

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Since the publication of the report “To Err Is Human” by the US Institute of Medicine in 1999, interest in patient safety has increased in the medical field, and has become a policy priority.12 Accordingly, various policies to improve patient safety have been recommended, and increased resources for related research are also being considered.345 However, despite the importance of patient safety, it is still challenging to specify the level of patient safety comprehensively and accurately.6 It is essential to develop measures of patient safety and calculate them in a way that is comparable to other fields or disciplines to prioritize and determine the allocation of resources for patient safety compared to other diseases.78
Measures of the burden of disease are commonly used to prioritize services and research in healthcare sectors.91011 These include the most intuitive way to measure the economic burden, such as cost of illness indicators, as well as comprehensive methods, such as the Summary Measures of Population Health (SMPH) index, which is an indicator that combines the health impacts of death and prevalence. There have been attempts to measure the disease burden of patient safety adverse events, and the economic burden has been estimated intermittently.12131415 In addition, in recent studies on the Global Burden of Disease, the adverse effects of medical treatment (AEMT) were added to the list of causes of disease, and patient safety issues were measured using disability-adjusted life years (DALYs), a type of SMPH.716
Although disease burdens for various diseases and injuries have been measured, measurement of the disease burden due to adverse events are not often undertaken. In addition, the methodology for measuring the disease burden due to adverse events comprehensively and reasonably has not been established. For example, Global Burden of Disease studies are concerned about underestimating or overestimating DALYs due to the AEMT because of the limitations of sources that contain data on limited types of adverse events and diagnostic codes.7 Even in studies that estimated the economic burden of disease due to adverse events, the estimated costs were highly variable.12131415
Accordingly, this study aimed to develop a standard methodology that can more systematically measure the burden of disease due to adverse events. It used the results of medical record reviews, which is a representative method of identifying the status of patient safety, and is commonly used as a gold standard. Specifically, this study utilized the scale and characteristics of preventable adverse events identified in the Patient Safety Incidents Inquiry (PSII), conducted to accurately monitor patient safety at the national level,1718 and estimated DALYs and economic cost.
METHODS
Data source
The Patient Safety Act was enacted in 2016 and requires the Korean government to conduct a PSII every five years to estimate the incidence of adverse events at the national level. This study used the first PSII, undertaken in 2019, as the primary data source. This described adverse events according to sex and age in 7,500 patients from 15 regional public hospitals. PSII used 3-stage retrospective medical records review to increase the validity of adverse event identification. More specific details about PSII are described in other studies.1718 However, data from 191 patients whose sex and age were not recorded in PSII were included after imputation that considered the sex and age distribution ratios among the total patients. The parameters used in the analysis are summarized in Supplementary Table 1.
Preventability of adverse events and prolongation of hospitalization
In this study, preventable adverse events identified in the PSII, or the patients who experienced them, were the units of analysis. In the PSII, two physician reviewers independently determined the preventability scores of each adverse event (no evidence of preventability-1 point to clear evidence of preventability-6 points) and preventability meant whether an adverse event could be prevented based on currently available medical evidence.17 A score of 4 or higher was considered a preventable adverse event. In this study, among the preventability scores evaluated by the two reviewers, the minimum standard was defined when they used a minimum value, and the maximum standard was defined when they used a maximum value. The results for each criterion were presented. If a patient experienced two or more adverse events, the event with the highest preventability was set as the representative event for the analysis using patients as the unit of analysis, and the most severe harm due to an adverse event was set as a representative value. Also, in the PSII, the adverse event final review committee classifies the degree of harm caused by an adverse event into five categories (temporary harm, long-term hospitalization, permanent harm, need for life support, and death), and the prolonged hospitalization period was divided into five categories. In this study, the median of the prolonged hospitalization days for each category was re-coded as follows: “5 days or less” was re-coded as three days, “6–10 days” as eight days, “11–15 days” as 13 days, “16–20 days” as 18 days, and “21 days or more” as 21 days.
