

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Proton pump inhibitors (PPIs) and histamine-2 receptor antagonists (H2RA) are widely used acid suppressants for treatment of acid-related gastrointestinal (GI) diseases such as peptic ulcer disease, heart burn, Zollinger-Ellison syndrome, and gastroesophageal reflux disease.12 They are also frequently used as prophylactic measures to prevent ulcers associated with certain medications such as nonsteroidal anti-inflammatory drugs, aspirin, and steroids.34 PPI acts by irreversibly binding to H+/K+ ATPase of gastric parietal cells to inhibit acid secretion, thereby lowering gastric pH,5 the H2RA competitively binds to histamine type 2 receptors on the basolateral surface of parietal cells thereby suppressing secretion of acid.1 Although PPI has strong potency for acid inhibition, wide use has raised concerns for adverse effects including development of pneumonia, gastric and colorectal cancer, hip fracture, and Clostridium difficile infection.6 Although adverse effects of H2RA are usually minor, meta-analysis reported increased risk of C. difficile infection and inflammatory bowel disease associated with H2RA use.78 Long-term reduction of gastric pH can alter composition of gut microbiota leading to development of different GI disease, and some studies have reported that exposure to PPI can increase the risk of allergic diseases such as atopic dermatitis and asthma.9 Recent studies have shown that prominent dysbiotic disruption can occur after only 4 to 8 weeks of PPI use, and it can lead to permanent disruption.1011
Rosacea is a common inflammatory skin disease characterized by various symptoms including erythema, telangiectasia, papules and pustules. Multiple etiologies, including genetic predisposition, environmental factors, skin barrier dysfunction, immune system dysregulation, and neurovascular dysregulation are known to contribute the pathophysiology of the rosacea, but exact pathogenesis of rosacea is unclear.121314
Recently, a study by Dai et al.15 reported that PPI use was significantly associated with increased risk of rosacea. PPI is a potent acid suppressant, and such association is most likely explained by inhibition of gastric acid. We aimed to retrospectively evaluate the association between acid suppressants and rosacea in the Korean population. The study also aimed to identify other factors associated with development of rosacea in the Korean population.
METHODS
Data source and study subjects
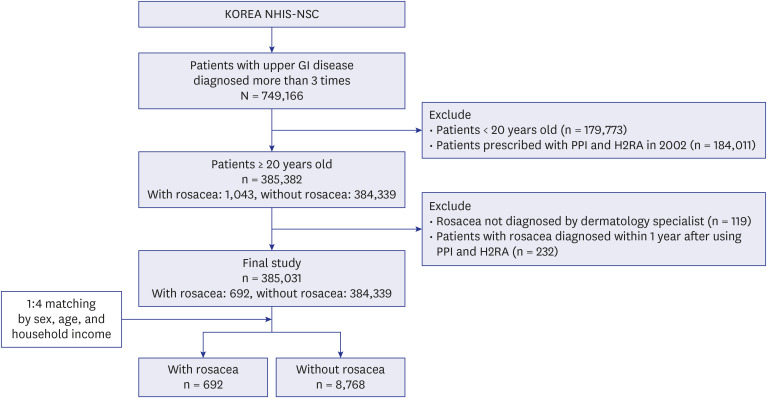
This study used data from the Korean National Health Insurance Service-National Sample Cohort, which is a nationwide cohort database gathered from 2% (1 million) of the total eligible Korean population (50 million) who were followed up for 12 years until 2013. The cohort provides information on patient’s medical history including diagnosis codes, prescribed medications, and information on socio-demographic factors including household income. The case cohort was defined as patients diagnosed with rosacea (Korean Standard Classification of Disease [KCD] codes L71.0, L71.8, L71.9) by dermatology specialists for the first time who had prior exposure to PPI and H2RA for more than 90 days at least 1 year before diagnosis of rosacea. The control cohort was defined as patients with esophageal, gastric, and duodenal diseases (KCD codes K20–K31) diagnosed at least 3 times who were prescribed with H2RA or PPI for more than 90 days. The cohort consisted of 692 subjects in case cohort and 749,166 subjects in control cohort. Subjects less than 20 years old, H2RA or PPI exposure for less than 90 days, H2RA or PPI prescribed before 2003, and any rosacea diagnosed by non-dermatologists or diagnosed within 1 year after first exposure to H2RA or PPI were excluded. For each case cohort subject, 4 control cohort subjects were matched using age, sex, index date and household income (the National Health Service groups household income into 10 separate groups for which groups 0, 1, 2, and 3 are categorized as low household income, 4, 5, 6, and 7 as intermediate, and groups 8, 9, and 10 as high household income). Final analysis included 692 subjects in case cohort and 2,768 subjects in control cohort (Fig. 1).
