

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Looking at the age-standardized suicide rate (the number of suicide deaths per 100,000 people) in Organization for Economic Cooperation and Development (OECD) countries, Korea maintained its top position almost every year from 2003 to 2019, when the statistics were released. The number of suicides per 100,000 people in Korea is 24.6, which is more than double the OECD average of 11.3.1
Although many scholars are studying suicide to lower the suicide rate, several limitations exist due to the absence of subjects to directly study suicide completion. The suicide process begins with suicidal ideation (SI), goes through suicide attempts, and ends with suicide completion.2 SI, the initiating stage of the suicidal process, is one of the strongest predictors of suicide attempts3 and a precursor to more severe suicide-related behaviors.45 Furthermore, as per a past study, the frequency of SI was found to be more related to suicide plans and attempts than other factors.6 Moreover, 60% of the transition from SI to a suicide plan and attempt occurred within one year.7 For this reason, research on SI to lower the suicide rate is thought to contribute toward preventing suicide in the early stages of the suicide process.
Psychological factors such as depression, hopelessness, mental disorders, and impulsivity are universal predictors of SI, which can lead to suicide attempts.8 In a study of college students in the United States, 6% of freshmen currently had SI, and 40% of them were classified as being depressed. Among those with depression, low social support, emotional dysregulation, discord with their father, and alcohol dependence were essential predictors of SI.9 In the case of American men, the degree of hopelessness and depression was significantly associated with SI in those who had a relatively tolerant attitude toward suicide.10 In a Portuguese study that studied the relationship between SI and factors such as depression and quality of life in older adults, a significant relationship was found.11
SI is also influenced by socio-demographic and health behavioral factors. For example, a study of European elementary school students found that the suicide rate was 16.96% higher in single-parent or large families.12 In an analysis of the relationship between bullying and SI among adolescents in 10 European countries, students who were bullied with physical harm were more likely to have SI.13 In a study of German adults, no longer living with a partner, job loss, and decreased income were associated with SI.3 In a Japanese study of office workers, problematic drinking and absence of friends were related to SI in both men and women.14 Another study on passive SI assessed accidental death without the intervention of one’s own will for older adults in Europe. This study mentioned the female gender, depression, older age, poor health, smaller social network size, loneliness, non-religiosity, and low perceived control as predictors of SI.15 In a study analyzing all age groups of adults in 17 European countries, the female gender, low age, low educational attainment, and being single were factors affecting suicidal behavior, including SI.7
There have been many studies on SI in Korea, especially among adolescents and older adults. First, a survey of SI among high school students showed that in the case of male students, parental divorce, parental alcohol abuse, depression, smoking, relationships with friends, hostility, and self-esteem were predictors of SI. In female students, bullying, depression, hate, sexual orientation, and self-esteem were predictors of SI.16 A study that examined the relationship between Internet addiction and SI among adolescents revealed that the rates of depression and SI were high among adolescents with Internet addiction.17 In a study investigating SI and risk factors in older adults, the rate of SI was 37.5% for women and 17.5% for men. Suicide-related factors for both men and women included depression, stress, physical exercise restriction, and quality of life. Low educational attainment and economic status were related to SI in men.18 An article that studied SI in a general population in their 20s to 50s suggested that SI may be related to a family history of mental illness, depressed mood, anger, and short or long sleep periods.19 In another specific group, vulnerable articles that studied SI in subjects in their 20s or older with a feeling of depression revealed that the factors significantly affecting SI differed for each age group.20
As discussed above, not only suicide completion, but also various suicide behavior-related factors show different characteristics according to age and gender. The OECD states that young people and older adults are vulnerable to suicide. Although suicide rates in other OECD countries tend to decrease in general, they are still increasing among the youth and older adults in Korea.21 For this reason, many studies have focused on these populations. However, according to the “Five-Year National Suicidal Death Analysis Results Report,” the highest suicide rate was among the late middle-aged group (50–64 years), followed by the early middle-aged group (36–49 years).22 Nevertheless, there are only a few studies on middle age individuals. According to the Centers for Disease Control and Prevention mortality statistics, 50% of those who died by suicide were never diagnosed with a mental illness, such as depression.2324 Suicide can thus even occur in people who do not have mental or psychological problems. Accordingly, in suicide-related research, it would be meaningful not only to study a specific group vulnerable to suicide, but also to search for factors related to SI in a general group. The White Paper on Suicide Prevention: the idea-to-action framework, published by the Ministry of Health and Welfare since 2014, explains the suicide rate by gender, suicide means by age, and suicide status by motive provided by the National Police Agency.25 However, because this white paper includes data on suicide deaths, it is thought that there is a limit to accurately grasping suicide-related factors. Therefore, to overcome these limitations, our study utilized Korea’s representative long-term health and big medical data (National Health and Nutrition Survey data from 2013 to 2019). Multiple logistic analysis was performed on the factors related to suicidal ideation by stratifying not only by age and gender, respectively, but also by age group according to gender, targeting a large general adult group of 18,339 people.
Identifying the factors related to SI by sex for each age group is expected to provide valuable data for planning and implementing the suicide prevention project promoted by the government to reduce suicide rates, contributing toward the prevention of suicide-related behaviors.