DALY calculation
The DALY due to a preventable adverse event was calculated as the sum of the years lived with a disability (YLD) and years of life lost due to premature mortality (YLL). This study estimated the DALYs of patients who experienced adverse events according to an incidence-based approach.9 The YLD calculation was based on patients who suffered harm to a degree of permanent disability (other than death) and more due to preventable adverse events. Here, the disability weight applied was 0.362 (95% confidence interval, 0.306–0.420),19 the value of AEMT calculated in previous studies. Since YLD was calculated in units of 5 years, the average age of onset was assumed to be the median value of the age group. Considering that disabilities are permanent, the morbidity period was set as a lifetime, but the morbidity period at onset was assumed to be 2.5 years, half of 5 years of age. To increase comparability with previous studies, the time discount rate (3%) and age weight (4%) applied in previous studies were used.20 The YLL calculation was based on patients who died from preventable adverse events. Since the PSII utilizing 2016 data used a patient as the unit of analysis, this study also used the Complete Life-Table of 2016 and applied a time discount rate (3%) to calculate YLL.2021 Thereafter, DALYs due to preventable adverse events, by sex and age groups, were calculated by summing YLD and YLL. The DALY calculated from 7,500 patients from PSII was extrapolated to the entire Korean population as of 2016, converted to DALYs per 100,000 population, and compared with the results of previous studies.20
Estimation of economic costs
To estimate the economic cost of the preventable adverse events, re-coded extended hospital-stay information for preventable adverse events, identified as extended hospital stays in the PSII, was summarized. In addition, the average daily medical cost for each major disease was calculated using the main disease information of each patient collected from PSII and the average medical costs by disease category and age group in Korea’s National Health Insurance Statistics Yearbook.22 The increased medical expenses for each preventable adverse event were calculated by multiplying these values (recoded extended hospitalization information and average daily medical costs). Since a patient can experience two or more adverse events, the total economic cost due to adverse events in PSII was calculated as the sum of the increased medical costs of each adverse event. Furthermore, by using the information on the number of hospital discharges by disease categories in the 2016 medical service usage data,23 information on the occurrence of adverse events by primary diagnosis identified in PSII, and the total economic cost due to adverse events by patients, the economic cost due to adverse events within the entire population was extrapolated.
RESULTS
DALYs
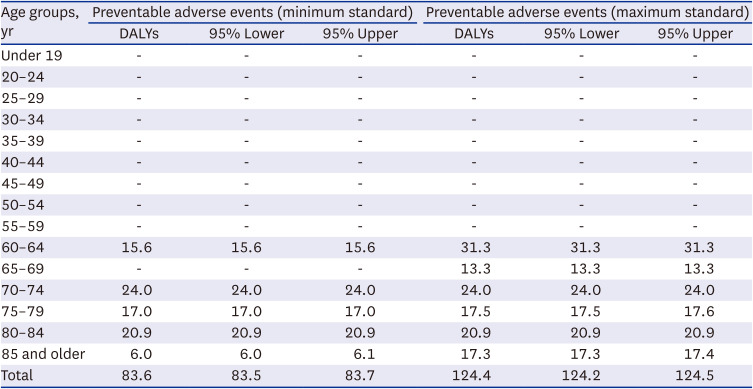
The number of patients with permanent disabilities due to preventable adverse events by the minimum standard was one (male) out of the total of 7,500 PSII patients. The associated YLD was 0.37. The number of patients with permanent disability due to a preventable adverse event by the maximum standard was two (one male, one female), and the associated YLD was 0.86. Nine patients (six males and three females) died from preventable adverse events by the minimum standard; the associated YLL was 83.2. A total of 13 patients (eight males and five females) died from preventable adverse events by the maximum standard, and the associated YLL was 123.5. The total DALYs was 83.6 by the minimum standard and 124.4 by the maximum standard (Table 1).
