

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
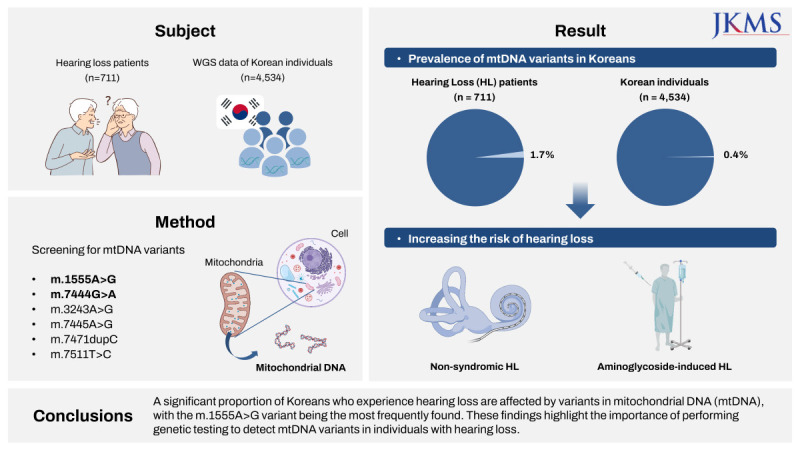
Hearing loss is the most prevalent sensory organ disorder, affecting approximately 1–2 per 1,000 newborns. More than half of congenital hearing loss cases are due to genetic causes,12 with 80% of genetic hearing loss inherited in an autosomal recessive manner and 20% inherited in an autosomal dominant manner or through less prevalent inheritance patterns, such as X-linked or mitochondrial inheritance.3 However, the proportion of post-lingual genetic hearing loss cases caused by mitochondrial DNA (mtDNA) variants increases with ethnic diversity. Causative mtDNA variants have been identified in 5% of Caucasians with post-lingual non-syndromic hearing loss4 and in 2.5–4.4% of Asians.567
Although the frequency of mtDNA variants varies by ethnicity, the m.1555A>G variant of MTRNR1 is the most common mitochondrial variant associated with deafness, especially aminoglycoside-induced or non-syndromic hearing loss.568910 Several other variants, including m.3243A>G in MTTL1,1112 m.7444G>A and m.7445A>G in MTCO1,13141516 m.7471dupC and m.7511T>C in MTTS1,17181920 have been causally linked to deafness in multiple studies.21 In addition to non-syndromic hearing loss, mitochondrial variants cause syndromic hearing loss. The m.3243A>G variant in the MTTL1 gene, which encodes leucine transfer RNA, has been linked to maternally inherited diabetes and deafness (MIDD) and mitochondrial encephalomyopathy, lactic acidosis, and stroke-like episodes (MELAS).1112 In addition to post-lingual and progressive deafness, the MTCO1 m.7445A>G variant is also associated with palmoplantar keratoderma.1314
Despite increasing reports of new mtDNA mutations associated with hearing impairment, the proportion of congenital or post-lingual hearing loss attributable to mtDNA mutations in cohorts with varying degrees of hearing loss remains unknown. Thus, this study aimed to investigate the frequency of mtDNA mutations in a cohort of individuals with pre- or post-lingual hearing loss of varying severity. Towards this goal, we screened m.1555A>G, m.3243A>G, m.7444G>A, m.7445A>G, m.7471dupC, and m.7511T>C variants of the mitochondrial genome, variants highly associated with sensorineural hearing loss. In addition, the frequencies of these variants, as well as the clinical and audiological characteristics of patients identified as carrying these mitochondrial variants, were investigated.
METHODS
Study design and patients
Patients with hearing loss were enrolled in the Yonsei University Hearing Loss (YUHL) cohort after providing informed consent for the study and publication of their clinical data. Molecular analysis was conducted on probands and additional family members from 711 Korean families, encompassing a total of 1,099 individuals. The inclusion criterion was hearing loss patients aged 0 to 75 years with multiple affected family members or suspected to harbor sporadic genetic mutations. Hearing loss caused by congenital cytomegalovirus infection or other medical conditions primarily affecting hearing function was excluded.
