

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Rathke’s cleft cysts (RCC) are benign sellar and/or suprasellar lesions arising from the remnants of the Rathke pouch [1]. Symptomatic RCC presenting with mass effect is usually managed surgically by draining the cyst contents with or without biopsy, while complete removal of the cyst wall is sometimes performed [2]. However, the recurrence of RCC is frequently observed with the reported rates from 0% to 42%, and there is no consensus over the most effective surgical method [34]. Some authors suggest aggressive surgical resection of the entire cyst wall to prevent cyst recurrence, but such an approach has been found to be associated with higher rates of postoperative endocrine dysfunction [56].
The intrinsic characteristics of RCC have been studied by many authors in an attempt to explore factors associated with cyst recurrence. Among them, the presence of squamous metaplasia is widely accepted as the most significant causative factor for recurrence [35678]. In fact, in their long-term follow-up study, Kinoshita et al. [9] suggest that the recurrence of RCC is independently associated with the presence of squamous metaplasia, but not with the surgical procedure.
Recently, a close relationship between aggressive RCC and craniopharyngioma has been suggested, and the possibility that these cystic ectodermal lesions represent a continuum has gained popularity over the last two decades [10]. In this paper, we present a case of recurrent RCC, which was initially thought of as craniopharyngioma, and discuss several relevant factors associated with cyst recurrence, including histological characteristics.
CASE REPORT
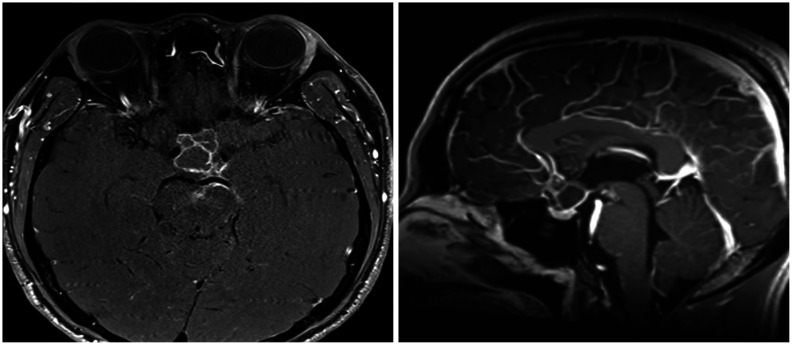
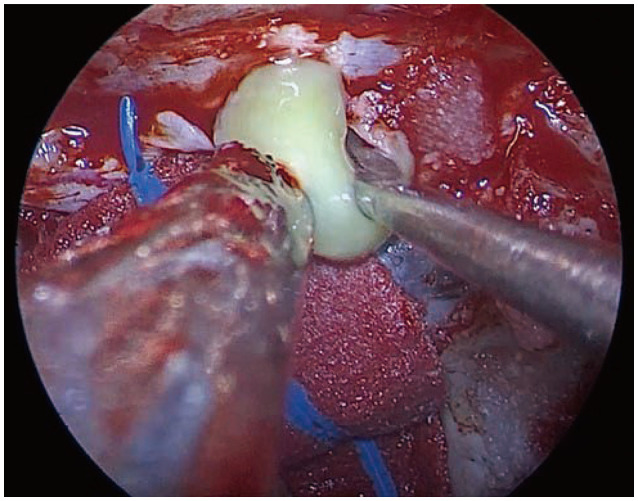
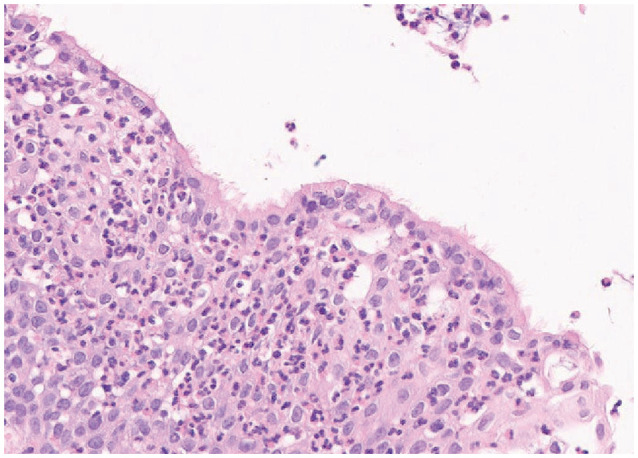
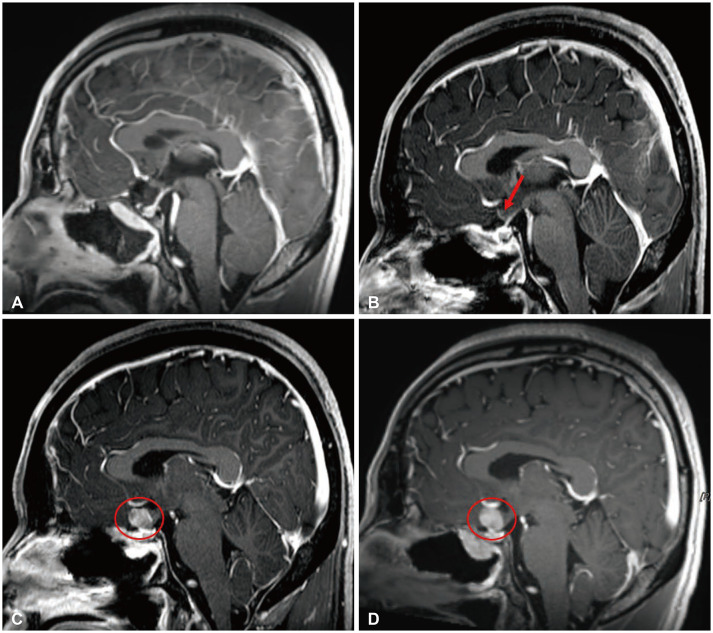
