

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The aim of root canal therapy is to treat or prevent the development of apical periodontitis (AP) [1]. However, several factors such as the location, adequate disinfection, and filling of the canals followed by the restoration of the tooth can affect the accomplishment of this aim. Thus, adequate knowledge about the internal anatomy of the root and removal of the biofilm from the root canal system are of utmost importance [2].
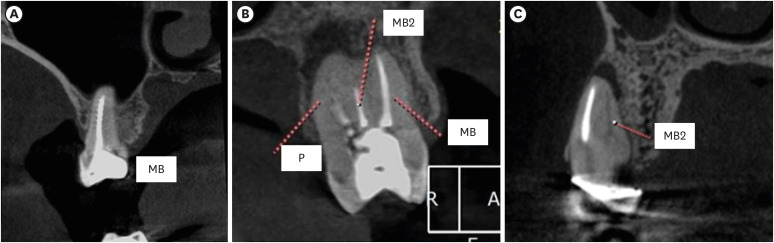
In humans, treatment of maxillary molars is often considered the most challenging, mainly due to the possible presence of a second canal in the mesiobuccal root, also known as the MB2 canal. Previously, in vitro destructive methodologies were used to study the internal anatomy, whereas currently, cone-beam computed tomography (CBCT) is considered as the best method available for in vivo applications [34]. CBCT images have indicated that the worldwide prevalence of the MB2 canal could vary from 48% to 98% [56].
Inadequate disinfection of root canals might lead to poor outcomes; this failure can be associated with an inadequate working length, insufficient root canal preparation, and failure in locating all the main canals [78]. Missed canals are considered one of the main reasons for root canal therapy failure [9]. In maxillary molars, a missed MB2 canal was found to be significantly associated with failure in endodontic therapy [1011].
The association between poorly disinfected canals and AP has been demonstrated via histological examination [1213]. However, the clinician has to rely on symptoms and radiographic images to reach an accurate diagnosis of AP. Even though bi-dimensional radiographs are easily available nowadays, they might lead to an inaccurate diagnosis [14]. A recent study using 250 µm voxel-size CBCT images, assessed the impact of root canal filling on AP; however, they concluded that further evaluations were required using smaller voxel sizes [10].
Thus, the present study aimed to assess the root canal anatomy of maxillary molars that underwent root canal treatment and to determine its association with the quality of the root canal therapy and the presence of AP.
MATERIALS AND METHODS
The research protocol used in this retrospective, observational study was reviewed and approved by the Ethical Committee of São Leopoldo Mandic School of Dentistry (#4.021.698). The images, taken for reasons not related to the present study, were selected from the database of a private radiology clinic.
The inclusion criteria were as follows: first and second maxillary molars with a mesiobuccal root and a history of root canal therapy, patient age, > 18 years old, presenting the included teeth in either right or left maxilla. The teeth should present with complete root development and the crown must have a restoration in position. The exclusion criteria were as follows: patients were under the age of 18 and those with immature apices, external root resorption, signs of fracture, and presence of metallic posts in the mesial roots. Images with artifacts in the crown or roots that prevented the proper visualization of the canals were also excluded. All images were obtained between 2015 and 2021 and assessed from March 2020 to February 2021.
The sample size was calculated considering the 95% confidence interval (CI), a statistically significant differences of 5%, and a proportion of prevalence of 70% for the first molars and 47% for the second molars. Consequently, taking into consideration a sample loss of 10%, a total of 359 and 426 MB canals were assessed in this study.
The Prexion 3D (Teracom, San Mateo, CA, USA) CBCT image scanner operating at 110 Kvp, 4 mA with a voxel size of 100 µm and field of view (FOV) of 5 × 5 cm was used.
Evaluation of the images
The images were simultaneously assessed by 2 dental specialists in oral radiology and endodontics, with more than 5 years of experience. The examiners used a high-definition screen Dell U2312HM DIGITAL (1,920 × 1,080, TrueColor 32 bits, 60 Hz) in a dark room, with a dedicated memory video board of 1,024 MB (Dell Inc., Austin, TX, USA). The OnDemand 3D (Cybermed, Irvine, CA, USA) software was used, wherein the evaluators could freely orient the images in any of the multiplanar reconstructions (axial, coronal, and sagittal). The contrast, brightness, and zoom were adjusted at the discretion of the evaluator. In case of disagreement, a third evaluator (specialist in oral radiology) discussed the case until a consensus was reached. The evaluators, including the third observer, were calibrated by assessing 100 images, and all discrepancies were discussed until a consensus was reached.