Clinical evaluation
All patients underwent a comprehensive physical examination and history interviews. Audiological evaluations using otoscopy, tympanometry, and pure-tone audiometry were conducted for all patients as well as for their affected and unaffected family members. Air and bone conduction thresholds were measured in a double-walled audio booth at frequencies of 250–8,000 Hz and 250–4,000 Hz, respectively. The level of hearing loss was categorized as mild (26–40 dB), moderate (41–70 dB), severe (71–90 dB), or profound (> 90 dB) based on the average threshold of the four frequencies (500, 1,000, 2,000, and 4,000 Hz). The audiogram pattern was defined as ascending when the average thresholds for high frequencies (2,000 Hz and 4,000 Hz) were 25 dB less than those for low frequencies (250 and 500 Hz), ski-sloping when high frequencies were more than 25 dB than low frequencies, and flat when the difference between high and low frequencies was within 25 dB.
Control data collection
We used the whole-genome sequencing (WGS) data of 4,534 Korean individuals from the National Project of Bio Big Data. As part of this project, the gVCFs of 6,886 individuals from 4,534 unrelated families were generated using the GRCh38 assembly. We created a genomics database (genomicsDB) for the complete mitochondrial region (chrM:1-16569) of 6,886 individuals, called variants, using HaplotypeCaller in the Genome Analysis Toolkit (version 4.1.9.0, Broad Institute, Boston, USA).
Molecular analyses
Genomic DNA was extracted from peripheral blood lymphocytes using red blood cell lysis, cell lysis, and protein precipitation solutions (iNtRon Biotechnology, Inc., Seongnam, Korea). After extraction, polymerase chain reaction (PCR) and restriction fragment length polymorphism (RFLP) were performed to detect mtDNA variants. For the six target mtDNA variants, PCR was performed in 1,099 DNA templates from 711 families using the primers listed in Supplementary Table 1. After identifying the target band size in 1% agarose gels under ultraviolet light, RFLP was performed using the enzymes listed in Supplementary Table 1. Finally, 2% agarose gel electrophoresis was performed to determine whether the tested samples were positive for the variants.22 Mutation analyses of GJB2, TRMU p.A10S, MTND1 m.3308T>C, and MTND6 m.14484T>C were performed using the primers listed in Supplementary Table 2. The PCR products were analyzed using Sanger sequencing. The sequences were assembled and compared to those of GJB2 (NC_000013.11), TRMU (NC_000022.11), MTND1 (NC_012920.1), and MTND6 (NC_012920.1).
Haplogroup analysis of the mtDNA genome
To amplify the hypervariable region (HVR) of the mtDNA genome, PCR amplification of the template DNA was performed using the F15971 and R638 primers.23 After visualization in 1% agarose gel, the PCR product was analyzed using Sanger sequencing with primers F16328, F015, F314, R16509, R240, and R569, in addition to the amplification primers (Supplementary Table 3). Pairwise comparison and convergence of sequences were performed using the CLC Workbench version 20.0.1 (Qiagen, Hilden, Germany) to create a FASTA format file of the individual’s HVR sequence. Haplogroup analysis was performed using the ‘Classify’ function of HaploGrep2.24
Ethics statement
This study was approved by the Institutional Review Board (IRB) of Severance Hospital, Yonsei University Health System (IRB #4-2015-0659) and was conducted according to the tenets of the Declaration of Helsinki. We obtained written informed consent from individuals with hearing loss for their participation in this study and the publication of their clinical data.
