

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The infant mortality rate (IMR) is defined as the number of infants who die within the first year of life for every 1,000 live births in a given period. The IMR is considered a key indicator of the overall public health level because it has a strong correlation with medical factors such as infection and the quality of pre- and postnatal care as well as nonmedical exogenous factors such as nutrition, culture, and socioeconomic determinants of health.1
Although the IMR has significantly declined worldwide in recent decades, it has been reported that inequalities and disparities in the IMR still exist across and even within countries, with variations by race, ethnicity, state, and region. In the United States, infants born to black, non-Hispanic women had the highest IMR, and significant differences in infant mortality by state were also observed.234 The United Kingdom, Japan, Canada and China also have substantial geographic disparities in infant deaths associated with region and rurality.5678 Therefore, governmental efforts to reduce the gap in the IMR, including understanding the differences in infant mortality due to various factors and establishing proper interventions to reduce preventable infant deaths, are ongoing challenges in many countries.
Despite homogeneity of race, ethnicity, culture and geography in Korea, regional disparities in the overall public health level have been reported.910 Although the IMR has improved over time in Korea, little is known about regional differences in the IMR.11121314 Recently, pediatric departments have been experiencing a medical crisis due to the rapidly decreasing application rate of pediatric residents, resulting in a shortage of pediatricians.1516 Many hospitals have decided to temporarily not offer pediatric emergency, intensive care or hospitalization treatment due to a lack of medical staff, especially in noncapital areas.15 This phenomenon exacerbates regional inequalities in pediatric care accessibility and, in turn, may increase regional disparities in the IMR in Korea. A better understanding of the regional differences in the IMR is essential to establish proper interventions to resolve IMR disparities and reduce preventable infant deaths as well as to indirectly estimate the differences in the overall public health level among regions. However, little is known about regional differences in the IMR, and there are no studies that have well described descriptive statistics on regional disparities in the IMR in Korea.
Therefore, in this study, we aimed to examine whether there are regional disparities in the overall and cause-specific IMR in Korea using vital statistics. We also investigated the differences in IMR trends by region in terms of both rate differences (RDs) and rate ratios (RRs).
METHODS
Data sources
All mortality and population data were extracted from the Korean Statistical Information Service database between 2001 and 2021. The number of deaths at age 0 by the underlying cause of death based on International Classification of Diseases 10th Revision codes was extracted for each year and region. Population data by region were obtained from the mid-year population for each year. The level of regional classification was limited to 17 administrative divisions (provinces and metropolitan cities) for data stability. However, Sejong was excluded from the present study, which started generating data after 2012, so we only calculated IMRs between 2012 and 2021. Since 2001, vital statistics have been supplemented through infant cremation report data and neonatal death data. Therefore, data before 2001, which were many missing infant deaths, were excluded from the analysis.9