Initially, the anatomical feature of the root was assessed and classified from types I to VIII following Vertucci’s classification [15]. Furthermore, the presence of a second canal in the mesiobuccal root was registered. The quality of the root canal treatment was assessed and classified as follows: 1) no root canal filling present; 2) ideal filling located at 0–2 mm from the apex with no technical errors; 3) underfilled canal; 4) overfilled canal; 5) presence of zips or ledges; and 6) presence of voids.
The classification suggested by Estrela et al. [16] for AP was used in this study. In the absence of any radiolucency, the tooth was classified as “0.” When a periapical lesion was detected, the tooth was classified from 1 to 5 depending on the size of the lesion as follows: 1 (0.5–1 mm), 2 (1–2 mm), 3 (2–4 mm), 4 (4–8 mm), and 5 (> 8 mm). The categories “E” when expansion of the cortical bone was observed and “D” when destruction was observed were added to the classification when deemed applicable. The size was measured as the largest diameter of the lesion when observed in the coronal view using the ruler tool of the software.
Statistical analysis
The Kappa test was used for interobserver reliability. The association between the quality of the root canal treatment and the number of canals and foramina and the presence of AP and also the presence of AP with the number of canals, foramina, and Vertucci’s classification were calculated using the χ2 test or G test; the odds ratio (OR) and CI were used when required. SPSS 23 (SPSS Inc., Chicago, IL, USA) was used, and a p value of 0.05 was considered statistically significant.
RESULTS
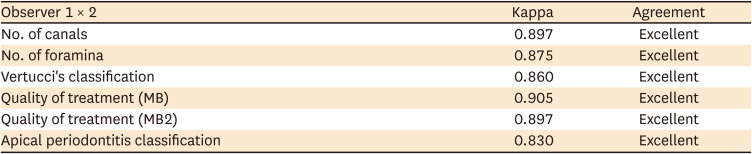
Overall, 1,549 canals from 1,000 mesiobuccal roots (692 [69.2%] first molars and 308 [30.8%] second molars) were assessed. The overall agreement between the examiners was considered excellent for all the parameters assessed (number of canals, number of foramina, Vertucci’s classification, quality of treatment in both the MB and MB2 canals, and presence of AP; Table 1).
Table 1
Kappa test showing excellent agreement rate between the observers at different variables
The prevalence of a single mesiobuccal canal was 45.1%, and 2 canals were observed in 54.9% of the teeth. A single foramen was observed in 60.7% of the teeth and 2 foramina in 39.3% of the teeth. Based on Vertucci’s classification, 44.7% of the teeth presented with type I configuration; 38.7% with type IV configuration, 15.9% with type II configuration, 0.6% with type V configuration, and 0.1% with type III configuration. None of the teeth presented with types VI, VII, and VIII configurations.
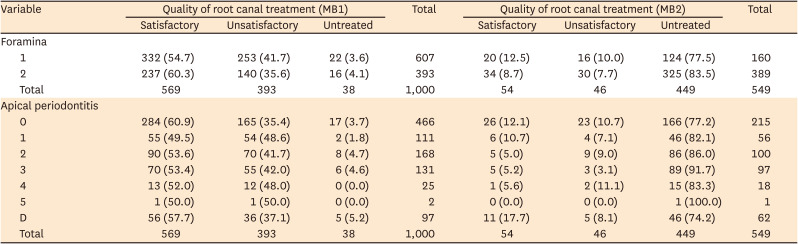
AP was detected in 544 roots (54.4%), and 466 (46.6%) teeth presented with intact bone. Of the 1,549 root canals, 623 (40.2%) presented with adequate fillings, 487 (31.4%) presented with no filling, and 439 (28.3%) presented with inadequate fillings (Table 2). Furthermore, 56.9% of the mesiobuccal canals were properly filled, 39.3% presented with inadequate fillings, and 3.8% were not filled. Similarly, 54 (9.8%) of the MB2 canals were adequately filled, 46 (4.6%) presented with inadequate fillings, and 449 (81.8%) were not filled. Table 3 depicts the overall classification of the quality of the filling in each root canal.