RESULTS
Mutational screening of mtDNA variants associated with hearing loss
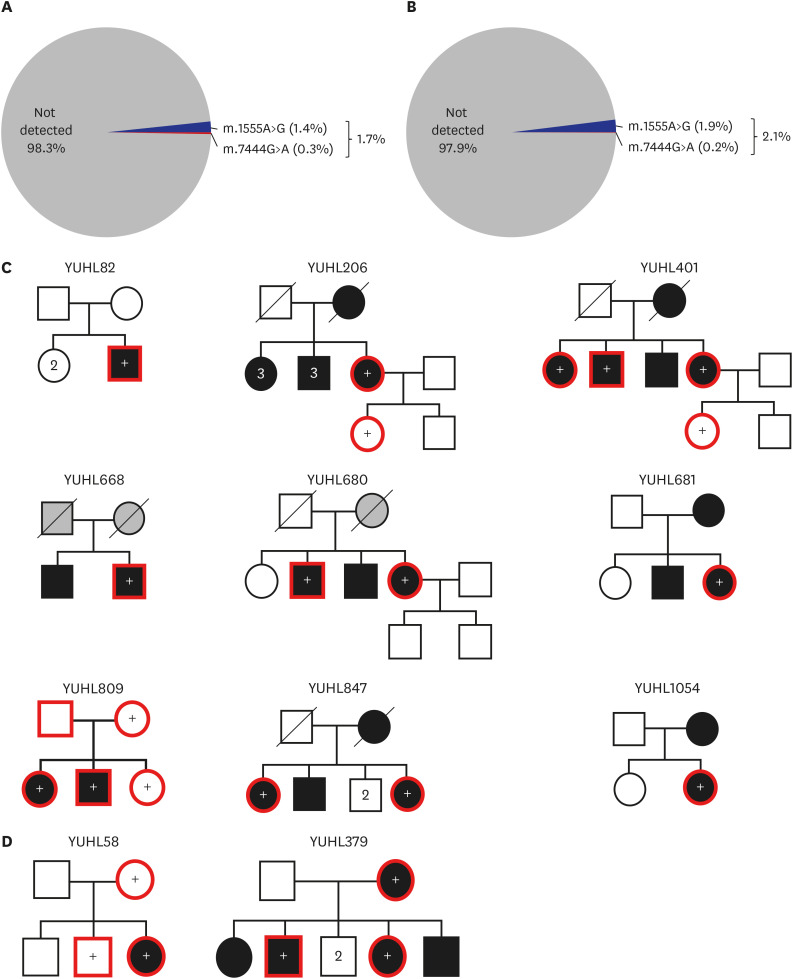
Of the 12 families that were identified with mtDNA variants, 10 out of 711 (1.4%) carried the m.1555A>G mtDNA variant whereas 2/711 (0.28%) were with the m.7444G>A variant (Table 1). None of the 759 individuals from the 373 unrelated families had the m.3243A>G, m.7445A>G, m.7471dupC, or m.7511T>C variants, indicating that these variants are extremely rare causes of hearing loss associated with mtDNA in Korea (Table 1). Overall, 1.7% of the YUHL cohort carried mitochondrial variants causing deafness (Fig. 1A). The detection rate in the phenotypic subgroup of individuals with post-lingual hearing loss with moderate-to-profound severity was 2.1%, suggesting that carriers of mtDNA variants, particularly those carrying the m.1555A>G variant, share clinical characteristics (Fig. 1B).
Table 1
Results of screening of deafness-causing mutations in mtDNA in Korean patients
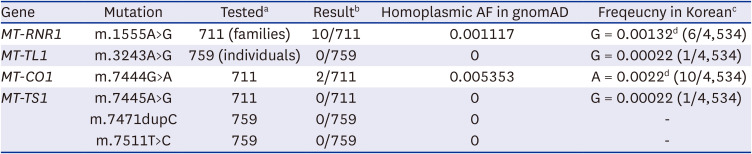
mtDNA = mitochondrial DNA, AF = allele frequency, gnomAD = Genome Aggregation Database.
aThe number of unrelated families or individuals whose mtDNA is analyzed for variants.
bThe number of individuals detected with mitochondrial variants.
cFrequency of mtDNA variants among the 4,534 Koreans from the National Project of Bio Big Data.
dAllele frequency of individuals carrying mtDNA mutations in both homoplasmic and heteroplasmic states.