Statistical analysis
First, the average IMRs per 1,000 population by region were calculated from 2001 to 2021 to determine whether there were regional disparities in the IMR in Korea. The relative regional disparities in the IMR were identified through the RRs using the region with the lowest IMR as a reference group. The standard errors were calculated using the Taylor series expansion method to obtain the 95% confidence intervals (CIs) of the RR.17
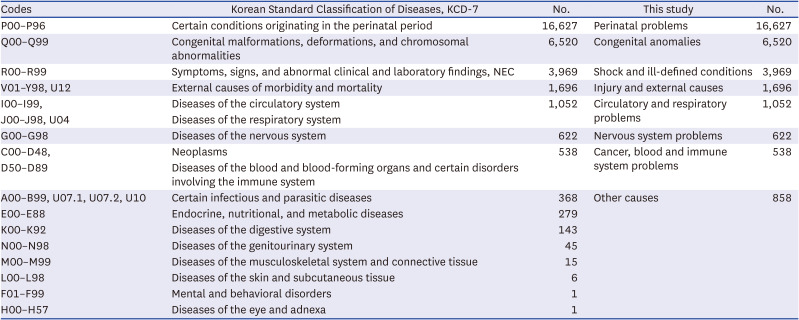
Second, infant mortality attributable to regional disparities between 2001 and 2021 was analyzed by cause of death. The cause of death was classified, considering the number of infant deaths by cause in Korea between 2001 and 2021 and clinical relevance (Table 1). The expected number of deaths was calculated by applying the IMR of the reference group by cause of death to the number of births in each region. The mortality attributable to regional disparities was presented as excess deaths and the region-specific population attributable fraction, defined as the fraction of excess deaths divided by observed deaths compared with the reference group. The 95% CIs of the fraction were obtained using Monte Carlo simulation under the assumption of a Poisson distribution.18
Table 1
Causes of death (code classification)
Finally, an analysis of regional disparities in IMR trends was conducted. Previous studies have reported that the IMR in Korea has been continuously declining, and we analyzed the IMR trend in 16 provinces and metropolitan cities using the Joinpoint regression method to confirm whether the IMR trends in each region are similar.11121314 The annual percent change (APC) in the IMR by region was calculated. More specifically, a maximum of two join points was set for each model, and the average APCs (AAPCs) were calculated for each segment.1920
Joinpoint regression can analyze decreasing trends in infant mortality by region, but it is difficult to accurately represent regional disparities in infant mortality trends. Therefore, the 21-year period from 2001 to 2021 was divided into 3 periods of 7 years each (period 1: 2001–2007, period 2: 2008–2014, period 3: 2015–2021), and the relative and absolute difference trends were examined to obtain the RRs and RDs in the IMR trend by region compared to those of the reference group. Monte-Carlo simulation was performed using R version 4.2.2, and Joinpoint Regression Program version 4.9.1.0 (National Cancer Institute, Bethesda, MD, USA) was used for Joinpoint regression analysis.
Ethics statement
The Institutional Review Board (IRB) of Kyungpook National University Chilgok Hospital reviewed the protocol of this study and approved an exemption, the requirement for informed consent was waived because of the nature of public data from the Korean Statistical Information Service database (IRB No. 2023-02-006).
RESULTS
Regional disparities in the IMR between 2001 and 2021
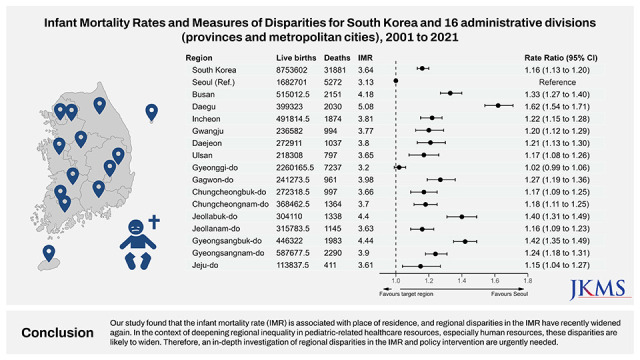
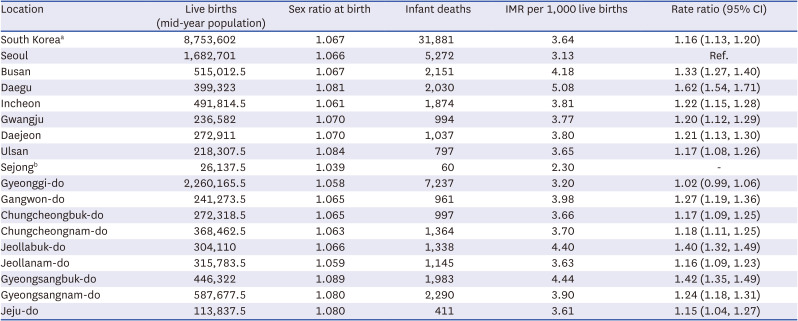
Excluding Sejong, there were a total of 8,753,602 live births and 31,881 infant deaths in Korea from 2001 to 2021. The overall IMR in Korea was 3.64 per 1,000 live births between 2001 and 2021. Significant regional differences in IMRs were observed over the study period, and the IMR in metropolitan cities and provinces ranged from 3.13 per 1,000 live births in Seoul to 5.08 per 1,000 live births in Daegu.