METHODS
Dataset
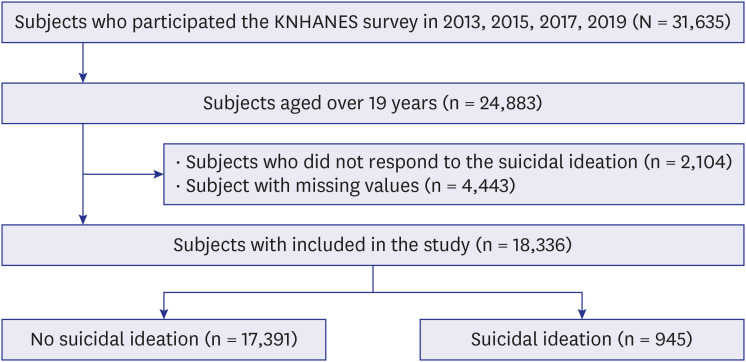
This study used data from the Korea National Health and Nutrition Examination Survey (KNHANES). The KNHANES is a nationwide cross-sectional survey conducted by the Korea Centers for Disease Control and Prevention to evaluate the health and nutritional status of Koreans. To select representative households of Koreans, stratification and multilevel cluster probability sampling were used. The data consisted of a health questionnaire and nutrition and health checkup items; the survey design, data collection, and detailed protocol of the National Health and Nutrition Examination Survey data were already made public.26 The current KNHANES data are available from 1998 to 2020. Among them, data from the 2013, 2015, 2017, and 2019 surveyed adults were used to compare whether they had SI (Fig. 1).
Definition and variables
In the KNHANES data, the dependent variable was whether people seriously considered suicide during the past year. As an exploratory study, this study referred to previous studies to understand the overall effect of age and gender on suicidal ideation. Independent variables, including the area of demographic factors,1127 lifestyle behaviors factors,27 psycho-emotional variables,11 and health status related variables11 were selected. Independent variables included sex, inmate, household income level, economic activity status, residence type, education level, depression, subjective health perception, stress level,28 sleep duration,29 chronic disease, smoking,30 marital status, weekly breakfast and dinner frequency,31 the Euro Quality of Life–5 Dimensions (EQ-5D) index, exercise, 28 obesity, and comprising a high-risk drinking group.32 Exercise was divided into three categories according to the distribution of the number of exercise sessions per week. In addition, the high-risk drinking group was divided into categories according to the percentage of drinking more than seven drinks per day (five drinks for women) and drinking more than twice a week. The EQ-5D index is a variable that can measure one’s quality of life related to health. It consists of five items and can be converted into a score between −1 and 1; the higher the total score, the higher the quality of life. Considering that most scores had a distribution close to 1, the EQ-5D index was divided into two categories based on Q1. One was defined as having a chronic disease if at least one of the following was applicable: hypertension, dyslipidemia, stroke, myocardial infarction, angina pectoris, arthritis, osteoporosis, tuberculosis, asthma, chronic obstructive pulmonary disease, or diabetes.
Statistical analysis