Fig. 1
Detection rate of pathogenic mtDNA variants in the YUHL cohort and pedigree information summarizing segregation analysis. (A) Detection rate of mtDNA mutations that cause deafness in the YUHL cohort. Among the 711 families screened for mtDNA mutations, 10 unrelated hearing loss patients with the m.1555A>G variant and 2 patients with the m.7444G>A variant are identified. (B) Detection rate of deafness-causing mtDNA mutations in a group of YUHL patients with moderate-to-profound post-lingual hearing loss. (C) Pedigree and segregation results of families carrying m.1555A>G variant. (D) Pedigree and segregation results of families with m.7444G>A variant. Individuals highlighted in red were those available for RFLP and Sanger sequencing. ‘+’ indicated individuals with the mtDNA variants.
mtDNA = mitochondrial DNA, YUHL = Yonsei University Hearing Loss.
Twelve YUHL families with mtDNA variants did not have a pathogenic variant in GJB2, one of the most common genes responsible for non-syndromic hearing loss.252627 In addition, since whole exome or genome sequencing data were available for seven individuals with mtDNA variants, we analyzed genes associated with hearing loss and found no likely pathogenic or pathogenic variants that could explain their hearing loss in five patients (YUHL58-21, 82-21, 206-21, 379-21, and 401-21). The c.671G>T variants in EYA1 and c.491C>G in POU4F3 were found in YUHL379-21 and 849-21, respectively (Supplementary Table 4). Despite of the fact that both variants are reported as pathogenic in the Deafness Variation Database (http://deafnessvariationdatabase.org/), their allele frequencies (AFs) in East Asians and functional evidence indicate that they are insufficient to explain their hearing loss.
Given that hearing loss caused by the m.1555A>G or m.7444G>A variant is predominantly post-lingual and progressive, we hypothesized that these mitochondrial variants may be overlooked in people with adult-onset hearing loss. In the Genome Aggregation Database (gnomAD), the AFs of the homoplasmic m.1555A>G and m.7444G>A variants were 0.001 and 0.005, respectively (Table 1). Although gnomAD provides reliable AF for various populations, Koreans are underrepresented in the database. Therefore, we investigated mitochondrial variants in the Korean population using 4,534 WGS data from the National Project of Bio Big Data. In the WGS data, we detected four mitochondrial variants corresponding to four of the six mtDNA variants screened for YUHL: m.1555A>G, m.3243A>G, m.7444G>A, and m.7445A>G (Table 1). Regarding the four variants identified in the Korean control data, the m.1555A>G and m.7444G>A variants were identified in multiple individuals, with the m.1555A>G variant present in six individuals and m.7444G>A in ten individuals, whereas the m.3243A>G and m.7445A>G variants were only identified in one individual each in the heteroplasmic state. Four of the six m.1555A>G variant carriers and all m.7444A>G variant carriers identified in the Korean control data were in a homoplasmic state. Overall, a considerable proportion (18/4,534; 0.4%) of the Korean population is at risk of developing hearing loss, primarily due to the m.1555A>G variant.
Clinical and molecular characteristics of the 12 mitochondrial variant-bearing families
To evaluate the clinical characteristics of patients carrying mtDNA variants, the patients were classified according to age at diagnosis, sex, age at disease onset, degree of hearing loss, audiogram pattern, and mode of inheritance (Table 2). Hearing loss was predominantly familial with post-lingual onset and showed progressive features (Table 2). The mitochondrial variant m.1555A>G is frequently associated with variable onset and severity of hearing loss.728 Patients with the m.1555A>G variant in Korea exhibited a phenotype similar to that described in previous studies, in that the severity of hearing loss ranged from mild to profound. Consistent with previous reports,7282930 eight m.1555A>G carriers exhibited bilateral and symmetrical hearing loss. However, hearing loss in the other two carriers (YUHL847-21 and 1054-21) was asymmetric, and the unaffected sides had normal thresholds (Table 3). In addition, the average age at the onset of hearing loss for all m.1555A>G carriers was 48.5 years, but there was a wide range, with some carriers experiencing hearing loss from infancy and others not until their early 50s.