The relative regional disparities in the IMR in Korea were assessed with RRs and 95% CIs and compared between Seoul, which was defined as the reference group because it had the lowest IMR in Korea, and the other 15 regions. The 14 regions showed significantly higher IMRs than Seoul, with RRs ranging from 1.15 (95% CI, 1.04–1.27) in Jeju-do to 1.62 (95% CI, 1.54–1.71) in Daegu. Only the IMR in Gyonggi-do, which is located adjacent to Seoul and one of the Seoul Capital Areas, was not significantly different compared to that of Seoul (RR, 1.02; 95% CI, 0.99–1.06). Interestingly, Gyeongsangbuk-do, which is located adjacent to Daegu and often referred to as Daegu-Gyeougbuk, had the second highest IMR (4.44 per 1,000 live births) and RR (RR, 1.42; 95% CI, 1.35–1.49). The IMRs in Jeollabuk-do (RR, 1.40; 95% CI, 1.32–1.49), Busan (RR, 1.33; 95% CI, 1.27–1.40), and Gangwon-do (RR, 1.27; 95% CI, 1.19–1.36) were also relatively high (Table 2).
Table 2
IMRs and measures of disparities for South Korea and 17 administrative divisions (provinces and metropolitan cities) (2001–2021)
Total and cause-specific excess infant mortality by region
Between 2001 and 2021, 14.0% (95% CI, 13.6–14.4) of infant deaths in Korea were attributable to regional disparities. If Seoul's IMR was applied to all live births in Korea, 4,455 infant deaths could have been prevented. In Korea, 16.1% of the deaths due to perinatal problems (P00–P96), 6.3% of the deaths due to congenital anomalies (Q00–Q99), 8.3% of the deaths due to shock and ill-defined conditions (R00–R99), 35.9% of the deaths due to injury and external causes (V01–Y89, U12), 19.9% of the deaths due to circulatory and respiratory problems (I00–I99, J00–J98, U04), 11.3% of the deaths due to nervous system problems (G00–G98) and 7.0% of the deaths due to cancer and blood problems (C00–D98) were