast in mental health statistics compared to the general population and the West further accentuates the need for reforms. This research also emphasizes the need for more inclusive healthcare policies and societal reforms. Ensuring these communities’ holistic well-being requires multifaceted efforts, ranging from healthcare optimization to enhanced societal understanding and acceptance.
 XML Download
XML Download