Table 2
Clinical characteristics of deafness-causing mtDNA variant carriers from the YUHL cohort
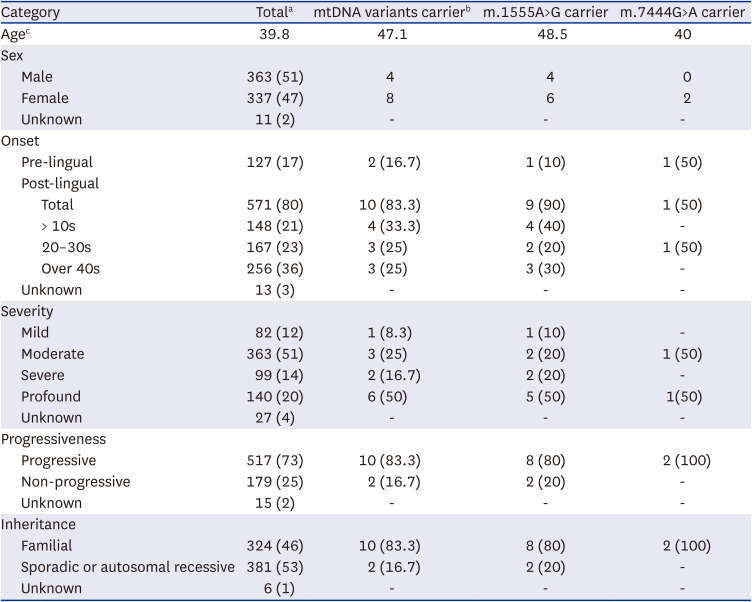
Table 3
Clinical and molecular characteristics of mtDNA m.1555A>G or m.7444G>A variant carriers in the Yonsei University Hearing Loss cohort
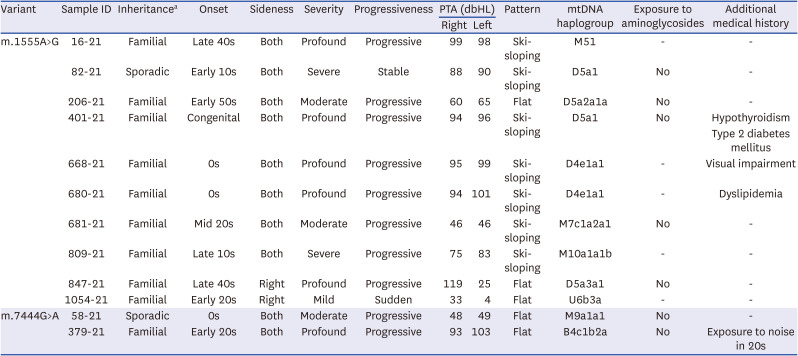
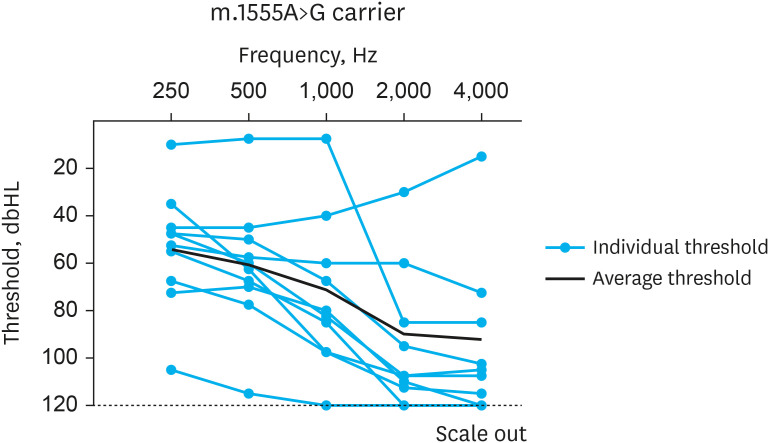
Among the 10 cases with the m.1555A>G variant, only 1 case (YUHL82-21) had sporadic inheritance, and the remaining 9 cases had familial inheritance (Table 3). Five of the nine familial cases (YUHL206-21, 401-21, 681-21, 847-21, and 1054-21) were suspected to be maternally transmitted despite incomplete penetrance (Fig. 1C). One of the m.1555A>G carriers (YUHL401-21) was also diagnosed with hypothyroidism and type 2 diabetes, and another m.1555A>G carrier (YUHL668-21) had severe visual impairment (Table 3). However, the exact association between these diseases and the m.1555A>G variant is unknown because of the lack of published reports. The individual and mean audiograms of the 10 individuals carrying the m.1555A>G variant are presented based on pure tone audiometry results in Fig. 2. These audiograms suggested that the audiometric patterns of the m.1555A>G variant carriers in our cohort were predominantly ski-sloping, although some patients (YUHL206-21, 847-21, and 1054-21) exhibited a flat configuration (Fig. 2).