Considering the characteristics of the KNHANES data, a complex sample analysis was performed by examining the primary extraction unit (region), stratification variables, and weights. The χ2 test was stratified by age group to confirm the distribution of SI according to the general characteristics. Univariate and multiple logistic regression analyses were performed to determine the effects on SI. Among subjects in their 20s to 80s, the median age was in their 50s, and because the characteristics of the subjects before and after could be clearly observed, 50 years of age was set as the reference in the logistic regression analysis. P values less than 0.05 were considered statistically significant. The software used for the analyses was SAS (version 9.4; SAS, Cary, NC, USA) and R 4.0.3 (Institute for Statistics and Mathematics, Vienna, Austria; http://cran.r project.org).
RESULTS
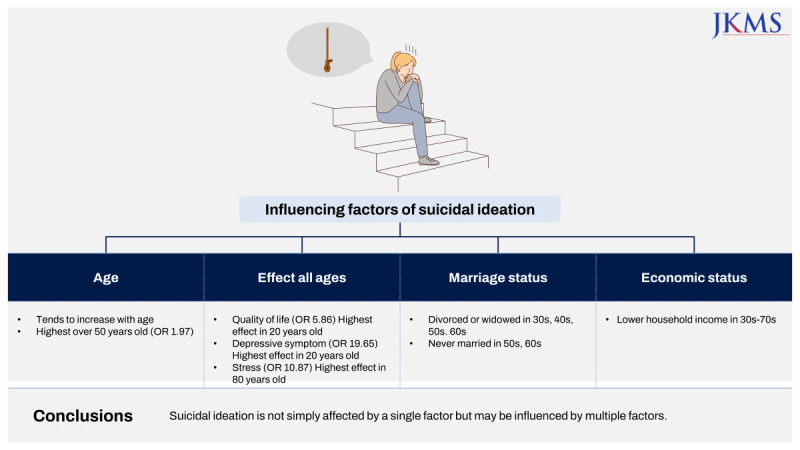
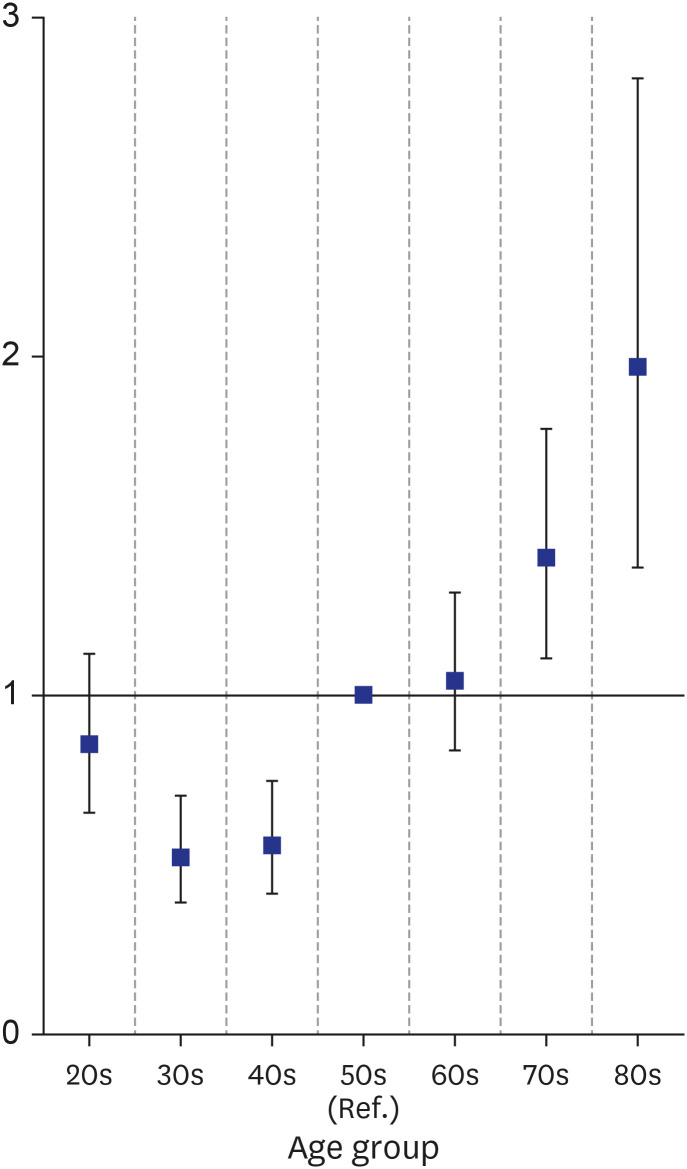
Fig. 2 shows the logistic regression analysis results of SI according to age group. Compared with those in their 50s, those in their 30s had the lowest rate of SI (odds ratio [OR], 0.52; 95% confidence interval [CI], 0.39–0.70), and those in their 80s had the highest rate of SI (OR, 1.97; 95% CI, 1.38–2.82). Except for those in their 20s, the rate of SI tended to increase with age.
In all age groups, the rate of SI was higher in women; in particular, in 40-year-old women, the rate was high (65.54%). In addition, in all groups, SI was high in individuals whose education level was below elementary school graduation, the bottom 25% of the EQ-5D index, those who had continued depression for more than two weeks, and those who had poor subjective health or much stress (Table 1). Variables with a high rate of SI by age group were as follows: those in their 20s who did not eat breakfast (43.33%), were obese (37.46%), and slept for less than six hours (13.44%); those in their 30s who did not participate in economic activities (40.30%); those in their 40s who were obese (47.97%) and in the high-risk drinking group (25.54%); those in their 50s who lived alone (19.45%), exercised less than one time (48.01%), did not eat dinner (1.49%), were in the high-risk drinking group (19.53%), and slept for less than six hours (26.77%); those in their 60s who lived alone (32.80%), exercised less than one time (44.18%), did not eat breakfast (12.57%) or dinner (1.18%), and slept for less than six hours (31.18%); those in their 70s who exercised 0–1 time (51.20%); and those in their 80s who did not eat dinner (2.59%). In particular, divorced, widowed, and single individuals, and smokers in their 30s and 60s had a high rate of SI; in all age groups except that of those in their 20s, the SI rate was high for those in the first decile of household income (Supplementary Table 1).