attributable to regional disparities. If this is expressed as the number of excess deaths compared to Seoul, it corresponds to 2,675, 413, 328, 609, 209, 71, 38, and 114 deaths, respectively. Perinatal problems comprised the greatest portion, accounting for 60% (2,675/4,455) of all excess infant deaths. The main causes of excess infant death were perinatal problems, congenital anomalies and injury and external causes, which accounted for 83% (3,697/4455) of excess infant deaths in Korea (Table 3 and Fig. 1).
Table 3
Infant mortality attributable to regional disparities for South Korea and 16 administrative divisions (2001–2021)
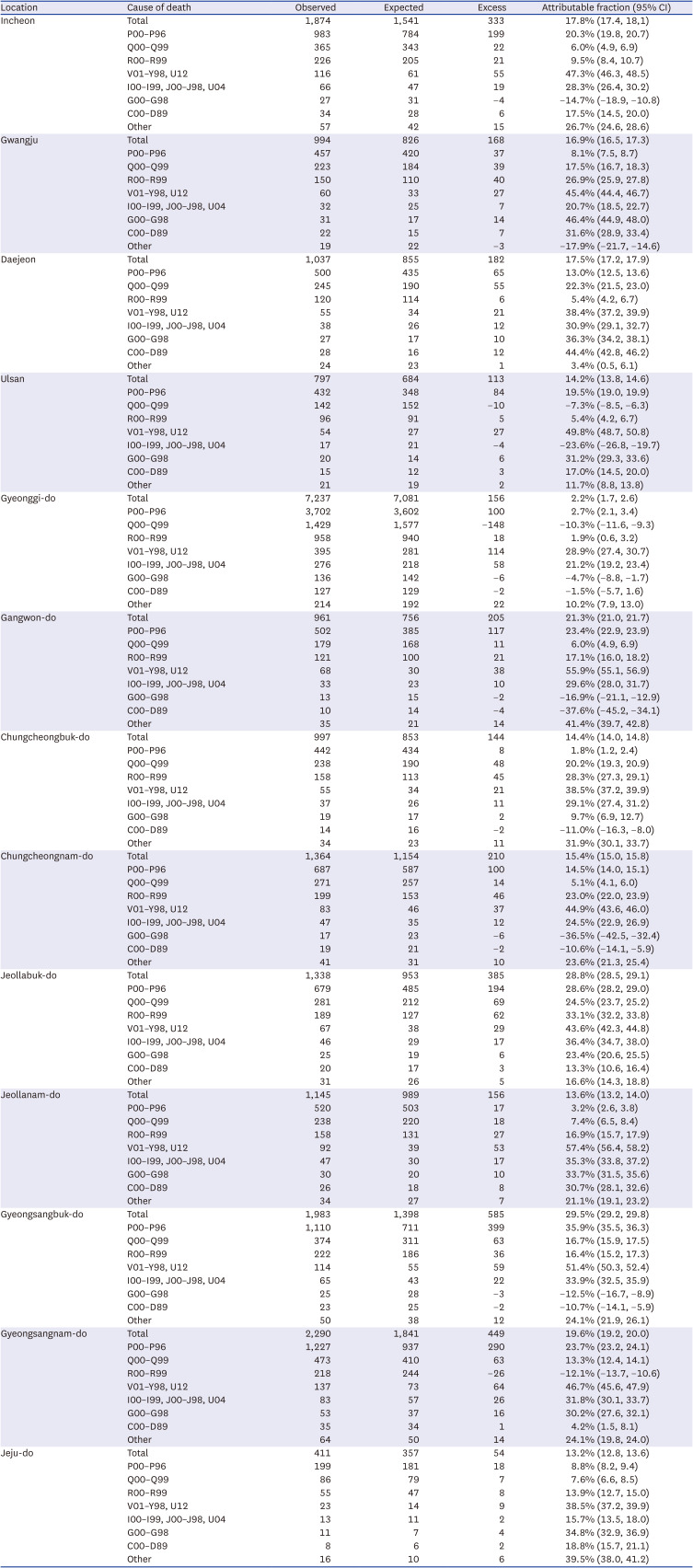
Fig. 1
Estimated excess number of deaths attributable to regional disparities and disease distribution in Korea.
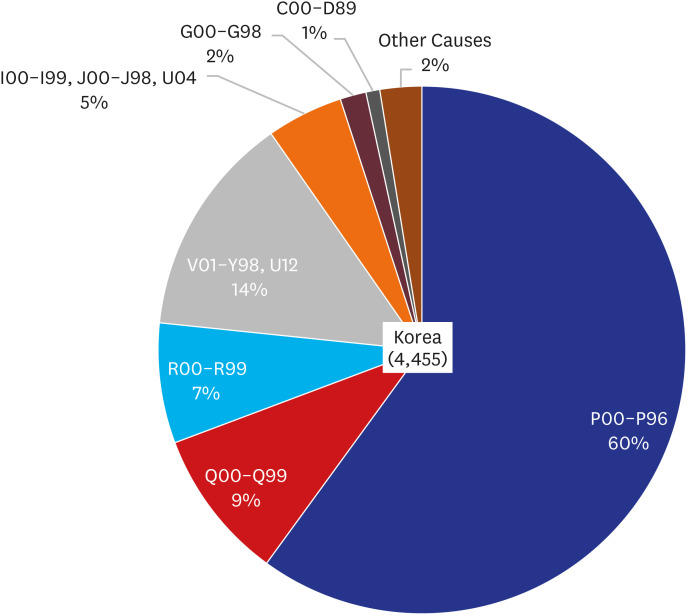
Regional disparities attributable to infant deaths ranged from 2.2% (95% CI, 1.7–2.6) in Gyeonggi-do to 38.4% (95% CI, 38.1–38.6) in Daegu. Perinatal problems were the leading cause of excess infant deaths in all regions except Gwangju, Gyeonggi-do, Chungcheongbuk-do, and Jeollanam-do. In Daegu and Gyeongsangbuk-do, where the number of excess infant deaths was the highest, perinatal problems accounted for 84.7% (660/779) and 68.2% (399/585) of the total excess infant deaths, respectively. Shock and ill-defined conditions in Gwangju, congenital anomalies in Chungcheongbuk-do, and injury and external causes in Gyeonggi-do and Jeollanam-do were the leading causes of excess infant deaths (Table 3). Overall, the proportion of excess deaths due to perinatal problems was high in the metropolitan cities (metropolitan cities: 68% vs. provinces: 53%), and the proportion of excess deaths due to injury and external causes was high in the provinces (metropolitan cities: 9% vs. provinces: 18%) (Supplementary Fig. 1).