Fig. 2
Audiograms of m.1555A>G variant carriers. The transparent blue line depicts the individual thresholds, the average of the right and left ear (except for YUHL847-21 and 1054-21). The thresholds of the affected ear are indicated for YUHL847-21 and 1054-21. The black line represents the average of ten audiograms.
YUHL = Yonsei University Hearing Loss.
In general, the m.7444G>A variant is associated with hearing loss of varying severity, frequently in conjunction with the m.1555A>G variant or aminoglycoside exposure.151631 We identified two patients in our cohort with the m.7444G>A variant but none with the m.1555A>G variant. Additionally, none of the m.7444G>A carriers in our study were exposed to aminoglycosides. These results suggested that the m.7444G>A variant alone may occasionally result in hearing loss, even in the absence of the m.1555A>G variant or aminoglycoside exposure. One of the carriers of the m.7444G>A variant had a sporadic inheritance, whereas the other had a suspected maternally inherited familial inheritance (Table 3, Fig. 1D). None of the carriers of the m.7444G>A variant in our cohort presented with any additional syndromic symptoms (Table 3).
Several factors have been linked to the variable expressivity and incomplete penetrance of hearing loss in individuals affected by mitochondrial variants. These include heteroplasmy levels,30 environmental factors such as noise or aminoglycoside exposure,615 modifier genes such as TRMU,3233 and other accompanying mtDNA variations,1529343536 which can influence the onset, severity, and penetrance of hearing loss. To assess the role of the p. A10S variant in the TRMU gene as a modifier of m.1555A>G, we conducted direct sequencing of the TRMU gene in all patients with m.1555A>G variant. However, the p.A10S variant in TRMU was not detected in any of the ten individuals with the m.1555A>G variant. Intriguingly, although accurate records of aminoglycoside medication were impossible because of the retrospective nature of the history interviews, 7 of the 12 probands (58.3%) were not exposed to aminoglycosides, and none of the probands reported that their hearing loss was initiated by particular medications (Table 3). Heteroplasmy levels also influence the expressivity of the phenotype, particularly in the m.1555A>G variant.30 After detecting the m.1555A>G variant by PCR-RFLP in eight patients (YUHL16-21, 82-21, 206-21, 401-21, 680-21, 681-21, 668-21, and 1054-21), Sanger sequencing of the MTRNR1 gene was performed. All m.1555A>G variants in the eight patients appeared to be in a homoplasmic state (Supplementary Fig. 1), although low-level heteroplasmy could not be completely ruled out owing to amplification bias during PCR. In addition, the m.7444G>A variant in two patients (YUHL58-21 and 379-21) was confirmed by direct sequencing of the MTCO1 gene, and the m.7444G>A variant in both patients was in a homoplasmic state (Supplementary Fig. 1).
Penetrance was determined by dividing the number of affected matrilineal relatives by the total number of matrilineal relatives in the family and then averaging the results according to the variant type.7 In total, 14 individuals from 10 families affected by the m.1555A>G variant and 4 individuals from 2 families affected by the m.7444G>A variant were included in the segregation analysis and penetrance calculations (Fig.1C and D). The penetrance of hearing loss for the m.1555A>G variant ranged from 33.3% to 100%, with an average of 70.6%. Penetrance ranged from 33% to 67% in the two m.7444G>A variant-carrying individuals, with an average rate of 50%.
