

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Hypertension is known to be a prevalent risk factor for cardiovascular disease and a common chronic disease in Korea, affecting nearly 29% of adults aged 20 years and older.1 However, there is controversy over the diagnostic criteria for hypertension, with differences between the United States (US) and other countries.2345 The Systolic Blood Pressure Intervention Trial (SPRINT) study,6 which used automated unattended office blood pressure (aUAOBP), led to changes in the US definition of hypertension.
Accurate blood pressure (BP) measurement is essential for the diagnosis and management of hypertension. While the Korean hypertension guidelines recommend auscultatory attended office blood pressure (ausAOBP) and automated attended office blood pressure (aAOBP) as the standard measurement methods,23 limitations in clinical practice suggest that out-of-office BP measurements, such as home blood pressure (HBP) and 24-hour ambulatory blood pressure (ABP), may be useful, and aUAOBP measurement can be considered when HBP or 24-hour ABP cannot. Several recent studies reported comparisons between aUAOBP and attended office BP, HBP, and 24-hour ABP measurements,78910 but there were differences in the study results. Studies in Korean population were scarce,1112 and none of them used all five BP measurement methods.
Thus, the aim of this study was to evaluate differences in BP measurements by different methods, including ausAOBP and aAOBP, aUAOBP, HBP, and 24-hour ABP in the Korean population, to identify the factors influencing differences in BP measurements, and assess the prevalence of hypertension phenotypes.
METHODS
Study population
This study constitutes a prospective, single-center study designed to compare the differences in BP readings between various BP measurement methods. Sequentially recruited from individuals visiting the outpatient cardiology department at Kangbuk Samsung Hospital, participants aged 19 or older, irrespective of any history of hypertension, provided informed consent to take part in this study. We excluded patients who were undergoing dialysis, pregnant women, and individuals whose left and right arm systolic blood pressure (SBP) and diastolic blood pressure (DBP) differed by more than 20 mmHg and 10 mmHg, respectively. Of the 209 individuals who agreed to participate from April 2019 to June 2022, 26 were excluded because they withdrew consent or had incomplete BP measurements. Finally, 183 participants were analyzed for the study.
Data collection
Medical history, use of antihypertensive medication, smoking habits (never, former, or current smoker), exercise frequency (minutes per week) and alcohol consumption (times per week) were assessed. Body mass index (BMI) was calculated as weight (in kg) divided by height (in m2). Waist circumference was determined at the midpoint between the lowest rib and the iliac crest. Diabetes mellitus was defined as fasting plasma glucose ≥ 126 mg/dL, hemoglobin A1c ≥ 6.5%, current diagnosed diabetes or use of antidiabetic medication. Atherosclerotic cardiovascular disease was defined as clinically established coronary heart disease, stroke, or peripheral arterial diseases. Menopause in women was defined as the absence of menstruation for more than 1 year, whether natural or surgical.
BP measurements
The general BP measurement methods were based on the latest Korean Society of Hypertension guidelines.23 The sequence of the BP measurement methods used to obtain BP measurements is shown in Supplementary Fig. 1.
ausAOBP
ausAOBP measurements were taken without smoking or consuming alcohol or caffeine within 30 minutes and after resting for at least 5 minutes in a quiet environment. ausAOBP readings were taken three times by a physician using a sphygmomanometer (OMRON HEM-907; OMRON Healthcare, Tokyo, Japan) at two-minute intervals in a seated position with the back supported and the upper arm at heart level. The Korotkoff’s I and V sounds were considered SBP and DBP, respectively. BP was measured in both arms at baseline and subsequently in the arm with the higher BP. The average value of the three measurements was defined as ausAOBP.
aAOBP
Preparation before BP measurement was the same as above. aAOBP was measured 5 minutes after ausAOBP measurement and at 2-minute intervals with the same device (OMRON HEM-907; OMRON Healthcare). The average value of the three measurements was defined as aAOBP.
aUAOBP
aUAOBP measurements were taken 5 to 10 minutes after aAOBP measurements using the same device (OMRON HEM-907; OMRON Healthcare). Based on the methods used in the SPRINT study,6 aUAOBP was measured three consecutive times at 2-minute intervals after 5 minutes of rest while the subject was alone in a quiet and separate room without medical staff. The average value of the three measurements was used as aUAOBP.