Acid suppressants and dose
Defined daily dose (DDD) was used for standardization of each medication, which is the assumed average maintenance dose per day for its main indication set by World Health Organization Collaborating Centre for Drug Statistics Methodology. The H2RA included in analysis are cimetidine (800 mg), ranitidine (300 mg), famotidine (40 mg), nizatidine (300 mg), and lafutidine (20 mg). The PPI included in analysis are pantoprazole (40 mg), esomeprazole (30 mg), lansoprazole (30 mg), dexlansoprazole (30 mg), and rabeprazole (30 mg). Cumulative dose equivalent to DDD (cDDD) was counted as 1, and total cDDD was grouped into less than 30, 30–120, and more than 120, where DDD less than 30 was defined as the reference group.
Covariates
Covariates included in the analysis were age (20–29, 30–39, 40–49, 50–59, and ≥ 60), sex (female, and male), residence (rural, and metropolitan), income (low, medium, and high), and comorbidities, which were assessed by Charlson Comorbidity Index (CCI) wherein each comorbid conditions were combined to calculate a single score.
Statistical analysis
Cross-tabulation analysis was used for between-group analysis. Odds ratio (OR) with 95% confidence interval (CI) for association between acid suppressants and development of rosacea after adjusting for covariates (age, sex, income, residence, and CCI score) was calculated using logistic regression analysis. A P value of 0.05 was considered statistically significant. All statistical analyses were performed using IBM SPSS software (version 26.0; IBM Corp., Armonk, NY, USA) and a P value less than 0.05 was considered statistically significant.
RESULTS
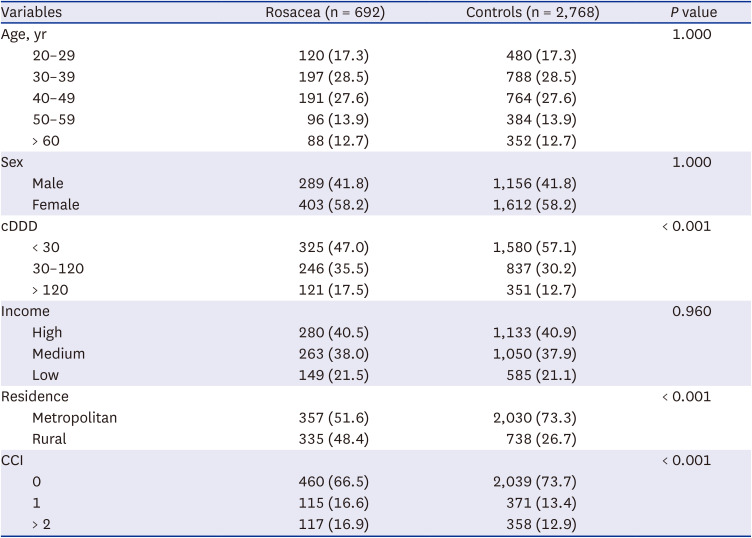
A total of 3,460 subjects with acid suppressants prescribed for more than 90 days were included in final analysis; among them, 692 were diagnosed with rosacea after 1 year since first exposure to acid suppressants. Age, sex and income were well matched and did not show significant difference between patients with rosacea and control group. The cDDD showed different distribution between the two groups. Patients with rosacea were exposed to longer duration of acid suppressants than control group (35.5% vs. 30.2%, respectively in cDDD 30–120, P < 0.001; 17.5% vs. 12.7%, respectively in cDDD > 120, P < 0.001). A significantly greater number of patients with rosacea were residing in the rural area than the control group (48.4% vs. 26.7%, respectively, P < 0.001) and patients with rosacea had greater CCI score than the control group (16.9% vs. 12.9%, respectively in CCI ≥ 2, P < 0.001). The comparison of demographic data is presented in Table 1.