Haplogroup analysis of the mtDNA of the twelve affected patients
To determine whether mtDNA haplogroups influenced the variable expressivity of the mtDNA m.1555A>G and m.7444G>A variants, we amplified the HVR of the mtDNA genome and directly sequenced the PCR amplicons to identify the mtDNA haplogroups in 10 m.1555A>G and 2 m.7444G>A variant carriers. Four major haplogroups, namely, D, M, U, and B, were detected in the 12 pedigree patients (Table 3). In accordance with a previous report that analyzed the mtDNA haplogroups in Korean patients with hearing loss,7 haplogroup D was the most prevalent (6/12, 50%), followed by haplogroup M (4/12, 33.3%). Eight individuals were identified with haplogroups D5a2a1a, D5a3a1, M51, M7c1a2a1, M10a1a1b, M9a1a1, U6b3a, and B4c1b2a, whereas haplogroups D5a1 and D4e1a1 were identified in two individuals each.
In addition, we analyzed the distribution of haplogroups among 4,534 Korean control individuals. Macrohaplogroup D was the most prevalent lineage among these individuals, identified in 1,477 (32.57%) of them. The second most prevalent haplogroup was B (681 individuals; 15.01%), followed by M (14.18%) and G (405 individuals; 8.93%) (Supplementary Table 5). These results are consistent with previous findings regarding the prevalent mtDNA haplogroups observed in East Asians.2337
DISCUSSION
To our best knowledge, this study represents the most extensive analysis of the major mtDNA mutations associated with hearing loss. Li et al.6 screened 128 Chinese pediatric patients with hearing loss for mutations in the mitochondrial 12S rRNA gene and reported that approximately 2.9% of patients with nonsyndromic hearing loss carried the m.1555A>G variant. Yelverton et al.38 examined 2,434 probands with hearing loss in the United States and found that 3.5% had either MTRNR1 or MTTS1 mutation. Although the detection rate of deafness-causing mtDNA variants in our cohort (approximately 1.7%) was slightly lower than that reported previously, it is important to consider the impact of ethnic background, demographic composition of the cohort, and environmental factors on the differences in prevalence. For instance, our cohort consists predominantly of adults with an average age of 39.8 years, in contrast to the study by Li et al.6 that focused on pediatric patients. In addition, the hearing loss of our cohort ranged from mild to profound, in contrast to the cohort of Yelverton et al.38 in whom the majority had profound hearing loss.
Maternally transmitted mtDNA is frequently used to determine maternal ancestry and evolutionary distance. Haplogroups D, G, M, and B are the most common haplogroups in East Asia.2337 Previous studies by Lu et al.39 and Bae et al.7 revealed that haplogroup D is the most common haplogroup among m.1555A>G variant carriers. These findings are supported by the fact that haplogroup D was the most prevalent in our cohort, followed by haplogroup M. In our cohort, we identified numerous specific haplogroups such as D5a2a1a, D5a3a1, D5a1, D4e1a1M51, M7c1a2a1, M10a1a1b, M9a1a1, and B4c1b2a, as well as rare East Asian haplogroups such as U6b3a. However, no definite correlations among expressivity, penetrance, and mtDNA haplogroups were observed. This indicates that the mtDNA haplogroup does not influence the penetrance and expressivity of mtDNA mutations that cause deafness. Additional research employing a larger pedigree is required to determine the relationship between mtDNA haplogroups and the expressivity of deafness-causing mtDNA variants.
Patients with mtDNA m.1555A>G variant show variable expressivity, ranging from profound congenital hearing loss to adulthood-onset moderate hearing loss.728 In accordance with previous reports, the m.1555A>G carriers in this study exhibited varying onset (birth to age 50s) and severity (mild to profound). In contrast to earlier findings indicating that the m.1555A>G variant typically causes bilateral and symmetric hearing loss,72830 some m.1555A>G carriers (YUHL847-21 and 1054-21) in our study exhibited unilateral and asymmetric hearing loss, with the normal unaffected side. Additionally, a flat audiometric pattern was observed in some m.1555A>G carriers (YUHL206-21, 847-21, and 1054-21), whereas the stereotypical m.1555A>G audiogram exhibited a ski-sloping pattern. These results expand the phenotypic variety of the m.1555A>G variant. In addition, our data revealed that the average penetrance of the m.1555A>G variant was 70.6%, higher than the 54.1–65.4% reported in other studies.793940 Notably, none of the m.1555A>G carriers in our study reported exposure to aminoglycosides, suggesting that penetrance may be influenced by factors other than aminoglycosides.