Table 1
Baseline characteristics for suicidal ideation
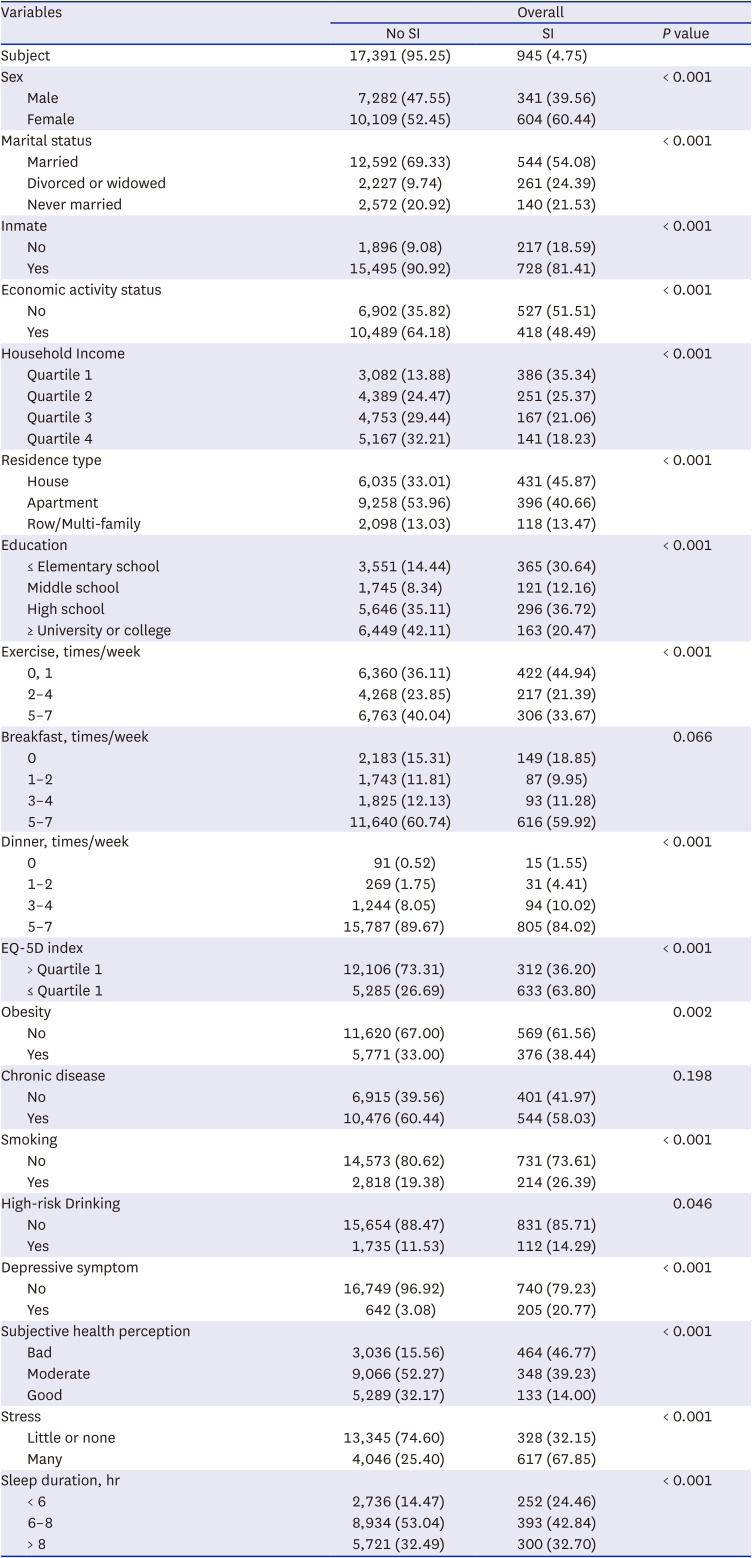
Fig. 3 shows the logistic regression analysis results of SI stratified according to age group. Overall, the probability of SI increased when the EQ-5D index was in the bottom 25%, depression persisted for two weeks or more, subjective health perception was poor, or stress was high. In particular, the EQ-5D index for those in their 20s (OR, 5.86; 95% CI, 3.73–9.20), depression for those in their 20s (OR, 19.65; 95% CI, 9.94–38.83), and stress for those in their 80s (OR, 10.87; 95% CI, 5.63–20.96) showed the highest SI; in the case of high stress in 80-year-olds or above, those with good subjective health perception, and those in their 30s (OR, 0.10; 95% CI, 0.05–0.20), SI was the lowest. People in their 30s, 40s, and 60s had higher SI when divorced or widowed, and those in their 50s and 60s had higher SI if they were unmarried or had no inmates. In all age groups, except for those in their 20s and 80s, the lower the household income level, the more likely they were to have SI. In addition, although not statistically significant, with the exception of those in their 70s and 80s, the higher the educational level, the lower the probability of SI.
Fig. 3
Univariate logistic regression result for all characteristics according to suicidal ideation stratified by age group.
