

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Allergic rhinitis (AR) is a common disease affecting over 500 million people globally, using a conservative estimate. Its prevalence has increased with industrialization and a Westernized lifestyle.1 AR is a nasal inflammatory disorder induced by an immunoglobulin E (IgE)-mediated immune response to inhaled aeroallergens.2 The upper airway symptoms (nasal obstruction, rhinorrhea, sneezing, and itching) of AR impact an individual’s performance at school, productivity at work, social life, and quality of sleep.3 Considering the socioeconomic burden of AR, it is important to study the pathophysiological characteristics of patients with AR. The patency of the nasal cavity and inflammatory neurotransmitter secretions are affected by the autonomic nervous system (ANS) activities, causing nasal symptoms in patients. Hence, ANS activity plays a critical role in the clinical manifestations of AR.4
Heart rate variability (HRV) is a noninvasive method that can be measured via single-lead electrocardiography (ECG) to evaluate cardiac autonomic activities.5 HRV parameters were generated by measuring the quantitative variation in normal-to-normal (NN) heartbeats.6 HRV is often used for assessing ANS function and estimating an individual’s health status. Several studies have reported that chronic diseases are related to ANS imbalance, based on HRV7; however, few studies have focused on the association with AR, a representative chronic disease. Further, the measured time of HRV in these studies was 5–30 minutes, making it difficult to understand ANS modulation throughout the day in patients with AR.48910 ANS monitoring requires 24 hours because the disease affects patients’ sleep and their daytime life.
We aimed to evaluate the 24-hour ANS activities in patients with AR. It was hypothesized that symptoms associated with AR are related to changes in the ANS, and can be measured through HRV analysis. We assessed the time- and frequency-domain parameters of HRV using 24-hour Holter monitoring in patients with AR and compared the results with those of healthy individuals.
METHODS
Participants
We enrolled 34 adult patients who visited our clinic and were newly diagnosed with AR between February 2021 and October 2021. We enrolled subjects with AR according to the following inclusion criteria: 1) adult patients (age ≥ 18 years); 2) patients who complained of nasal symptoms (anterior or posterior rhinorrhea, sneezing, nasal blockage, and nasal itching); and 3) class 1 responses or more in the multiple-allergen simultaneous test (MAST) using Advansure Alloscreen™ (LG Life Sciences, Seoul, Korea). We excluded patients with the following criteria: 1) patients with nasal polyposis and/or sinusitis on endoscopic examination; 2) patients who took oral or topical nasal medications 2 weeks before the HRV study; and 3) a history of specific pathology related to HRV changes (coronary heart disease, arrhythmia, stroke, asthma, or psychiatric disorder). Before prescribing medications for AR, the participants underwent Holter monitoring for 24 hours. During the 24-hour Holter monitoring, participants were instructed to avoid excessive exercise, caffeinated beverages, and alcohol consumption on the study day. All data from the 24-hour Holter monitoring were interpreted by C.K.J., a cardiologist. Of the 34 patients, two were excluded for newly diagnosed arrhythmia and low-quality data (artifacts > 10% on Holter monitoring), and 32 participants were finally evaluated. We assessed the nasal symptom score and blood samples for total IgE and eosinophil counts to evaluate the degree of AR in the patients. The score for each nasal symptom (nasal obstruction, rhinorrhea, sneezing, and itching) was measured by having the participants rate the severity on a four-point Likert scale (0 = absent, 1 = mild, 2 = moderate, 3 = severe). The total nasal symptom score was calculated as the sum of the symptom score.
The control group was selected from the Department of Cardiology Holter registry from May 2018 to April 2019. During this period, 1,620 participants underwent 24-hour Holter monitoring. We excluded patients with a history of AR, asthma, atopic dermatitis, coronary artery disease, cerebrovascular disease, heart failure, chronic kidney disease, atrial fibrillation, and syncope according to their medical records. We also excluded patients with arrhythmia detected in the Holter data or those with low-quality data. The control group was matched with 32 patients with AR according to age (± 5 years), sex, hypertension, and diabetes and was selected four-fold. Finally, 128 controls with no MAST results were selected to compare HRV parameters in patients with AR.