ABP
ABP was measured using a 24-hour ambulatory BP monitor (Mobil-O-GraphNG; IEM GmbH, Aachen, Germany) for at least 20 hours, referring to the sleep time recorded in the participant’s diary. BP was measured at 30-minute intervals during the day and at one-hour intervals during the night. Daytime, nighttime, morning, and average BP were assessed.
HBP
HBP measurement was started on the day of the office BP measurement, with an automated HBP sphygmomanometer (OMRON HEM 7120; OMRON Healthcare) after stabilization for at least 2 minutes in the sitting position before breakfast (before antihypertensive medication in hypertensive patients) and before going to bed at night. BP was measured twice at 2-minute intervals by measuring it for one week, and the average value was defined as HBP. Mean HBP was defined as the average of morning and evening HBPs.
Definition of hypertension
In accordance with the current hypertension guidelines,234 office hypertension was characterized by a mean SBP/DBP equal to or greater than 140/90 mmHg, as assessed by ausAOBP and aAOBP. Out-of-office hypertension was defined as daytime ABP or mean HBP equal to or greater than 135/85 mmHg. Unattended office hypertension was divided into two categories based on mean SBP/DBP values equal to or greater than 140/90 mmHg (aUAOBP-1) and equal to or greater than 135/85 mmHg (aUAOBP-2). White-coat hypertension was defined as ausAOBP ≥ 140/90 mmHg but daytime ambulatory BP and mean home BP < 135/85 mmHg, and masked hypertension was defined as the opposite. In hypertensive patients taking antihypertensive medication, uncontrolled hypertension was defined as ausAOBP ≥ 140/90 mmHg and daytime ABP and mean HBP ≥ 135/85 mmHg; white-coat uncontrolled hypertension was defined as ausAOBP ≥ 140/90 mmHg and daytime ABP and mean HBP < 135/85 mmHg; masked uncontrolled hypertension was defined as ausAOBP < 140/90 mmHg and daytime ABP and mean HBP ≥ 135/85 mmHg; controlled hypertension was defined as ausAOBP < 140/90 mmHg and daytime ABP and mean HBP < 135/85 mmHg.
Statistical analysis
Previous studies in both hypertensive and non-hypertensive subjects reported that the difference between ausAOBP, aAOBP and aUAOBP values ranged from 3 to 16 mmHg.91112 To determine the required sample size, a 5% difference in SBP between the two measurements was assumed, and the minimum number of participants required to achieve 80% statistical power and a 5% significance level was calculated to be 174 subjects, with a total of 190 subjects recruited, considering a drop-out rate of 10%.
The data collected were presented as means (standard deviations) for continuous variables and numbers (percentages) for categorical variables. Descriptive statistics were used to analyze the distribution of BP differences between the different measurements, and the paired t-test was used to compare the mean BP values. Bland and Altman plots were used to assess the agreement between paired BP values, while Pearson’s correlation analysis was used to assess the correlation between paired BP values according to different BP measurements. Multivariable regression analysis was performed to determine the variables influencing the disparity in BP between paired BPs, with the model adjusted for age, sex, and those variables with a univariate relationship (P < 0.150). Prespecified subgroup analysis was conducted based on the presence or absence of hypertension.
Statistical significance was set at a two-tailed P value < 0.05 using STATA version 16.1 (StataCorp LP, College Station, TX, USA).