Table 1
Demographic data of patients with rosacea and controls
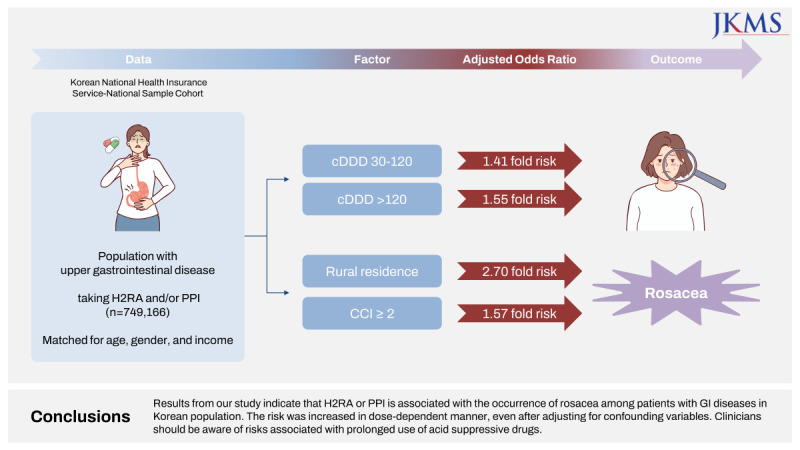
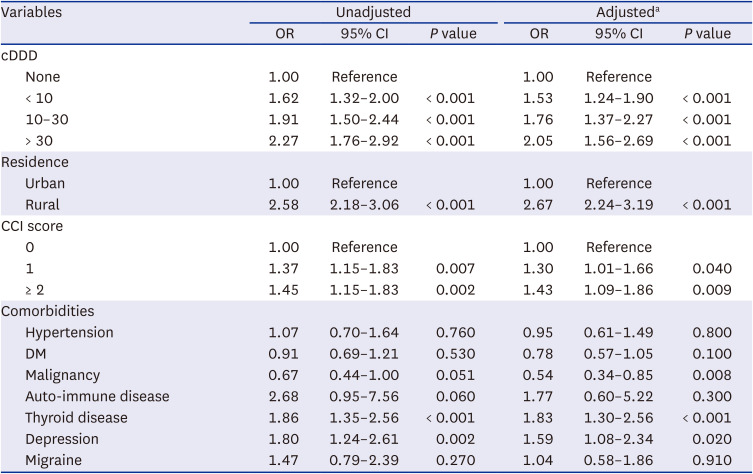
Longer use of acid suppressants was significantly associated with increased risk of rosacea. Acid suppressants use of cDDD more than 30 days increased risk of rosacea (OR, 1.43; 95% CI, 1.19–1.72; P < 0.001) and cDDD more than 120 days was associated with even greater risk of rosacea (OR, 1.68; 95% CI, 1.32–2.13; P < 0.001). After adjustment for possible confounders, increased cDDD was still significantly associated with risk of rosacea (OR, 1.55; 95% CI, 1.20–2.00; P = 0.001). Other factors significantly associated with risk of rosacea include residing in the rural area (OR, 2.58; 95% CI, 2.18–3.06; P < 0.001), greater CCI score (OR, 1.45; 95% CI, 1.15–1.83; P = 0.002), and comorbidities (malignancy, thyroid disease, and depression). Results for OR are presented in Table 2. When duration of acid suppressants was limited to use less than one year, increased cDDD was still associated with risk of rosacea (OR, 2.05; 95% CI, 1.56–2.69; P < 0.001) and similar trend was also observed for area of residence, CCI score, and comorbidities (Table 3).
Table 2
Logistic regression results for risk of rosacea
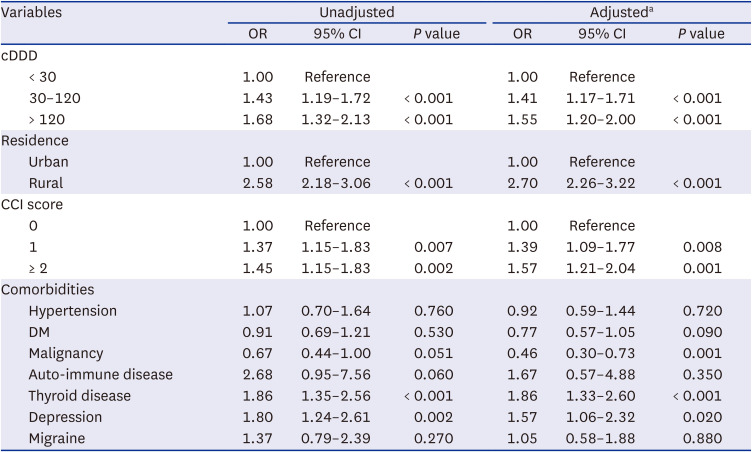
Table 3
Logistic regression results for risk of rosacea, when acid suppressants use was limited for 1 year
DISCUSSION
To our knowledge, this is the first study to analyze the association between acid suppressants including H2RA and PPI, and risk of rosacea using a nationwide cohort. H2RA and PPI are widely used for their excellent acid suppressing effects, but prolonged use has raised concerns related to outcome from elevated gastric pH. In this study, we observed that patients with rosacea were exposed to longer duration of acid suppressants compared to the cohort group, and significant association between prolonged use of acid suppressants and increased risk of rosacea was found in dose-response trend, even after adjusting for confounding variables. When analysis was limited to use less than 1 year, a similar trend was observed with even greater OR value with smaller cDDD. The results of our study provide epidemiological evidence for an association between acid suppressants and rosacea in the Korean population.