HRV
HRV data were acquired via ECG data from Holter monitoring (MARS; GE Healthcare, Chicago, IL, USA) and analyzed using time- and frequency-domain methods. Fast Fourier Transform (a non-parametric spectral estimation method) was used to convert single-lead ECG signals to power spectral densities. The cubic spline-interpolated NN interval function was sampled at 1,024 samples/300 seconds or 3.413 samples/sec. We omitted NN intervals < 150 ms or > 5,000 ms and NN interval ratios < 0.80 or > 1.20 prior to HRV analysis. The following parameters were adapted using time-domain methods: 1) average NN interval, 2) standard deviation of NN interval (SDNN), 3) standard deviation of the 5-minute averages of NN interval (SDANN), 4) square root of the mean of the squared differences of adjacent NN interval (RMSDD), and 5) the rate of number of pairs of adjacent NN intervals more than 50ms (NN50) in the total number of NN interval (pNN50). The frequency-domain parameters were evaluated as the average of the values measured every 5 minutes as follows: 1) very low-frequency (VLF) component, power of 0.0033–0.0400 Hz; 2) low-frequency (LF) component, power of 0.0400–0.1500 Hz; 3) high-frequency (HF) component, power of 0.1500–0.4000 Hz; 4) LF to HF ratio (LF/HF); 5) LF power of normalized unit (LFnu), LF/(LF + HF) × 100; 6) HF power of normalized unit (HFnu), HF/(LF + HF) × 100. We considered patients to have sympathetic withdrawal when the LF/HF was below the mean value of the participants (LF/HF > 1.67).
Statistical analysis
All analyses were performed using SPSS version 20.0 software (SPSS Inc., Chicago, IL, USA), and a P value < 0.05 was considered significant. Values obtained during this study were expressed as percentages (for categorical variables) or means ± standard deviations (for normally distributed continuous variables). We used the χ2 test and independent t-test for comparative analysis between the AR and control groups. Univariate analysis was performed to evaluate the odds ratios (ORs) and 95% confidence intervals (CIs) of the independent factors associated with parasympathetic predominance. Multiple logistic regression analysis was used, including variables measured in univariate analysis, to evaluate adjusted ORs and their 95% CI.
RESULTS
Characteristics of the study participants
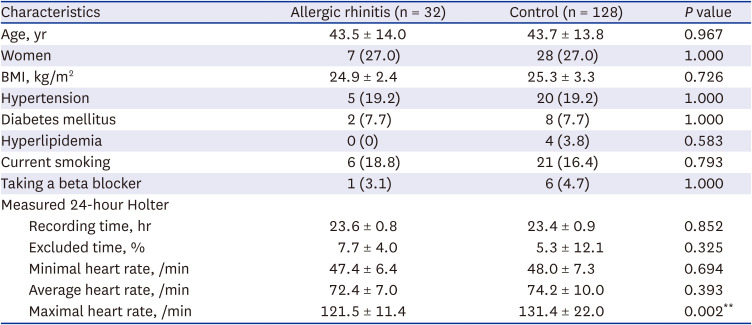
There was no difference between the AR and control groups in terms of demographics because we selected controls matched with AR patients. In addition, no difference was discovered in measuring time, excluded time, and minimal and average heart rates of raw Holter data between the groups. However, the maximal heart rate was significantly lower in the AR group than in the control group (Table 1).