RESULTS
Baseline characteristics
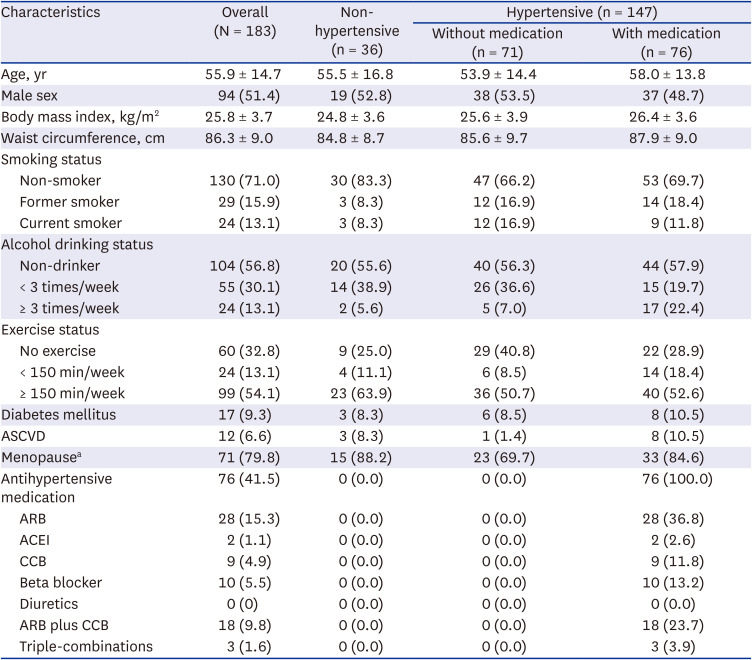
Of a total of 183 participants, 36 were normotensive, and 147 were hypertensive, with a mean age of 55.9 ± 14.7 years and 51.4% were male (Table 1). Of the 147 hypertensive patients, 76 were prescribed antihypertensive medications. The prevalence of current smoking and alcohol consumption (≥ 3 times/week) was 13.1%, and that of diabetes mellitus and atherosclerotic cardiovascular disease was 9.3% and 6.6%, respectively.
Table 1
Baseline characteristics of the study population
Comparison of BPs according to different BP measurement
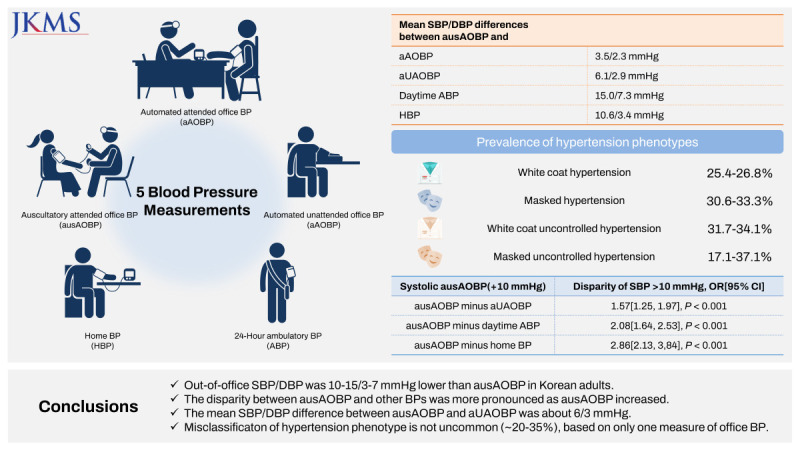
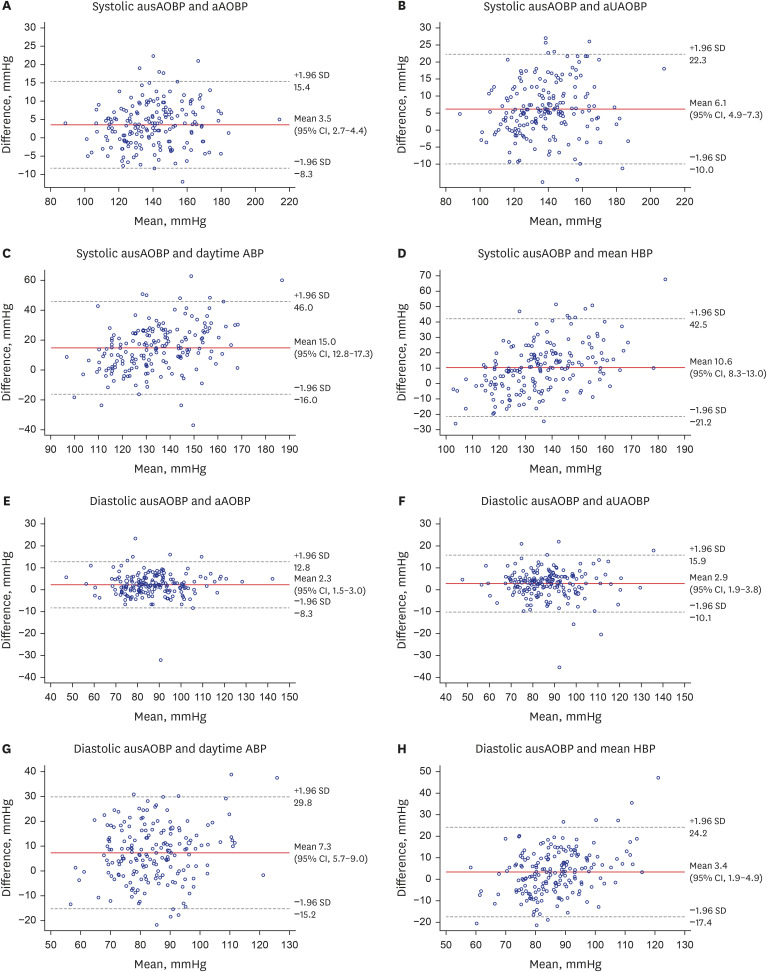
In the total population, the mean systolic/diastolic ausAOBP, aAOBP, aUAOBP, daytime ABP, and mean HBP were 141.2 ± 19.8/88.2 ± 13.8 mmHg, 137.6 ± 19.0/85.9 ± 13.8 mmHg, 135.1 ± 18.7/85.3 ± 14.0 mmHg, 129.3 ± 15.3/83.7 ± 13.2 mmHg, and 130.5 ± 13.2/84.8 ± 10.2 mmHg, respectively (Table 2). The systolic/diastolic ausAOBP values were significantly higher