Table 2
Association between the number of foramina and quality of root canal treatment and association between the quality of root canal treatment and the classification of apical periodontitis
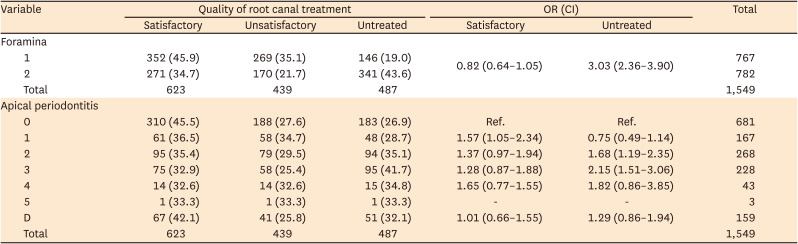
Table 3
Absolute number (percentage) of the quality of root canal treatment and prevalence of apical periodontitis in its different classifications
Association between the root canal anatomy and the quality of the root canal filling
The Chi-square test showed a statistically significant association between the number of foramina and the quality of the root canal treatment (p < 0.001) (Figure 1). The presence of 2 foramina increased the risk of untreated canals by 3.03 times. A total of 352 out of 767 (45.9%) canals with one foramen and 271 out of 623 (34.7%) canals with 2 foramina presented with satisfactory fillings. Furthermore, no root canal fillings were observed in 146 out of 767 (19%) canals with a single foramen and 341 out of 623 (43.6%) canals with 2 foramina; unsatisfactory fillings were observed in 269 canals (35.1%) with a single foramen and 170 canals (21.7%) with 2 foramina.
Association between AP and the quality of root canal filling
The periapical bone was normal in 681 (44.4%) canals out of 1,549 canals; among them, 310 (45.5%) canals presented with satisfactory root canal fillings. AP was observed in 868 (55.6%) canals, and 32.6% to 36.5% of them presented with satisfactory root canal fillings (Table 3).
A statistically significant association was observed between the quality of root canal treatment and the presence of AP (p < 0.05). The presence of unsatisfactory root canal fillings increased the risk of AP (classifications 1, 2, and 3 by 1.57, 1.68, and 2.15 times, respectively).
Association between AP and the number of root canals
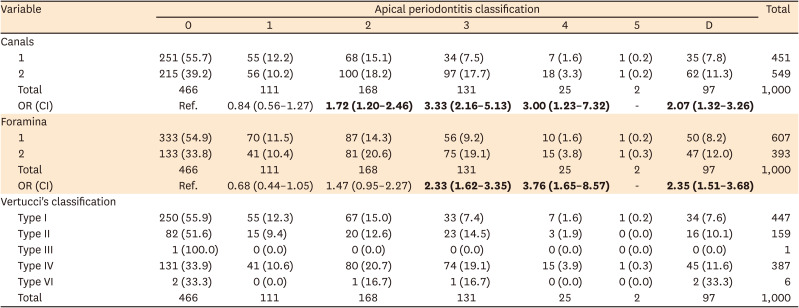
Among the 451 roots with a single canal, 251 (55.7%) presented with normal bone and 200 (44.3%) with AP; likewise, among the 549 teeth with MB2 canals, 215 (39.2%) presented with normal bone and 334 (61.8%) with AP. The risk of class 2, class 3, class 4, and class D AP was 1.72 (CI, 1.20–2.46); 3.33 (CI, 2.16–5.13), 3.00 (CI, 1.23–7.23), and 2.07 (CI, 1.32–3.26), respectively, in teeth with MB2 canals.
Association between AP and the number of foramina
Among the 607 roots with a single foramen, 333 (54.9%) had normal bone and 274 (46.1%) presented with AP; among the 393 teeth with 2 separated foramina, 133 (33.8%) had normal bone and 260 (66.2%) presented with AP. The risk of class 3, class 4, and class D AP in roots with 2 separated foramina was 2.33 (CI, 1.62–3.35), 3.76 (CI, 1.65–8.57), and 2.35 (CI, 1.51–3.68) times, respectively.
Association between AP and Vertucci’s classification
The classification 0 (absence of AP) was the most prevalent in teeth with Vertucci’s type I (55.9%), type II (51.6%), type III (100%), and type IV (33.9%) configuration. Among teeth with Vertucci’s type VI anatomy, no AP was detected in 33.3% of the teeth, whereas another 33.3% presented with class D AP. No association was observed between Vertucci’s classification and the presence of AP.