Table 1
Baseline characteristics of the participants
Characteristics of the AR group
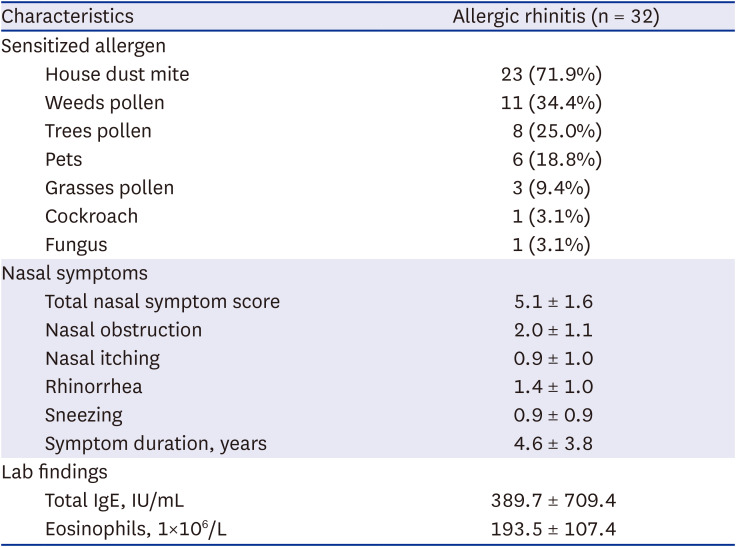
The most sensitized allergens were house dust mites (Dermatophagoides pteronyssinus and Dermatophagoides farinae), followed by weed pollen, tree pollen, and pets. The AR group presented a mean symptom score of 5.1 and a mean symptom duration of 4.6 years. The most struggling nasal symptom was nasal obstruction (mean score of 2.0), followed by rhinorrhea (mean score of 1.4) (Table 2).
Table 2
Clinical characteristics of the allergic rhinitis group
HRV analysis of participants
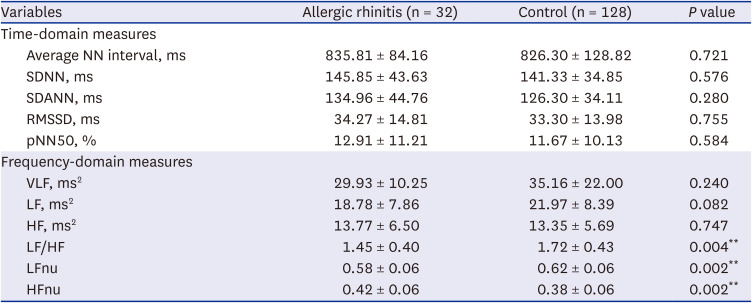
All parameters measured using the time-domain methods revealed no difference between the AR and control groups. However, in the frequency-domain methods, LF/HF, LFnu, and HFnu differed between the two groups. The measured LF/HF (1.45 ± 0.40 vs. 1.72 ± 0.43, P = 0.004) and LFnu (0.58 ± 0.06 vs. 0.62 ± 0.06, P = 0.002) were significantly higher in the control group than in the AR group. Inversely, the HFnu of the AR group was significantly higher than that of the control group (0.42 ± 0.06 vs. 0.38 ± 0.06, P = 0.002) (Table 3).
Table 3
The differences in heart rate variability between the allergic rhinitis and control groups
Values are expressed as means ± standard deviations (for normally distributed continuous variables).
NN = normal-to-normal, SDNN = standard deviation of NN interval, SDANN = standard deviation of the 5-minute averages of NN interval, RMSDD = square root of the mean of the squared differences of adjacent NN interval, pNN50 = rate of number of pairs of adjacent NN intervals more than 50 ms in the total number of NN interval, VLF = very low-frequency, LF = low frequency, HF = high frequency, LFnu = LF power of normalized unit, HFnu = HF power of normalized unit.