than the systolic/diastolic aAOBP, aUAOBP, daytime ABP, 24-hour ABP, and HBP values. These findings in the prespecified subgroup analysis based on the presence or absence of hypertension were more pronounced in hypertensive subjects not taking antihypertensive medication (Table 2). The limits of agreement for systolic ausAOBP were 15.4 and −8.3 mmHg for aAOBP, 22.3 and −10.0 mmHg for aUAOBP, 46.0 and −16.0 mmHg for daytime ABP, and 42.5 and −21.2 mmHg for mean HBP (Fig. 1A-D). Those in diastolic ausAOBP were 12.8 and −8.3 mmHg for aAOBP, 15.9 and −10.1 mmHg for aUAOBP, 29.8 and −15.2 mmHg for daytime ABP, and 24.2 and −17.4 mmHg for mean HBP (Fig. 1E-H). The mean differences (95% confidence interval) between ausAOBP and aAOBP, aUAOBP, daytime ABP, and mean HBP were 3.5 (2.7–4.4)/2.3 (1.5–3.0) mmHg, 6.1 (4.9–7.3)/2.9 (1.9–3.8) mmHg, 15.0 (12.8–17.3)/7.3 (5.7–9.0) mmHg, and 10.6 (8.3–13.0)/3.4(1.9–4.9) mmHg, respectively (Fig. 1). The distributions of BP differences according to different BP measurements are shown in Supplementary Fig. 2.