Overall and regional trends in the IMRs between 2001 and 2021
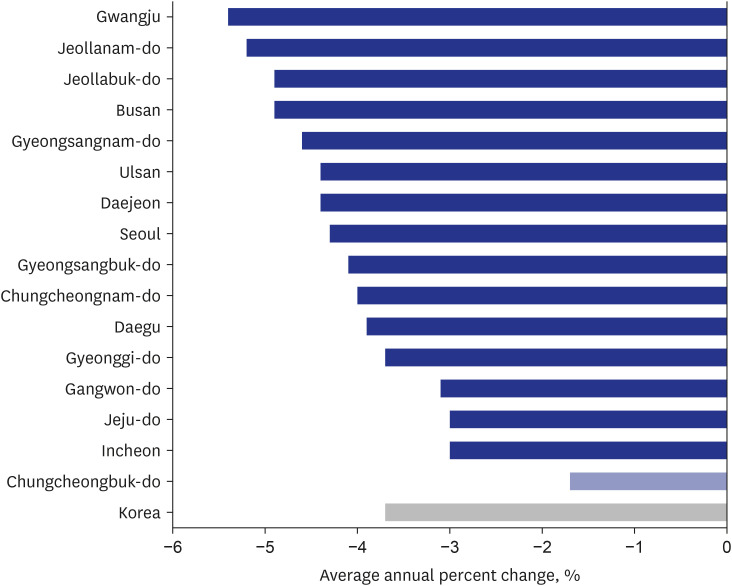
The overall IMR in Korea significantly decreased over the study period (AAPC, −3.7%, 95% CI, −4.6%, −2.7%). The IMR decreased significantly in all regions except Chungcheongbuk-do, and the AAPCs ranged from −5.4% (95% CI, −6.7%, −4.0%) in Gwangju to −3.0% (95% CI, −3.6%, 2.3%) in Incheon. Specifically, the trend of change in the overall IMR in Korea showed that the IMR decreased rapidly between 2003 and 2008 (APC, −8.0%), but the rate of decline slowed between 2008 and 2021 (APC, −2.5%). During the same period, Seoul's APC was −4.3%, which means that, on average, the overall disparity in the IMR compared to that in Seoul decreased at the beginning of the observation period, but the overall disparity in the IMR compared to that in Seoul increased again after 2008. Excluding Seoul from the calculation of infant mortality in Korea, the gap has widened slightly since 2008 (Fig. 2 and Supplementary Figs. 2, 3).
Fig. 2
Changes in the infant mortality rate in Korea (2001–2021). Dark blue and gray bars indicate statistical significance (P < 0.05).