**P < 0.01.
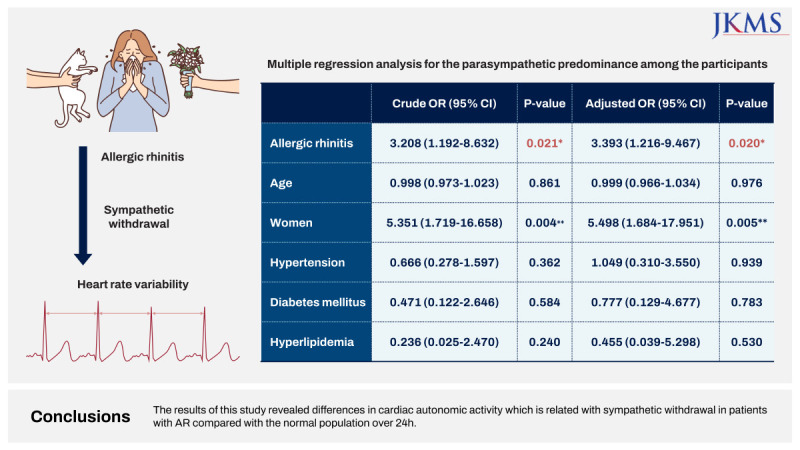
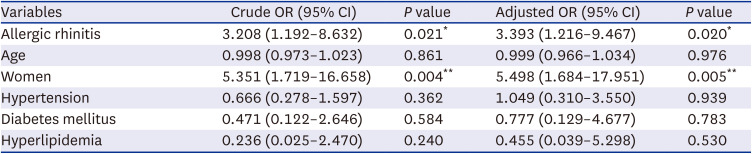
Logistic analysis revealed that AR (OR = 3.208, P = 0.021) and women (OR = 5.351, P = 0.004) were significantly associated with sympathetic withdrawal (LF/HF < 1.67). After adjusting for all other variables in the table, AR and women were independently associated with sympathetic withdrawal (adjusted OR = 3.393, P = 0.020 for AR; adjusted OR = 5.498, P = 0.005 for females) (Table 4).
Table 4
Multiple regression analysis for the parasympathetic predominance among the participants
DISCUSSION
HRV, which evaluates the time variations between heartbeats, is a noninvasive assessment of cardiac autonomic activity via single-lead ECG. Previous studies have revealed that LF power reflects sympathetic and parasympathetic modulation, whereas HF power reflects parasympathetic modulation.6711 Therefore, LF/HF represents sympathetic modulation in which the influence of parasympathetic activity is partially eliminated.12 HFnu and LFnu are regarded as modulation parameters of the parasympathetic and sympathetic branches of the ANS, respectively, and are inversely related to each other.13 We discovered that LF/HF and LFnu were significantly lower, and HFnu was significantly higher in the AR group than in the control group. In the multiple regression model, we also discovered that AR was an independent factor that measured LF/HF below the mean of the participants. Our findings suggest that: 1) patients with AR reveal parasympathetic predominance and sympathetic withdrawal for 24-hour compared to controls, and 2) AR is independently associated with sympathetic withdrawal.