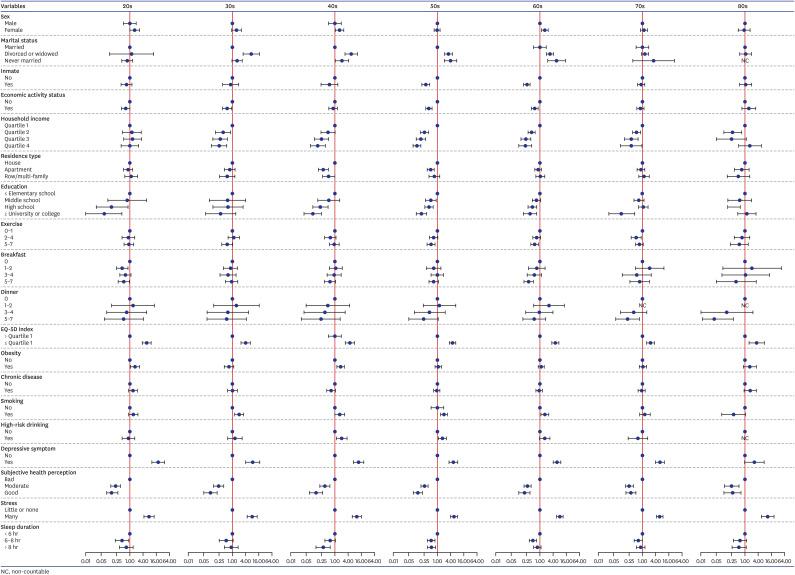
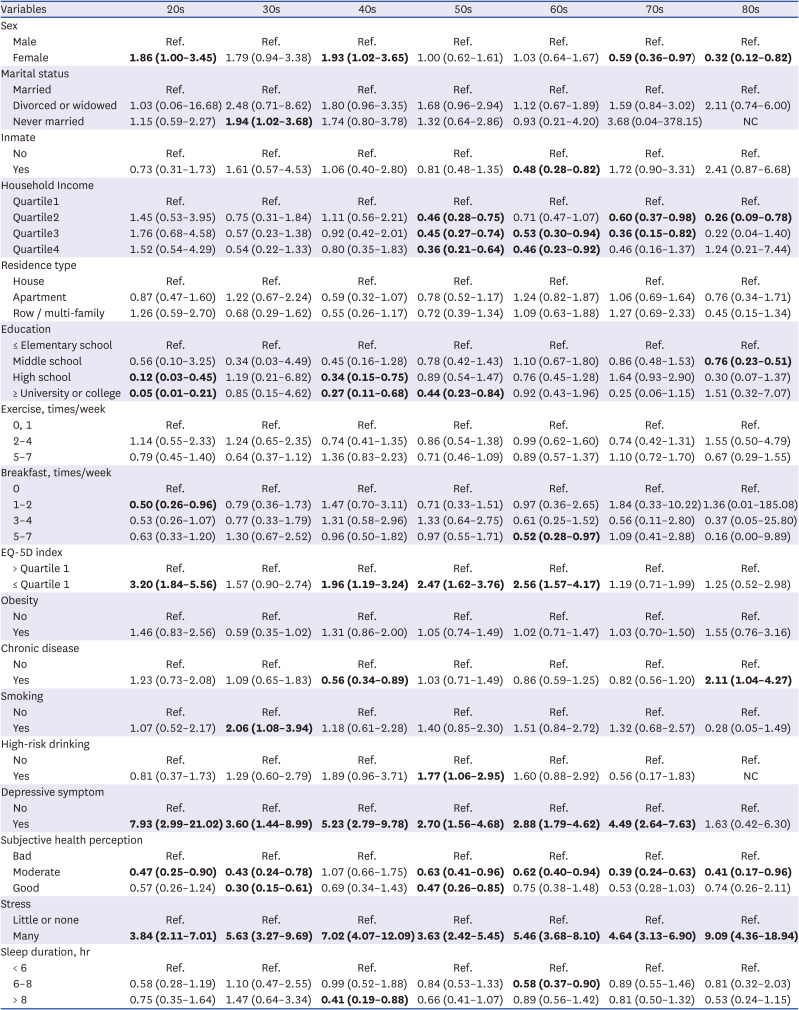
Table 2 shows the results of the multiple logistic regression analysis. Stress was found to significantly affect SI in all age groups. Depression continued for two weeks, except for those in their 80s, which had a significant effect, and subjective health perception had a significant effect, except for those in their 40s. The greatest influence of SI was found in the case of high stress in 80-year-olds or above (OR, 9.09; 95% CI, 4.36–18.94), depression for two weeks for those in their 20s (OR, 7.93; 95% CI, 2.99–21.02), and those who had a good subjective health perception in their 30s (OR, 0.30; 95% CI, 0.15–0.61). Women in their 20s and 40s were more likely to consider suicide than men, and among them, women in their 40s (OR, 1.93; 95% CI, 1.02–3.65) had the highest rate of SI. Conversely, the probability of SI decreased among those in their 70s and 80s; among them, women in their 80s (OR, 0.32; 95% CI, 0.12–0.82) had the lowest SI. Similar to the results in Fig. 3, except for those in their 20s and 80s, the higher the household income level, the lower the probability of contemplating suicide. In particular, the higher the household income level among those in their 50s, the lower the probability of contemplating suicide. Compared to individuals with elementary school graduation or lower, the probability of SI was lower for those in their 20s, 40s, and 50s when they graduated from college or higher and the lowest for those in their 20s (OR, 0.05; 95% CI, 0.01–0.21). In the 20s, 40s, 50s, and 60s, EQ-5D was associated with SI in the bottom 25% and was most clearly observed in the 20s (OR, 3.20; 95% CI, 1.84–5.56). In addition, those in their 30s who were smoking or unmarried; those in their 40s who were high school graduates, had chronic diseases, and slept for more than eight hours; and those in their 50s who were in high-risk drinking groups showed statistically significant results. Moreover, those in their 60s who had inmates, had breakfast 5–7 times per week, and slept for 6–8 hours, as well as those in their 80s who had chronic disease, showed statistically significant results.
Table 2
Multiple logistic regression for suicidal ideation according to the age group
Supplementary Figs. 1 and 2 shows the results of univariate logistic regression on the factors of suicidal ideation by age group in males and females. Two peculiar points can be found. First, the possibility of suicidal ideation according to the presence or absence of economic activity was significantly lower in the economically active group among men in their 30s, 50s, and 60s, but no significant result was found in women. In addition, women in their 40s to 60s high-risk drinking group had a higher possibility of suicidal ideation than non-high-risk drinking group, and no significant results were found in men. Stratified by gender, multiple logistic regression analysis was performed according to age. The results of multiple logistic regression were nearly identical to those of univariate logistic regression (Supplementary Tables 2 and 3). In male, EQ-5D, depression, and stress had an effect in most age groups, but depression had no effect in men in their 30s and 50s. In female, depression, subjective health perception, and stress affected most age groups. However, depression and subjective health perception did not affect those in their 80s, and subjective health perception did not affect people in their 40s. In multiple logistic regression analysis, c-statistics was over 0.8 in all age groups, regardless of gender.