Table 2
Comparison of BPs according to different BP measurement methods
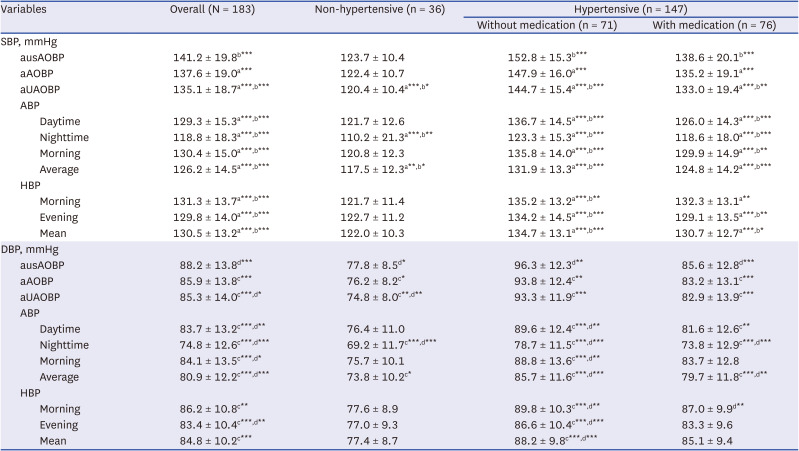
Paired sample t-tests were used to compare the mean difference between BP values according to different BP measurement methods.
BP = blood pressure, SBP = systolic blood pressure, ausAOBP = auscultatory attended office blood pressure, aAOBP = automated attended office blood pressure, aUAOBP = automated unattended office blood pressure, ABP = ambulatory blood pressure, HBP = home blood pressure, DBP = diastolic blood pressure.
‘a’ and ‘b’ are comparisons of the difference of mean values between systolic ausAOBP and other BPs and between aAOBP and other BPs, respectively.
‘c’ and ‘d’ are comparisons of the difference of mean values between diastolic ausAOBP and other BPs and between aAOBP and other BPs, respectively.
*P < 0.05, **P < 0.01, ***P < 0.001.
Fig. 1
Bland-Altman plots for the comparison between SBP and DBP according to different BP measurement methods.
(A) Systolic ausAOBP and aAOBP, (B) systolic ausAOBP and aUAOBP, (C) systolic ausAOBP and daytime ABP, (D) systolic ausAOBP and mean HBP, (E) diastolic ausAOBP and aAOBP, (F) diastolic ausAOBP and aUAOBP, (G) diastolic ausAOBP and daytime ABP, and (H) diastolic ausAOBP and mean HBP. The middle solid line depicts the mean difference (95% CI) and the top and bottom dotted lines represent the limits of agreement (± 1.96 SD).
SBP = systolic blood pressure, DBP = diastolic blood pressure, BP = blood pressure, ausAOBP = auscultatory attended office blood pressure, aAOBP = automated attended office blood pressure, aUAOBP = automated unattended office blood pressure, ABP = ambulatory blood pressure, HBP = home blood pressure, SD = standard deviations, CI = confidence interval.
Disparity between paired BP values according to different BP measurement
ausAOBP values were highly correlated with aAOBP (r = 0.954, P < 0.001) and aUAOBP (r = 0.914, P < 0.001) values, but less so with office BP and out-of-office BP (r = 0.5’s–0.6’s, P < 0.001) (Supplementary Table 1). In the subgroup analysis based on the presence or absence of hypertension, weak correlation coefficients between systolic AOBP and out-of-office BP were observed in non-hypertensive subjects (Supplementary Table 2).
Multivariable regression analysis showed that only increasing systolic ausAOBP was significantly associated with an increase in the absolute difference between systolic ausAOBP and aUOBP (β = 0.141, P < 0.001), daytime ABP (β = 0.521, P < 0.001), and HBP (β = 0.598, P < 0.001) (Table 3). Furthermore, an SBP difference of > 10 mmHg between ausAOBP and aUAOBP, daytime ABP, and mean HBP was only associated with increasing systolic ausAOBP (odds ratio [95% CI], 1.036 [1.017–1.056], 1.077 [1.052–1.103], and 1.109 [1.076–1.143], respectively, Table 3). The differences between diastolic ausAOBP and BPs taken by different BP measurement methods were similar to the SBP results above (Table 4).