Table 1
Estimated DALYs of patients who experienced preventable adverse events in the Patient Safety Incident Inquiry
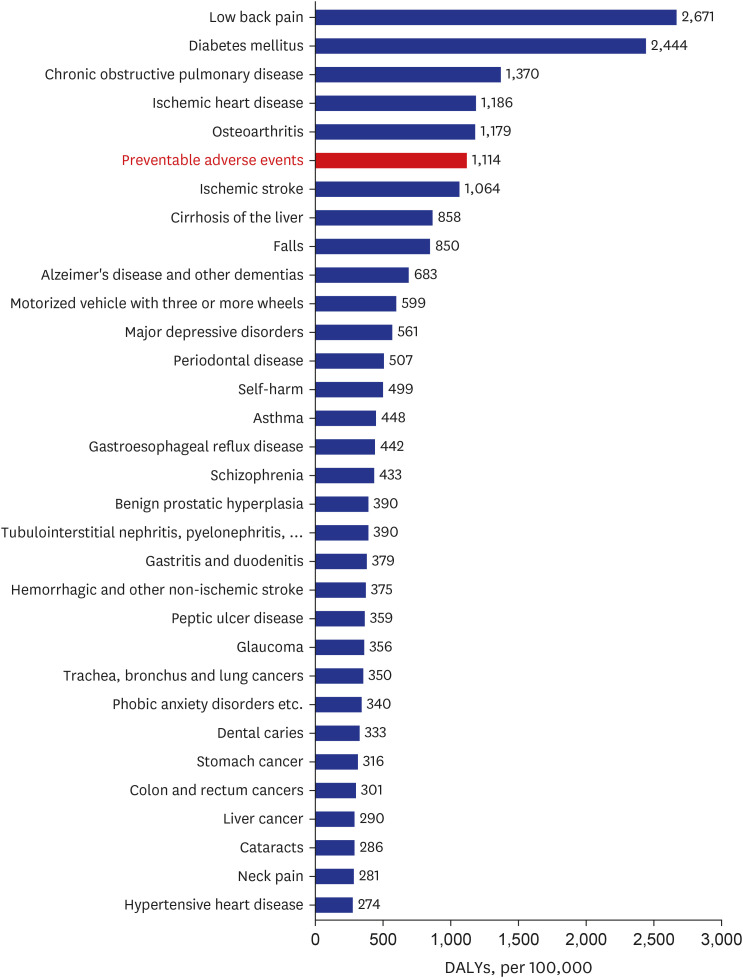
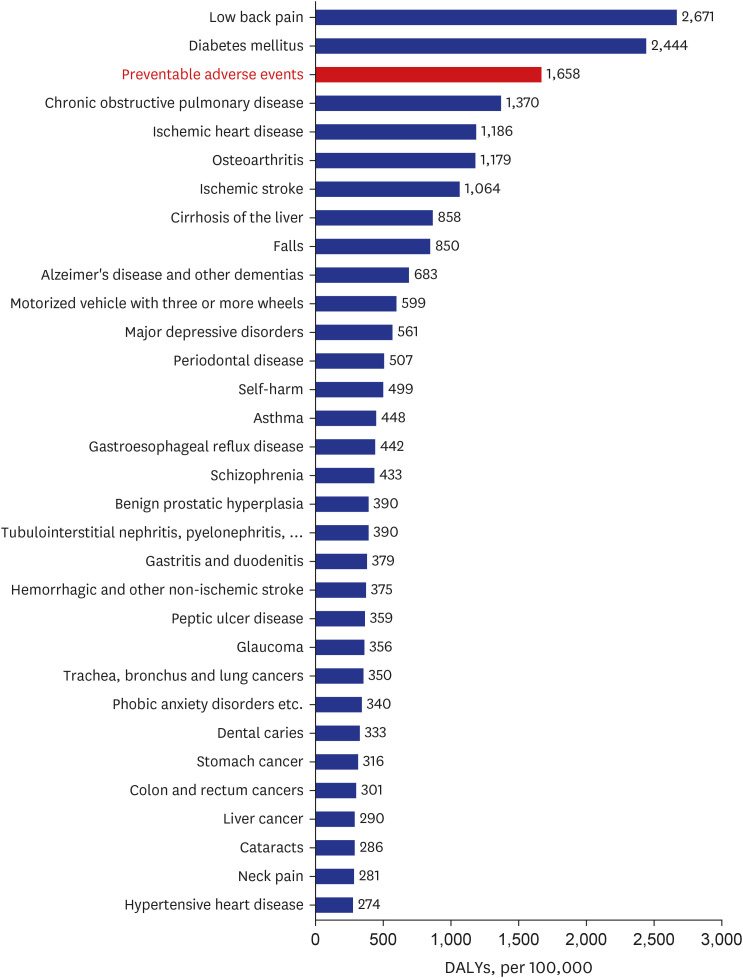
When estimating DALYs due to preventable adverse events across the whole of Korea, the estimated DALYs per 100,000 population was 1,114.4 by the minimum standard. This was in sixth place, after back pain, diabetes, chronic obstructive pulmonary disease, ischemic heart disease, and degenerative arthritis, when compared to the 2015 Korean Burden of Disease results (Fig. 1). The estimated DALYs per 100,000 population, based on the maximum standard, was 1,658.5. This was in third place, after low back pain and diabetes, compared to the results of the same study (Fig. 2).