Alteration of gut pH has been associated with altered composition of gut microbiota.1617 A large study using fecal samples from 1,827 healthy twins reported that PPI use was associated with altered composition and reduced diversity of microbiota.16 The study hypothesized that an increase in gastric pH caused by PPIs could alter the composition of the gut microbiota, which could potentially lead to an increased susceptibility to infections and other complications.16 Disruption of gut microbiota has been associated with different GI diseases such as small intestinal bacterial overgrowth, and C. difficile infection, but recent studies also reported association with inflammatory skin diseases, emphasizing the importance of “gut-skin axis.”1819202122 The skin and gut share similar important characteristics such as high vascularization and dense innervation but they are also colonized with distinct microbial communities.21 Although the mechanism is not clear, studies have shown strong association between skin and gut modulated by immune environment via the microbiota that directs to existence of “gut-skin axis,” clinically relevant inter-organ communication.2324
Since the introduction of metagenomics, there is an increased interest in studying the link between microbial organisms and human body and it has led to revealing pathogenesis of several dermatologic diseases.252627 Evidence suggests that dermatologic diseases are not only influenced by skin microbiota alone, but also by gut microbiota as shown by Song et al.,28 who reported that altered microbiota was related to exacerbation of atopic dermatitis by aberrant Th2-type immune response. Also, improvement of skin inflammation after administration of oral prebiotics and probiotics suggest perplexing connection between the gut, brain, and skin.29 Although the association of gut microbiota in pathogenesis of rosacea is yet to be elucidated, metagenomic studies by Nam et al.,30 and Chen et al.,31 compared gut microbiota between healthy subjects and rosacea patients. The results on change of specific bacteria were different possibly owing to difference in demographics, but both studies observed differences in microbiota between healthy subjects and patients with rosacea. Although the studies are limited by the small number of rosacea patients included in the study, this suggests a possible role of gut microbiota in rosacea through the gut-skin axis.
PPI and H2RA have different mechanisms for suppressing gastric acidity, and increase in gastric pH has been associated with change in microbiota. Although PPI is more potent than H2RA, alteration of gastric pH itself is a risk factor for altered microbiota, as acidic barrier renders the stomach unfavorable for bacterial survival as observed in different studies.3233Accordingly, we analyzed the effect of both H2RA and PPI and its association with rosacea to observe the overall effect of acid suppressing agents.
Our study matched population for age, sex, and income and found distinct association between acid suppressants and rosacea. Unlike medications for hypertension or diabetes mellitus that are used daily for several years, acid suppressants are usually prescribed for a limited amount of time which may be repeated depending on patient’s symptoms. Results from our retrospective study that collected data from a national cohort over 10 years showed association with acid suppressants and risk of rosacea in dose-dependent manner, but even short duration of less than 1 year was associated with risk of rosacea suggesting that acid suppressants can cause gut dysbiosis in short time, and such effect is maintained for prolonged period of time.
Also, rural residency was identified as another risk factor for rosacea development. Sun exposure has long been acknowledged as a contributing factor in the development or exacerbation of rosacea,11 as symptoms of the condition are commonly observed in areas of the face that are frequently exposed to sunlight. The higher frequency of sun exposure experienced by rural residents, compared to those living in urban areas, is thought to be the underlying reason for the higher incidence of rosacea found in this population in the study. Several comorbidities have been identified as having an association with rosacea, including cardiovascular diseases, depression, GI disorders, cancers, neurological diseases, and autoimmune conditions.12 We have also observed that the risk of rosacea increases with the increase in CCI.
The limitations of this study are that the analysis of insurance prescription records may not reflect the actual clinical environment, also, there may be cases which rosacea diagnosis is missed due to the majority of rosacea diagnoses being performed by dermatologists. Also, separate analysis for H2RA and PPI could provide results for different types of acid suppressants, but the number of patients diagnosed with rosacea who had been taking acid suppressants in Korea are very limited, which is another limitation. In conclusion, results from our study indicate that H2RA or PPI is associated with the occurrence of rosacea among patients with GI diseases in the Korean population.
 XML Download
XML Download