Most chronic diseases are generally associated with impaired ANS balance, resulting in overstimulation of the sympathetic nerve and a lack of vagal activity,7 whereas AR reveals sympathetic withdrawal. Several mechanisms of AR may explain this unusual ANS imbalance. The ANS primarily influences the nasal mucosal vasculature. Allergen-induced parasympathetic stimulation promotes nasal obstruction and rhinorrhea, which are the cardinal symptoms of AR.14 In contrast, activation of the sympathetic nervous system causes blood vessel constriction in the nasal cavity, thus increasing nasal patency, which is rarely associated with AR. In addition, nitric oxide released by vagal hyperactivity may enhance Th2 lymphocyte proliferation, which leads to cytokine production, consequently aggravating AR.1516 Also, the central effector cells in allergic rhinitis, such as mast cell, basophils, and eosinophils, are express cholinergic receptors which are prone to cholinergic modulation.17
In literature, several studies presented the association between AR and ANS imbalance during short duration. The effects of AR on the ANS were consistently parasympathetic predominance and sympathetic withdrawal; however, the methods for assessing the ANS varied. Ozsutcu et al.18 reported that smaller pupil diameters in children with AR than in the control group were evidence of parasympathetic hyperactivity. In an American study, the ANS scores, measured by the quantitative sudomotor test, heart rate response, and blood pressure response, also represented sympathetic withdrawal in 10 patients with allergy compared to 16 age-matched controls.19 A case-control study revealed increased parasympathetic activity using sympathetic skin response and heart rate interval variation in 55 children with AR compared to 40 controls.20
The effects of AR on the ANS persist during sleep and throughout the day. Nasal congestion due to AR causes sleep disturbances and may be associated with obstructive sleep apnea.21 The sympathetic predominance in patients with obstructive sleep apnea has been reported in many studies.222324 Therefore, 24-hour monitoring is essential for evaluating the ANS status of patients with AR. To our knowledge, most ANS measurements using HRV have been assessed for a short duration when nasal resistance changes with postural modification or allergen provocation tests,48910 and only two Turkish studies have measured for 24 hours.2526 In a 24-hour HRV study conducted for children, the difference in time-domain parameters (RMSSD and pNN50) and frequency-domain parameters (HF and LF/HF) were measured between the AR and control groups.25 Another study reported that time-domain parameters (RMSSD and pNN50) of HRV measured by 24-hour Holter monitoring were greater in 24 adults in the AR group than in 22 participants in the control group.26 It differed from our results because our study revealed differences in the frequency domain, not the time domain, between the AR and control groups. In general, there are strong correlation between time and frequency domain, but frequency domain methods are preferred to assess ANS under controlled condition.27 This discrepancy may have been caused by differences in ethnicity (East Asian vs. West Asian) and/or age (adults vs. children) between both studies. However, we believe that the results of our study are more reliable because the representativeness of the general population by the controls increased through 1:4 matching.
In the multiple regression model, AR and women were independent risk factors for sympathetic withdrawal. This is an interesting finding because women demonstrated a lower LF/HF than men in a previous meta-analysis, and AR revealed an effect equivalent to that of the women.28 Previously, the dominance of the parasympathetic nervous system in women is affected by hormones such as estrogen and oxytocin, which has been proven through human and animal experiments.29 The reciprocity the neural control of the heart in men and women is also related to the women’s sympathetic withdrawal.30 A meta-analysis is needed to evaluate the effect of ANS based on AR.
An altered balance of ANS has been presented in several cardiovascular diseases, such as heart failure, myocardial infarction, arrhythmia, and stroke.31 Most cardiovascular diseases are associated with sympathetic over activity and reduced parasympathetic activity, and even more this ANS imbalances are related with poor disease prognosis.32 Considering the opposite ANS imbalance of AR, it would be interesting if a study on the cardiovascular prognosis of AR patients with parasympathetic dominance is conducted in the future.
This study had several limitations. First, the control group had no allergy test result, although atopic disease was excluded from the medical records. To overcome this limitation, we selected a control group four-fold to increase the representativeness of the general population; however, a follow-up study to select a control group through an allergy test is needed. Second, selection bias was possible because only those who agreed to delay drug administration until the 24-hour Holter monitoring were enrolled. Thus, participation may have been low in patients with more severe AR symptoms. Third, controls were selected from a Holter registry. We carefully excluded patients with diseases that could affect HRV by criteria. Nevertheless, there is a possibility that the control group was accompanied by undiscovered cardiac pathology.
In conclusion, among the HRV parameters measured by 24-hour Holter monitoring, LFnu, Hfnu, and LF/HF differed between the AR and control groups, implying parasympathetic predominance and sympathetic withdrawal during 24 hours in patients with AR. Moreover, AR is an independent risk factor for sympathetic withdrawal. Further studies are needed to elucidate whether the degree of ANS imbalance is correlated with AR severity or if it can be corrected by appropriate treatment.
 XML Download
XML Download