Table 3
Multivariable regression analysis of factors affecting SBP differences between ausAOBP and other BPs
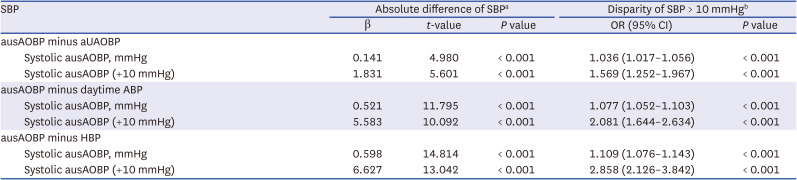
All multivariable models were adjusted for age, sex, and the variables with a univariate relationship of P < 0.150.
SBP = systolic blood pressure, ausAOBP = auscultatory attended office blood pressure, BP = blood pressure, OR = odds ratio, CI = confidence interval, aUAOBP = automated unattended office blood pressure, ABP = ambulatory blood pressure, HBP = home blood pressure.
aAbsolute difference between paired BP values.
bDifference between paired BP values of more than 10 mmHg.
Table 4
Multivariable regression analysis of factors affecting DBP differences between ausAOBP and other BPs
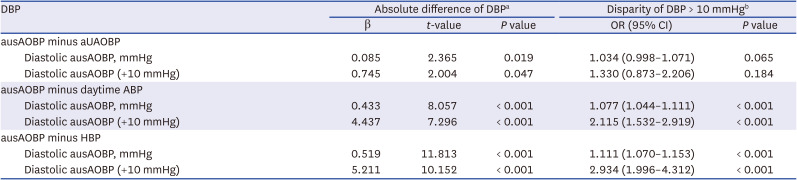
All multivariable models were adjusted for age, sex, and the variables with a univariate relationship of P < 0.150.
DBP = diastolic blood pressure, ausAOBP = auscultatory attended office blood pressure, BP = blood pressure, OR = odds ratio, CI = confidence interval, aUAOBP = automated unattended office blood pressure, ABP = ambulatory blood pressure, HBP = home blood pressure.
aAbsolute difference between paired BP values.
bDifference between paired BP values of more than 10 mmHg.
Prevalence of the hypertension phenotype
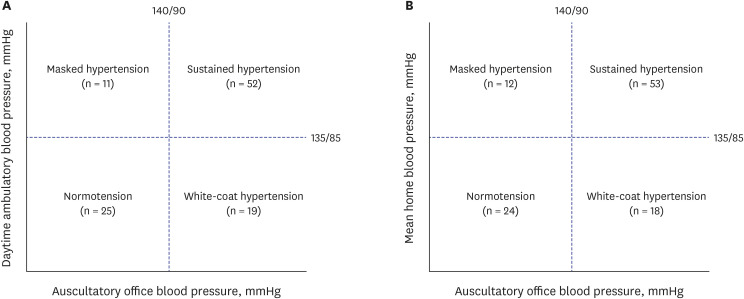
In the 107 subjects not taking antihypertensive medication, the prevalence of hypertension according to different BP measurement methods was 71 (66.4%) for ausAOBP, 57 (53.3%) for aAOBP, 52 (48.6%) for aUAOBP-1, 68(63.6%) for aUAOBP-2, 63(58.9%) for daytime ABP, and 65 (60.7%) for mean HBP (Fig. 2). Among 71 hypertensive patients based on ausAOBP levels (≥ 140/90 mmHg), the prevalence of white-coat hypertension was 19 (26.8%) for daytime ABP (< 135/85 mmHg) and 18 (25.4%) for mean HBP (< 135/85 mmHg) (Fig. 3A). In contrast, the prevalence of masked hypertension among the 36 non-hypertensive subjects based on ausAOBP levels (< 140/90 mmHg) was 11 (30.6%) for daytime ABP (≥ 135/85 mmHg) and 12 (33.3%) for mean HBP (≥ 135/85 mmHg) (Fig. 3B). The prevalence of hypertension phenotypes based on aAOBP, daytime ABP and mean HBP is shown in Supplementary Fig. 3. The prevalence of white-coat hypertension based on aAOBP (17.5–21.1%) was lower than that based on ausAOBP. In the 76 hypertensive patients taking antihypertensive medication, the prevalence of white-coat uncontrolled and masked uncontrolled hypertension was 34.1% for daytime ABP and 31.7% for HBP, and 17.1% for daytime ABP and 37.1% for mean HBP, respectively (Supplementary Fig. 4).