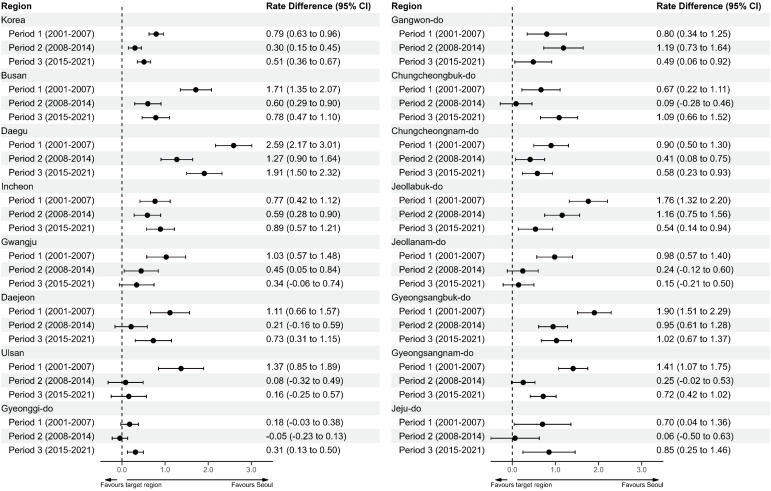
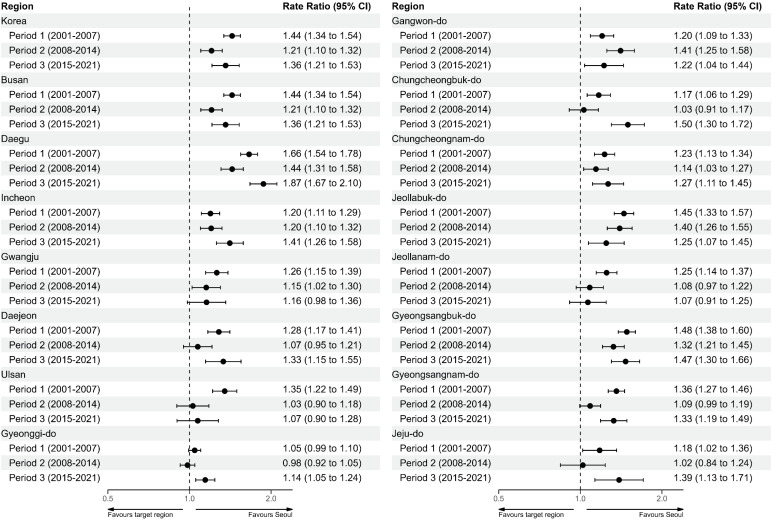
The absolute and relative regional disparities in IMR trends were compared between Seoul (reference group) and the other 15 regions using RRs and RDs with 95% CIs according to period (Figs. 3 and 4). In Korea, there was a decrease in the RD and RR from period 1 (between 2001 and 2007) to period 2 (between 2008 and 2014) followed by an increase from period 2 (between 2008 and 2014) to period 3 (between 2015 and 2021). By region, the RDs and RRs were similar to the overall trend in Korea, but in Gwangju, Jeollabuk-do, and Jeollanam-do, the RDs and RRs decreased throughout the study period. In Gangwon-do, the RD and RR increased from period 1 to period 2 and decreased from period 2 to period 1. Supplementary Figs. 4 and 5 present cause-specific IMR trends during the study period.
DISCUSSION
We examined regional disparities in the IMR in Korea using cause of death statistics from the National Statistical Office, which covers the entire country. There have been discussions about the regional disparities in the IMR in Korea, but little is known about this issue.
We identified that regional disparities in the IMR exist in Korea. The region with the lowest IMR between 2001 and 2021 was Seoul; except for that in Gyeonggi-do during period 2, the IMR was consistently low in Seoul compared to other regions from period 1 to period 3. Considering the proportion of excess deaths due to perinatal problems in other regions, the low IMR in Seoul can be mainly explained by the lower IMR due to perinatal causes compared to those in other regions. Notably, as reported in previous studies, Korea’s IMR has been declining; the relative and absolute disparities have tended to increase in recent years.11121314 This is because the decline in IMR in other regions has slowed compared to that in Seoul, and various causes, including the distribution of medical resources, social determinants of health, and the physical environment, need to be considered to determine the cause.21
Although our study focused on the phenomenon of regional disparities in the IMR rather than on causal relationships, regional differences in the IMR can be explained indirectly through the causes contributing to excess mortality. The perinatal problems that contributed the most to excess mortality and regional disparities in this study were related to maternal causes such as age, obesity, and smoking, fetal sex and ethnicity, prenatal care, socioeconomic status, and the protocol and capacity of neonatal intensive care units (NICUs).2223242526272829 According to previous studies, the factors affecting the mortality of children and adolescents in developed countries were divided into 4 domains: intrinsic (biological and psychological) factors, the physical environment, the social environment, and service delivery.30 Applying this classification to the risk of perinatal mortality, factors related to perinatal problems are mainly related to social environment and service delivery, except for fetal sex, which is classified as an intrinsic factor. Regarding fetal sex, many studies have reported that the perinatal mortality rate of boys is higher than that of girls.2329 In Korea, the sex ratio at birth in Seoul is lower than that in other regions, and although recently alleviated, it has been reported that Daegu and Gyeongsangbuk-do, where the preference for sons is strong, have a high sex ratio at birth.31 In particular, between 2001 and 2021, which was the study period, the sex ratio at birth was high on average in the Gyeongsang province area. Although fetal sex was classified as an intrinsic factor, in a study that analyzed the sex ratio at birth and parents' social status, it was found that since the late 1990s, the higher the parents' social status, the lower the sex ratio at birth. This means that the sex ratio at birth not only acts as a biological factor but is also affected by the social environment.32 Sidebotham et al. reported that the social environment has the greatest effect on child mortality among the 4 domains.30 Regarding perinatal mortality, social determinants affect maternal pregnancy and postpartum well-being, which