Economic costs
By the minimum standard, in terms of the increased number of days of hospitalization and medical costs due to preventable adverse events by sex and age, prolonged hospitalization was longest in males aged 60–64 and 70–74 years, with an average of 1.9 days (Table 2). In addition, the increased medical costs were found to be approximately Korean Republic Won (KRW) 470,000 (380 US dollars), on average, for those aged 70–74 and approximately KRW 330,000 (260 US dollars), on average, for those aged 60–64. The average number of prolonged hospitalization days for females was 3.3 days in the 25–29-year age group, with an increased medical cost of approximately KRW 1.66 million (1,300 US dollars) on average.
Table 2
Estimated medical costs in patients with prolonged hospitalization due to preventable adverse events in the Patient Safety Incident Inquiry
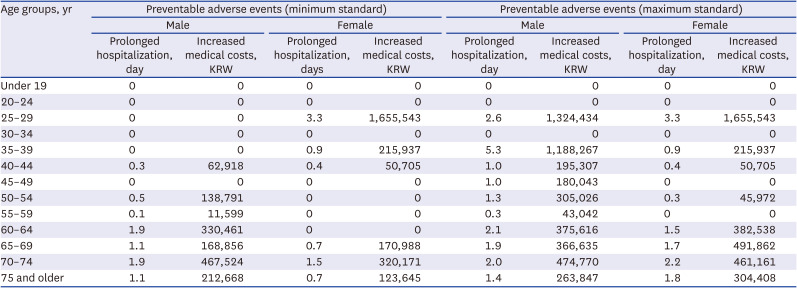
By the maximum standard, for the increased number of hospitalization days and medical costs due to preventable adverse events by sex and age, the prolonged hospitalization days were the longest in males aged 35–39 years, with an average of 5.3 days. In addition, the increased medical costs were approximately KRW 1.19 million (950 US dollars) on average in the 30-39-year age group, and approximately KRW 1.32 million (1,100 US dollars) in the 25–29-year age group. The average number of prolonged hospitalization days in females was the longest, at 3.3 days, in the 25–29-year age group, and the increased medical cost was approximately KRW 1.66 million (1,300 US dollars) on average in the 25-29-year age group and approximately KRW 490,000 (390 US dollars) in the 60–65-year age group.
The increased number of hospitalization days annually in 2016 due to adverse events is estimated to be about 4 million days, about 730,000 days when the minimum preventability standard is applied, and about 1.44 million days when the maximum standard is used (Table 3). The annual medical cost due to adverse events in 2016 was estimated to be approximately KRW 870 billion (700 million US dollars). The medical expenses due to preventable adverse events were approximately KRW 150 billion (120 million US dollars) by a minimum standard and approximately KRW 300 billion (240 million US dollars) by a maximum standard.
Table 3
Estimates of prolonged hospitalization days and increased medical costs due to adverse events for a year in 2016

DISCUSSION
This study estimated the DALYs and economic costs due to preventable patient safety adverse events using the PSII results that identified the scale of adverse events at the national level. To summarize the results, the DALYs due to preventable adverse events in Korea in 2016 was 1,114.4 per 100,000 population at the minimum standard and 1,658.5 per 100,000 population at the maximum standard. In addition, the annual prolonged hospitalization days due to preventable adverse events were estimated to be approximately 730,000 days at the minimum standard and about 1.44 million days at the maximum standard. The increase in annual medical costs in 2016 due to preventable adverse events was estimated at KRW 150 billion (120 million US dollars) at the minimum standard and approximately KRW 300 billion (240 million US dollars) at the maximum standard.
Attempts to measure disease burden in the patient safety area have continued.7812131415 Still, there were limitations, such as data availability for specific areas only or invalid estimated values due to limited data sources. This study is significant in that it suggests a standard methodology that can calculate the disease burden due to adverse events more systematically by using PSII as the data source, which uses a medical record review methodology to estimate the scale of adverse events more accurately. In other words, this study showed that it is possible to measure the disease burden due to patient safety more accurately if we utilize not only the information on the occurrence of adverse events collected in PSII, but also information on preventability, degree of harm, and the resulting prolonged hospitalization period. Since research to identify the scale of adverse events at the national level using the medical record review methodology is steadily being conducted in other countries,24 cross-country comparisons of disease burden due to patient safety can be more valid by applying the method used in this study.