Fig. 2
Prevalence of hypertension according to different blood pressure measurement methods in 107 individuals not taking antihypertensive medication.
The hypertension cutoff level was defined as ≥ 140/90 mmHg for ausAOBP, aAOBP, and aUAOBP-1 and ≥135/85 mmHg for aUAOBP-2, daytime ABP, and mean HBP.
ausAOBP = auscultatory attended office blood pressure, aAOBP = automated attended office blood pressure, aUAOBP = automated unattended office blood pressure, ABP = ambulatory blood pressure, HBP = home blood pressure.
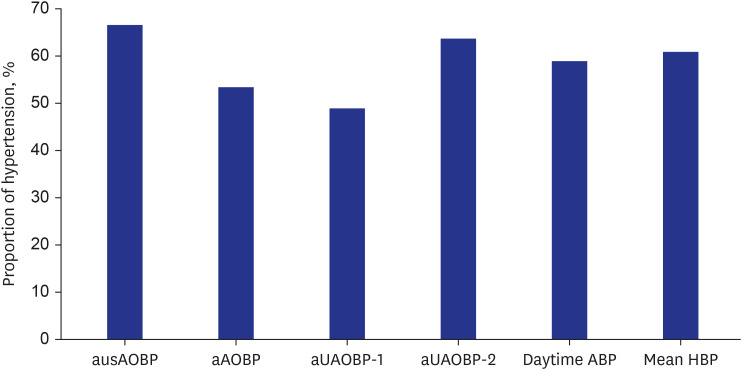
Fig. 3
Prevalence of hypertension phenotypes based on ausAOBP, daytime ABP, and mean HBP in 107 individuals not taking antihypertensive medication.
(A) Based on ausAOBP and daytime ABP. (B) Based on ausAOBP and mean HBP. Sustained hypertension was defined as ≥ 140/90 mmHg ausAOBP and ≥ 135/85 mmHg daytime ABP and mean HBP. White-coat hypertension was defined as ≥ 140/90 mmHg ausAOBP and < 135/85 mmHg daytime ABP and mean HBP. Masked hypertension was defined as < 140/90 mmHg ausAOBP and ≥ 135/85 mmHg daytime ABP and mean HBP. No hypertension was defined as < 140/90 mmHg ausAOBP and < 135/85 mmHg daytime ABP and mean HBP.
ausAOBP = auscultatory attended office blood pressure, ABP = ambulatory blood pressure, HBP = home blood pressure.
DISCUSSION
This study showed that out-of-office SBP/DBP measurements, such as daytime ABP and mean HBP, were 10–15/3–7 mmHg lower than ausAOBP in Korean adults, and the mean SBP/DBP difference between ausAOBP and aUAOBP were about 6/3 mmHg. These differences between ausAOBP and other BPs were associated with increasing BP and were more pronounced in hypertensives than in non-hypertensives. The prevalence of white-coat hypertension and masked hypertension was 25.4–26.8% and 30.6–33.3%, respectively, and that of white-coat uncontrolled hypertension and masked uncontrolled hypertension was 31.7–34.1% and 17.1–37.1%, respectively.
Although the recent hypertension guidelines state that ausAOBP is still the standard method for measuring BP, office BP measurements may not always accurately reflect a patient’s true BP outside of a clinical setting. This could be due to several factors, including observer bias, the measurement technique, and the white-coat effect. As recommended in the 2022 focused update of the 2018 Korean Hypertension Society Guidelines,3 out-of-office BP measurements are becoming increasingly important in clinical practice as they can provide additional information about a patient’s BP control and help to identify patients with white-coat hypertension or masked hypertension.