DISCUSSION
The idea-to-action framework, which is the basis of many theories regarding suicide, explains its process from SI to suicide attempt and suicide completion. This demonstrates that there are distinct stages that mark the development of SI and its progression to a fatal suicide attempt. However, all theories of suicide affirm that not all suicide ideators attempt suicide. For example, only 1 in 31 suicide ideators in the United States attempted suicide.33 This suggests that suicide attempts can be prevented if a policy or project, with a good understanding of the nature of the process and stages of suicide, intervenes with and assists suicide ideators. In this study, factors related to SI were identified according to sex and age group.
Logistic regression analysis was used because the primary purpose of this study was to confirm the factors affecting SI according to age in the general population and derive and interpret meaningful results. Logistic regression analysis is the most conventional statistical method for developing risk-prediction models. The predictive effect of a predictor variable can be expressed simply and descriptively, and multiple variables can be determined and used to make predictions. However, recent studies with similar content to our research topic mainly dealt with predictive models using machine learning or deep learning. Many studies predict SI using data from the general population.34353637 If a predictive model is built using the artificial intelligence (AI) method, it is possible to classify SI as “yes/no” by deriving a probability value for predicting the outcome. However, it is impossible to interpret and explain the process by which the result value is produced and the factors resulting from it. This may be a limitation of research using AI, and our study using only logistic regression analysis has the advantage of compensating for the shortcomings of AI research. To indirectly compare our research results with the AI research model, the importance of the variables that affect the prediction of the results in the AI model can be confirmed. Ryu et al.36 reported that depression, anxiety, and stress were important characteristics of SI; similarly, Oh et al.37 showed that stress, depressive symptoms lasting more than two weeks, and EQ-5D results were essential factors of SI. In our study, when there was a lot of stress (β = 0.78; OR, 4.71; 95% CI, 3.94–5.64) and depression for more than two weeks (β = 0.67; OR, 3.83; 95% CI, 2.98–4.92), individuals belonging to the bottom 25% of the EQ-5D index (β = 0.39; OR, 2.18; 95% CI, 1.78–2.69) had the greatest influence on whether SI occurred. In addition, variables such as education level38 and economic level,39 which have been reported to impact suicide in several previous studies, were shown to be equally related to SI. As such, in our study, we provided validity through numerical values for areas that AI research could not identify and influence.
The significant findings of our study are as follows: The rate of SI differed according to age; after the age of 50, the rate of SI increased. As for the results according to sex, the SI rate of women was high in all age groups. According to the regression analysis, the possibility of SI was significantly higher in women in their 20s and 40s than that in men. In contrast, it was considerably lower in individuals in their 70s and 80s. Furthermore, for all age groups, psychological factors such as depression, stress, and quality of life were strongly related to SI, and the factors related to SI differed among age groups.
The probability of SI by age group was low in individuals in their 20s, 30s, and 40s compared to those in their 50s, and gradually increased in those in their 60s, 70s, and 80s. The increase in SI rate as one’s age increased after 50 years was different from a study that investigated SI over the age of 50 in 20 European countries. In Europe, the highest rate of SI was found among those aged 50–64 years, and the rate of SI decreased with increasing age among those aged ≥ 65 years. This is thought to represent the aging problem that occurs as life expectancy increases in Korea,1 which has the fastest aging rate among OECD countries. In Korea, the traditional extended family era has developed into a nuclear family one, and single-person households are increasing in modern times.40 This has emerged as a social problem of loneliness and depression among older adults living alone because of the lack of a sense of belonging and bonding as a family member. In addition, the older group, whose income is relatively low compared to other age groups, has ranked first in the poverty rate in older adults among OECD member countries.1 Older adults suffer from economic problems, but the social protection that can support them is weak. The receipt rate of basic pension to guarantee a specific part of the income of older adults fell to 66.8% in 2014, 65.5% in 2016, and 66.2% in 2019.41 Loneliness, health issues, and poverty of older adults due to an increase in the aging population is a problem that the government must solve.
In the “Five-Year National Suicide Death Analysis Results Report” that analyzed Korea’s data from 2013 to 2017, the rate of SI was the lowest among those in their 30s and 40s, which is similar to our study.22 On the other hand, a survey of Australians in their 20s, 40s, and 60s found that those in their 20s had the highest SI, and those in their 60s had the lowest SI rate.42
Second, the SI rate of all individuals in this study was nearly double that of women compared to men. In an article that studied SI in Korea from 1995 to 2005, the rate of SI among women was higher than that of men in all age groups.43 This was similar to a study on SI from 2013 to 2019, which found that women still had a high SI rate.
Meanwhile, as a result of analyzing the relationship between age and SI in the multivariate logistic regression analysis controlling for other variables, women in their 20s and 50s were more likely to have SI than men, and women in their 60s and 80s had lower SI. On the other hand, in European studies of middle-aged people over 50 years and those over 75 years, women were more likely to have SI,71544 which was different from the results of this study. However, as in this study, it was challenging to determine SI by age because the age groups were not analyzed separately.