DISCUSSION
AP appears to be present in 50% of the population worldwide; although it is present in only 3% of the teeth in general, the incidence of AP is considerably higher in the posterior teeth [17]. In agreement with this previous result, in the present study, AP was observed in 54.4% of the teeth [17]. AP is related to cardiovascular disease and poor outcomes in pregnant women [1819]. A recent study demonstrated that high levels of C-reactive protein (CRP) are found in patients with AP [20]. High levels of CRP are correlated with the development of atherosclerotic plaque and serious systemic adverse effects [21]. However, proper root canal treatment, which includes the identification, adequate preparation, and filling of these teeth results in a decreased level of these proteins. The high prevalence of missed canals resulting in AP in the present study leads to the conclusion that it is important to address this issue in order to improve the health of the population.
The use of CBCT in dentistry was proposed by Mozzo et al. [22] the tri-dimensional aspect of CBCT images results in higher sensitivity for the detection of AP when compared to bi-dimensional radiographs. The interpretation of these images may vary depending on the experience of the observer; therefore, 2 observers certified in both oral radiology and endodontics were used in the current study [23]. Excellent agreement levels were reached with all the assessed parameters (Table 1). Such a level of agreement while discussing CBCT images was not reported in previous studies using dental students, residents, or oral radiologists [102324].
One of the greatest challenges during the treatment of maxillary molars is the possibility of encountering a second canal in the mesiobuccal root. Similar to the findings of previous studies using CBCT, 54.9% of the teeth in the current study presented with an additional canal [625]. However, it is important to emphasize that this finding might not reflect that observed in a clinical setting. A previous in vitro study showed that the combined use of microscopes and ultrasonic resulted in a MB2 visualization of 74% [26]. Furthermore, a previous clinical study have reported a higher prevalence of MB2 canals than that reported in the present study [27]. Parker et al. [28] demonstrated that troughing could lead to clinical negotiating in canals that were not visible in the CBCT scan. Some roots with a single canal, especially those with appropriate fillings and AP might consist of a second canal that is not visible in the CBCT scan.
Missed canals have been associated with AP. do Carmo et al. [10] used CBCT images to evaluate the presence of missed canals in a Brazilian subpopulation and found that 48.25% of the MB2 canals were missed in maxillary molars. However, the findings of the present study are not in accordance with the results of the aforementioned study. In the present study, untreated MB2 canals were detected in 81.8% of the teeth examined. This discrepancy might be due to differences in the CBCT acquisition; while the present study used a voxel size of 100 µm, the size used in the aforementioned study was 250 µm. Voxel sizes smaller than 200 µm are more reliable in detecting the internal anatomy variances in the case of a filled MB canal [29]. Moreover, the aforementioned study comprised 3 oral radiologists, while the present study employed 2 specialists in both oral radiology and endodontics.
A recent study reported that 98% of teeth with at least one missed canal, particularly the multi-rooted teeth, was affected by AP; AP was detected in 100% of teeth presenting with a missed canal [30]. The results of the present study showed that among the 449 missed MB2 canals (representing 81.8% of the total), 166 (37.0%) had a healthy periapical status and 283 (63.0%) had AP. The OR for AP in untreated canals was 3.03 (CI, 2.36–3.90). These results seem to be less impressive compared to those reported by Costa et al. (6.25; CI, 2.92–13.37) [30]. It may be inferred that an untreated MB2 with a foramen that merges with the main MB canal might not present with AP. Roots with 2 foramina were significantly associated with AP in the current study (Table 4).
Table 4
Association between the number of canals, foramens and Vertucci’s classification with the classification of apical periodontitis
This study has some limitations owing to the large sample size. It was not possible to determine whether the root canals were treated by an endodontist or a general dentist. In the case of posterior teeth, there is a higher risk of failure if the treatment is not performed by an endodontist [31]. Despite the improved sensitivity with regard to the diagnosis of AP in untreated root canals and filled roots, there is the possibility of over-diagnosis when CBCT images are used [32]. Additionally, properly filled roots with AP could be in the healing mode, which could lead to an overestimation of the results. Therefore, care should be taken before drawing conclusions related to the presented results and invasive and unnecessary procedures should be avoided [33]. A recent study showed that CBCT studies can be present with limitations associated with the image resolution (voxel size, focal distance, FOV), artifacts created by filling or restorations, and the possible movement of patients during scanning [34].
CONCLUSIONS
Thus, based on the findings of the present study, it can be concluded that AP is a very common occurrence in the mesiobuccal roots of endodontically treated maxillary molars. The occurrence of 2 canals or foramina increases the risk of untreated canals and presence of AP. Furthermore, the majority of MB2 canals are missed, and only a few of them receive satisfactory treatment.
 XML Download
XML Download