Previous studies reported different results between ausAOBP and other office BP measurements, aAOBP and aUAOBP,13141516 and recent meta-analyses also showed inconsistent results.8910 However, because most of these studies were conducted in hypertensive patients,131415 they may not be representative of the BP in non-hypertensive and hypertensive individuals in general practice. Our study included both non-hypertensive and hypertensive individuals based on ausAOBP and showed a very high correlation between the three office BP measurements. However, ausAOBP showed the highest BP values, resulting in a difference in the prevalence of hypertension of up to 17.8% (Fig. 2). A notable finding of our study was subgroup analysis by hypertension status. The difference in BP between the three office BP measurements was relatively small, about 3 mmHg systolic/diastolic in non-hypertensive individuals but larger in the hypertensive group (Table 2). These findings were similar to those of a recent meta-analysis.10
Many studies have compared the discrepancies between office BP and out-of-office BP measurements.78911121314151617 However, only a few studies have included four or five methods of measuring BP, as we did.16181920 The results differed between studies with differences in the study population. The present study showed a significant difference between office BP and out-of-office BP in all subjects, but especially in hypertensive patients taking or not taking antihypertensive medication. This finding reinforces the importance of out-of-office BP measurements for appropriate BP control in hypertensive patients.
Our study showed that the prevalence of white-coat hypertension based on ausAOBP was about a quarter (25.4–26.8%) higher than that based on aAOBP (17.5–21.1%). Another study in Korea reported that the prevalence of white-coat hypertension was 20.1%.12 Meanwhile, the prevalence of masked hypertension based on both ausAOBP and aAOBP in our study was about one-third, which is slightly higher than that of another study in Korea (23.4%).12 These differences may have been due to different definitions of hypertension phenotypes between studies. There was no significant difference in the present study according to sex due to the small number of subjects. However, the prevalence of white-coat hypertension was numerically higher in women than that in men (33.3% vs. 21.1%, P = 0.244), whereas that of masked hypertension was higher in men than in women (42.1% vs. 17.6%, P = 0.112), consistent with previous studies.1121 Considering the above, together with our findings that there was only fair-to-moderate agreement (kappa = 0.393–0.508; Fig. 3, Supplementary Fig. 2) with the true categories of normotension and hypertension between office BP and out-of-office BP, out-of-office BP measurements should be used together with office BP measurements in clinical practice to reduce the misclassification of hypertension.2223
This study has some limitations that need to be considered. First, the study was conducted in a single center with a relatively small number of population, which may limit the generalizability of the findings to other populations. Second, this study did not evaluate the long-term clinical outcomes of the different BP measurement methods, which may be an area for future research. Third, our study did not randomize the sequence of office BP measurements, which may have led to higher ausAOBP. Fourth, this study measured office BPs with the OMRON HEM-907. A recent validation study in a small Korean population reported that DBP values measured with the OMRON HEM-907 may be underestimated compared with an electronic auscultatory device and did not meet the accuracy requirements of the universal standard for DBP.24 However, in our study, the office BPs were measured with the same device (OMRON HEM-907), rather than comparing different devices for office BP measurement. Therefore, further validation studies are required to determine whether it can serve as a reference standard for BP measurement with various devices. Despite the limitations mentioned above, the strengths of this study include its prospective design, the use of standardized BP measurement techniques, the inclusion of different BP measurement methods, and the results of BP differences according BP status.
In conclusion, this study showed that although BP values from different BP measurement methods are significantly correlated, auscultatory office BP measurement may overestimate BP values from other methods, particularly at elevated BP levels. This implies that a holistic approach employing diverse modalities for measuring BP can provide additional insights for clinical BP assessment, especially for patients with suspected white-coat hypertension or those with difficult-to-treat hypertension. Further multicenter studies are needed in the Korean population so as to accurately determine the differences in out-of-office BP according to the degree of office BP with different BP measurement methods.
 XML Download
XML Download