According to the results of our study, the possibility of SI among women was higher than that of men until the age of 50 and lower than that of men aged 60 years, suggesting that women after the age of 60 were less likely to experience SI than men. In addition, since each age group had different historical experiences, suicidal behaviors may appear differently for each age group.
Third, this study identified the factors affecting SI characteristics by sex and age. First, the differences in SI factors according to sex were as follows: In our study, the younger the age of the women, the higher the likelihood of SI. According to data from the National Health Insurance Corporation of Korea, the group with the highest increase in the number of people treated for depression in the first half of 2021 compared to the first half of 2017, comprised women aged 15–34 years. In the first half of 2021, the age group with the highest number of patients receiving treatment for depression involved women aged 25–29 years.45 In addition, Koreans in their 20s and 30s had the lowest happiness index; among them, women in their 20s were the most unhappy.46 For women in their 20s, the suicide rate increased by more than 15% from 2017 to 2020, and the increase rate was about 25% in 2019, the highest of any other group.
Social and economic factors also explain this trend. Currently, young women comprise a generation that has entered society at a higher rate than men compared to the previous generation, and they have a complex issue with being the youngest at their workplace, including the difficulties they face as women.47 The 20s involve an age at which they start their life as an adult. They face much trouble getting jobs, dating, and marrying, and they have a lot of worries regarding life. In particular, youth unemployment is increasingly becoming a social problem. In addition, the proportion of the economically inactive population among college graduates in Korea is 20.3%, the third highest among 37 OECD countries.48 In our society, men in their 20s also suffer from the same problems. However, they still have a grace period before entering social competition compared to women because they have the task of serving in the military. Therefore, it is thought that the possibility of SI among women in their 20s is relatively high in this social environment.
Most women in their 30s take on housework and childcare while getting married or having a job and social life. The primary responsibility for child-rearing and housework is still being passed on to women.49 Many married women with young children experience stress or depression related to the burden of child-rearing.50 Women with the youngest children aged 2–3 years have the highest SI.51 In our study, women under the age of 50 were more likely to have suicidal thoughts than men. We suggest that it could be study relation to attributed stress and depression caused by their burden of raising children and SI among women in further study.
After reaching 60, women become relatively relieved from the burdens of child-rearing, housework, daughter-in-law duties, and work life. Meanwhile, children emotionally need their mothers rather than fathers at home, wanting to talk to them. This is in contrast with men, whose roles in the household decrease as they age. For this reason, it is thought that SI decreases from the age of 60 years, when the burden on women begins to fall.
Looking at the factors influencing male and female suicidal ideation, first, the possibility of suicidal ideation according to the presence or absence of economic activity was not significant in females but significant in economically active males in their 30s, 50s, and 60s. Their suicidal ideation was found to be low. It is judged that this shows that men feel the burden of household responsibility more heavily. Similar to our results, an article that studied the relationship between unemployment and suicidal ideation revealed that men were more likely to have suicidal thoughts if they were unemployed. 52 Cleary said that according to the traditional Korean patriarchal social culture, men appear to be more affected by financial stress and psychological effects of job loss.53
Also, the results of this study suggest that high-risk drinking appears to have a more significant impact on suicidal ideation in women. In a study of alcohol and suicide, alcohol abuse occurs more often in men, but suicide-related behaviors due to alcohol abuse are more common in women.54 This result indicates that women are more vulnerable to adverse health consequences of chronic heavy drinking than men.5556 Moreover, both men and women showed significantly similar trends in depression, stress, subjective health perception, and EQ-5D Index variables, which are known to be highly related to suicidal ideation.
Next, looking at the differences in factors of SI by age, one of the results that should be considered in our study is the relationship between SI and income. In the multivariate regression analysis that controlled for other variables, overall, the higher the income quintile for all age groups, the lower the likelihood of SI. Furthermore, the relationship with SI had borderline statistical significance in people over 50 years of age, who had a higher probability of SI than in other age groups. In particular, it was clearly seen that the likelihood of SI decreased as income increased among those in their 50s.
In Korea, people in their 50s still demand stable income because of their children’s education and marriage. However, unemployment due to the foreign exchange crisis; economic crisis caused by COVID-19; and job insecurity, such as irregular employment, do not guarantee a stable income for families. During this period, many children prepare for employment before becoming independent. It is also a time when a lot of revenue is needed because of preparations for children’s marriage. Since there are many cases in which stable income is not guaranteed during this period, it is thought that income significantly affects SI in this age group.
The relationship between income and SI in the 60s also showed that the higher the payment, the lower the likelihood of SI. According to the 2016 household income by the number of household members announced by the National Assembly Budget Office, single-person households in their 60s earned only half of their peer-year income and, in many cases, became single-person households due to bereavement.5758 Among our study participants, 14% of those in their 60s were in single-person families, and it can be inferred that their income was relatively lower than that of their peers. The results of our study showed that the possibility of SI in those in their 60s living with a family was lower than that of single-person households with individuals in their 60s. Income is thus considered to affect the possibility of SI.