When the DALYs due to preventable adverse events estimated in this study were compared with the 2015 Korean burden of disease study,20 the ranking was third in terms of the maximum standard and sixth in terms of the minimum standard. This study found that the disease burden due to preventable adverse events was considerable, and the problem of patient safety is no less important than that of other major diseases, such as diabetes and chronic obstructive pulmonary disease. Furthermore, since disease burden studies generally do not calculate DALYs based on whether the condition is preventable, if the DALYs for the adverse events are calculated, the ranking is expected to be higher. Considering that the purpose of disease burden research is to allocate resources in line with the current disease burden, it is necessary to evaluate whether current healthcare policies on patient safety are being drafted and implemented according to the scale of disease burden and to pay more social attention to patient safety issues.
Estimating the burden of disease using the disease cost index helps publicize patient safety issues more practically by transforming patient safety issues into cost issues.12131415 In other words, calculating the cost of disease due to adverse events emphasizes that reducing medical harm to patients is not only the right thing for patients but also financially desirable. Thus, it gives more power to persuade the healthcare field, and other sectors, of the importance of patient safety. This may explain why it is easier to find studies that have attempted to estimate the cost of disease due to adverse events than studies that have used SMPH, an indicator that considers both morbidity and mortality, to calculate the disease burden for patient safety issues. Although there may be a variety of methods for estimating the cost of disease due to an adverse event, estimating the cost associated with prolonged hospitalization due to an adverse event is a conservative approach and a less controversial methodology.1314 Therefore, the cost of adverse events estimated in this study is a conservative value. Since it costs at least this much, it can be emphasized that more attention should be paid to patient safety.
The cost of preventable adverse events calculated in this study was approximately 1% of total hospitalization costs in Korea in 2016 (minimum standard: 0.7%, maximum standard: 1.3%). When considering total adverse events, without distinguishing preventability, it was about 3.6% (approximately KRW 870 billion). According to the 2015 economic burden of disease study in Korea, the cost of diseases caused by colon and rectum cancers was about 2.7 trillion won (2,172 million US dollars), and alcohol use disorders were approximately 2.4 trillion won (1,888 million US dollars).25 At first glance, the cost of disease due to preventable adverse events appears to be less than the cost of these diseases. Still, the difference may not be so significant if only direct costs are considered because these costs are the sum of both direct and indirect costs. In addition, since the cost of disease due to preventable adverse events estimated in this study can be theoretically zero, patient safety should be prioritized in the healthcare field from an economic point of view, just as the patient safety issues identified in the DALYs are significant.
Although this study tried to present a standard methodology that could calculate the disease burden due to patient safety more systematically, there are still limitations that need to be improved methodologically. First, when calculating YLD due to preventable adverse events, only cases of disability due to permanent harm were considered, and cases of temporary harm or long-term hospitalization were not considered in YLD calculation. This would have underestimated the YLD calculation, but the increase in YLD is not expected to be so large because the disability weight in case of temporary harm or long-term hospitalization will be smaller than that of permanent disability, and the duration of disease will be shorter. However, in the future, it is necessary to calculate disability weights that can reflect disability caused by adverse events in a more diverse way, that is, with more subdivided severity. If disability weights with subdivided severity are used, it will be possible to more reasonably estimate the burden of disease due to adverse events.26
Another limitation is that indirect costs, such as those due to productivity loss, were not considered in the cost of disease due to preventable adverse events estimated in this study. In addition, when estimating the costs due to the prolonged hospitalization, the cost can be calculated more accurately by considering additional tests and procedures. It is worth considering a method of collecting data on the costs of additional tests or procedures performed due to adverse events in the PSII.
In this study, preventable adverse events and economic costs were estimated using the results of medical record reviews, which is the most representative and standardized method for estimating the scale of adverse events at the national level. The results of this study indicate that we need to pay more attention to the issue of patient safety. In addition, if the more standard method of systematically calculating the burden of disease due to patient safety proposed in this study is used, it is possible to compare the burden of disease due to patient safety adverse events among different countries and to demonstrate the importance of patient safety globally. In addition, since PSII is scheduled to be conducted repeatedly in Korea, it is necessary to continuously calculate the burden of disease due to adverse events by using the information on the occurrence rate and characteristics of adverse events identified in PSII. Although this study presented a standardized method for estimating the burden of disease in patient safety, research on estimating the burden of disease in patient safety is still lacking compared to other disease groups. It is hoped that future studies estimating the disease burden due to patient safety will be conducted repeatedly.
 XML Download
XML Download