Interestingly, one m.1555A>G carrier (YUHL401-21) was diagnosed with type 2 diabetes and hypothyroidism, whereas another carrier (YUHL668-21) displayed visual impairment. In a Chinese family with Leber’s hereditary optic neuropathy (LHON) and hearing loss, Wei et al.41 reported co-segregation of the MTND6 m.14484T>C and MTRNR1 m.1555A>G mutations in a Chinese family with LHON and hearing loss. In addition, Mezghani et al.42 identified the coexistence of MTND1 m.3308T>C and MTRNR1 m.1555A>G mutations, as well as multiple mitochondrial deletions, in two related Tunisian patients with MIDD. However, no study has linked the m.1555A>G variant as the sole cause of LHON or MIDD. None of the maternal relatives of the two patients (YUHL401-21 and 668-21) was diagnosed with type 2 diabetes or visual impairment, indicating that these conditions occurred independently. In our analysis, neither of the two patients (YUHL401-21 and 668-21) possessed any additional mtDNA variants such as m.14484T>C or m.3308T>C. Determining the functional contribution of the m.1555A>G variant to LHON and MIDD requires further research.
The pathogenicity of the m.7444G>A variant in hearing loss remains unknown because this variant alone is insufficient to cause a phenotype and requires additional modifiers such as the m.1555A>G variant or aminoglycoside exposure.151631 Notably, the m.7444G>A variant carriers in our cohort lacked the m.1555A>G mutation and were not exposed to aminoglycosides. The m.7444G>A variant modifies the stop codon of the CO1 gene and adds three additional amino acids (Lys-Gln-Lys) to the C terminus of the protein, potentially resulting in aberrant protein function.153139 Moreover, the m.7444G>A variant is located close to the 3’ end endo-nucleolytic processing site of L-strand polycistronic RNA precursors spanning tRNASer(UCN) and ND6 mRNA, which may result in splicing defects in RNA processing and a decrease in steady-state tRNASer(UCN) precursor level, similar to the m.7445A>G variant.4344 Our results indicated that the m.7444G>A variant may be the sole cause of hearing loss in certain ethnic and nuclear genetic backgrounds. Therefore, additional comprehensive functional investigations are required to establish the pathogenicity of the m.7444G>A variant in hearing impairments.
Aminoglycosides are commonly used to treat gram-negative sepsis,4546 infective endocarditis,47 and multidrug-resistant Mycobacterium tuberculosis infections.48 However, this medication may have adverse effects, including ototoxicity and nephrotoxicity.4950 In addition, patients with susceptible mtDNA mutations may experience hearing loss, even with a single therapeutic dose of aminoglycosides. The mtDNA variants m.1555A>G and m.7444G>A were detected in 16 individuals with unknown hearing phenotypes: 6 carried m.1555A>G (0.13%) and 10 individuals the m.7444G>A variant (0.22%) in the Korean control data. Therefore, 0.35% of the Korean population is at a risk of aminoglycoside-induced hearing loss based on this result. Before administering aminoglycosides, physicians should inquire about the history of hearing loss in the relatives of patients and screen for susceptible mtDNA variants if a suspicious family history is present.
In conclusion, this study presents a comprehensive examination of the frequencies of the main mtDNA mutations that cause deafness in East Asian populations. The detection rates of deafness-causing mtDNA variants such as m.1555A>G and m.7444G>A are consistent with those of previous studies, albeit with differences presumably caused by ethnic background, demographic composition, and environmental factors. This study also highlights the diversity of phenotypic expression associated with the m.1555A>G variant, such as variations in hearing loss onset, degree, and audiometric patterns. Additional medical conditions are observed in some m.1555A>G carriers, suggesting the involvement of multiple systems. The m.7444G>A variant is also analyzed, emphasizing the need for additional functional research to determine its pathogenicity in hearing loss. These findings improve the understanding of the genetic and clinical characteristics of hearing loss caused by mtDNA mutations.
 XML Download
XML Download