Participants who reported good subjective health perception in all age groups were less likely to have SI. Although many studies have targeted older adults, each study clearly shows the relationship between personal health status and SI.596061 The younger the age, the more the better subjective health perception lowers the possibility of SI. The 20s and 30s comprise the healthiest times of adulthood. Thinking that individuals are not in good health during this period may pose a clinical or medical problem, either physically or mentally. It can be seen that the fewer these worries that can act as stressors, the lower the likelihood of SI.
The relatively weak influence for those in their 70s and 80s is that all the older adults who enter old age experience a weakening of their physical functions. As a result, underlying diseases can easily occur. It is thought that since the weakening of health status is perceived as a natural aging process among older adults, they do not take it more seriously emotionally than those belonging to young adulthood.
In our study, the relationship between sleep duration and SI was lower in the group that slept for more than six hours for all age groups, except for those in their 30s. This was similar to a study of adults, which found that those who slept for less than six hours were 1.33 times more likely to commit suicide,62 and those who slept for more than seven hours in another study had lower SI than those who did not.63 The relationship between sleep time and SI can be found not only in the accumulation of fatigue from simply not getting enough sleep but also in the quality of sleep. It has been found that SI increases in people with short sleep duration and low-quality sleep due to insomnia or nightmares.64 According to the American Sleep Society, depressive symptoms can cause sleep disorders; conversely, sleep disorders can contribute to depressive symptoms.65
According to the results of this study, factors related to age-specific SI had essential outcomes. The factors that strongly influenced SI in most age groups were depression, stress, and quality of life. It has been found in many previous papers that depression, stress, and low quality of life are risk factors for SI,81011151618192343 showing a similar pattern to our study. Depression is the most common suicide-related risk factor,8 and stress directly affects SI, having a positive correlation with depression.66 Depression begins in various stressful situations and can lower the quality of life. Therefore, to reduce depression, a systematic program on stress management for risk groups is needed at the government level.
People can experience SI for several reasons such as unstable income, loneliness, or health problems. In this study, even after controlling for psychological factors such as depression and stress, which are most related to SI, demographic, economic, and health behavior variables remained significant in the regression analysis. In particular, we found that income—an economic variable—is an essential factor influencing the SI of older adults in Korea. Therefore, the government should establish policies to reduce the suicide rate among this population in Korea, which has the highest OECD poverty rate. Programs and social initiatives are also required to ensure stable employment for the young and old population, including relieving stress and depression for women.
The Korean government has made great efforts to dispel the stigma of having the highest suicide rate among the OECD countries. Following the National Health Promotion Act, the National Health and Nutrition Survey, a nationwide survey that calculates national statistics on health and nutrition for 10,000 Korean citizens every year, including items of SI, suicide plans, and suicide attempts, is calculated statistically. Accordingly, each local government has been operating various suicide prevention programs to prevent suicide among older adults.67 In 2018, the suicide prevention hotline 1393 was opened by the government for those who felt suicidal.68 Furthermore, since 2014, involving the current status of suicide in Korea, the White Paper on Suicide Prevention has been published so that practitioners related to suicide prevention can use it to promote projects appropriate to each region’s circumstances and conditions.69 Rather than seeing suicide as a problem for a single population group, classifying the population group by sex and age and understanding the characteristics that fit each group is necessary. Furthermore, implementing differentiated policies and projects presumes that Korea will be one step closer to reducing its suicide rate.
Our study was non-clinical and resulted from a general population survey, in which a large sample of 18,336 people was analyzed. Our results were derived after studying the general population and not a specific disease, age group, or sex. Our findings are thus expected to provide vital information for various applications. However, since it was a cross-sectional study, there is a limitation in that it cannot infer the direction of the relationship between SI and each variable. SI shows various aspects, ranging from a passive level of simply wishing not to wake up in the morning to specifically planning suicide. Harmer noted that all healthcare professionals must thoroughly evaluate, monitor, and document the patterns, intensity, characteristics, and effects of SI on an individual.33 However, this study used a secondary questionnaire with questions about SI in a binary yes/no fashion, which may lack validity or reliability. Therefore, it was impossible to analyze the factors that could vary according to the pattern. In future research, we hope to study risk factors according to the intensity of SI by using a questionnaire that can evaluate SI in more depth rather than simply in a binary yes/no fashion. Related to suicidality, there were limited variables and analysis for the biological aspects and psychiatric disorders. There was a variable related to ‘mental problem counseling experience’ as a variable related to psychiatric disorders. Still, this variable could not be used in our study because it was deleted in other periods. Due to the limited variables in the raw data, we could not observe other biological variables.
SI is not simply affected by a single factor but may be influenced by multiple factors. A combination of factors such as personality traits, stress or ability to cope with various events, social support, and mental or physical limitations influence suicidal behavior. If we can see such a complex mechanism in a simpler schematic view, it would help lower serious suicide rates in Korea. As per our study’s findings, identifying the factors that have a more decisive influence on SI by classifying the subjects by age and sex will make an outstanding contribution to the systematic planning and execution of management systems and programs to prevent suicide. The reason why we conducted this study was to find the factors related to SI according to gender and age from the health perspective, not the clinical point of view, and use it as reference material for prevention. Our results will be used as reference materials for psychiatry, family medicine, and preventive medicine.
 XML Download
XML Download