in turn will affect perinatal mortality.263334 A cohort study reported that the regional deprivation index correlated with the IMR in Korea, and metropolitan areas had negative excess mortality and negative deprivation indices compared to local provinces.35 In a Japanese study that analyzed trends in perinatal mortality, the reduction in perinatal mortality in Japan was largely attributed to the reduction in early neonatal mortality, which was explained by improved NICU capacity, effective interventions to save neonates, and improved quality of treatment.28 In our study, although the IMR is improving in Korea, there is still a regional gap compared to Seoul, suggesting that service delivery needs to be considered. Due to the nature of healthcare resources, which cannot be stored and are produced and consumed simultaneously, regionalization and risk-appropriate healthcare delivery are important, especially during the perinatal period when transport can be a risk factor that increases mortality.36 In addition, low accessibility due to physical distance to healthcare centers can contribute to regional disparities. Several studies have reported on the relationship between the distance to healthcare centers and neonatal prognosis.373839 Several studies have reported on regional disparities in healthcare resources related to NICUs, and although there have been improvements, regional disparities, particularly in human resources, are still a problem.164041
Disparities in the IMR at the regional level have also been studied in other countries.34567 In a study comparing IMRs between southern states and states in other regions of the United States, the southern states had a higher IMR than the states in other regions (7.37 vs. 6.19 per 1,000 live births), and the three main causes of excess mortality were sudden unexpected infant death (SUID), prematurity, and congenital anomalies.3 In another study conducted in the United States, the IMRs were 5.43 per 1,000 live births in large metropolitan areas, 6.31 in medium/small metropolitan areas, and 6.67 in counties in nonmetropolitan areas, and SUID and congenital anomalies were the main causes of excess mortality.4 Interestingly, in both studies, prematurity, not SUID, was the main cause of excess mortality in black infants, which means that regional disparities cannot simply be generalized and a contextual approach is needed. In most regions in Korea, perinatal problems accounted for the highest proportion of excess deaths, but in some regions, external causes, shock and ill-defined conditions, and congenital anomalies contributed the most to excess mortality. The contribution of external causes to excess mortality was greater in provinces than in metropolitan areas, suggesting the need for an improved physical environment in provinces.
This work has several limitations. First, there have been concerns about the validity of death certificates. Cause of death statistics from the National Statistical Office are based on death certificates and may be inaccurate because of underreporting or misreporting. However, we used infant mortality data after 2001 when underreporting was corrected using cremation data and neonatal death data. In addition, death certificates in Korea are written by a physician, and according to research, the accuracy of the cause of death was relatively accurate at 91.9%.942 Second, our analysis was limited to examining the phenomenon of disparities in IMRs among regions and only presented interpretations post hoc. Further research is needed to analyze the relationship between etiological factors, such as gestational age, birth weight, race, and statuses, and the IMR to understand the mechanism of regional disparities in the IMR and to suggest appropriate policies.
Our study found that the IMR is associated with place of residence, and regional disparities in the IMR have recently widened again. In the context of deepening regional inequality in pediatric-related healthcare resources, especially human resources, these disparities are likely to widen. Therefore, an in-depth investigation of regional disparities in the IMR and policy intervention are urgently needed.
 XML Download
XML Download