A 33-year-old male patient presented with a sudden worsening of headache and visual symptoms for two weeks. His initial MRI showed about 1.8×1.5×2.3 cm sized, mostly cystic, suprasellar mass compressing the optic chiasm. The mass also showed peripheral rim enhancement on contrast-enhanced T1-weighted MRI (Fig. 1). On admission, basal hormone level was checked and visual field analysis was also done, and both results were normal. Based on the preoperative information, suprasellar craniopharyngioma was highly suspected. Tumor removal via endoscopic extended transsphenoidal approach was performed. The tumor consists of mostly yellow mucoid with some solid portions and gross total resection (GTR) was done while preserving the pituitary stalk (Fig. 2). Intraoperative frozen section biopsy favored the diagnosis of craniopharyngioma. Postoperative MRI showed no immediate complications and the patient’s initial symptoms improved and he was discharged at postoperative day 9. Unexpectedly, the final pathological diagnosis confirmed RCC rather than craniopharyngioma (Fig. 3). Outpatient follow-up with MRI was done 3-months postoperatively and a slightly enhancing small suprasellar lesion was seen. His 1-year postoperative MRI explicitly showed recurred cystic mass at the suprasellar area, which was also seen on his 1.5-year postoperative MRI (Fig. 4). Since the patient was asymptomatic, and the size of the recurred mass did not change significantly, close observation with subsequent MRI follow-ups was planned instead of surgical intervention.
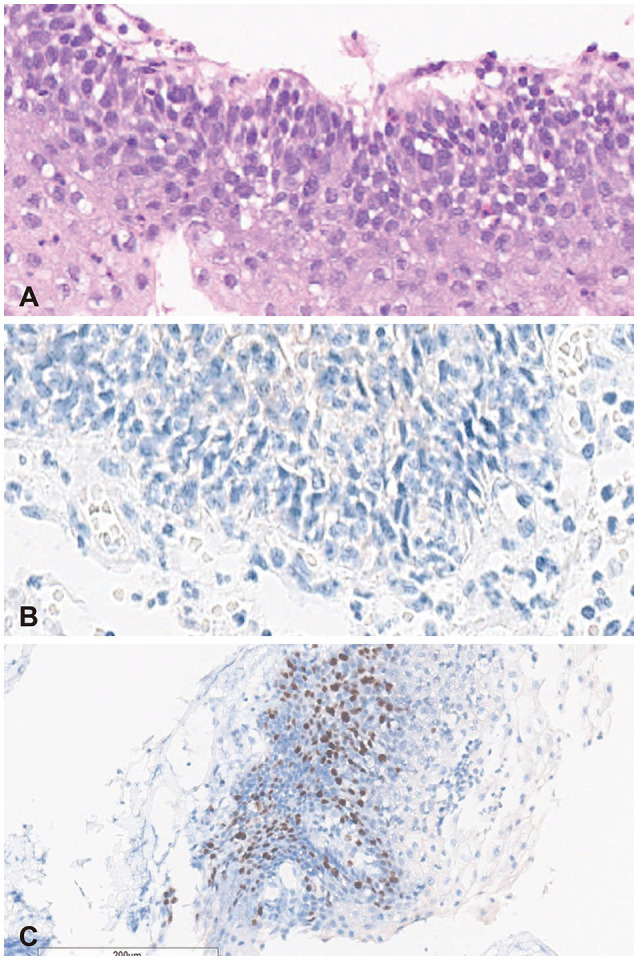
Since early recurrence of RCC following surgery seemed unusual, additional histopathological tests were done. To differentiate from craniopharyngioma, BRAF V600E mutation and β-catenin mimmunohistochemical studies were performed and the results were negative. Further histopathological studies showed the presence of squamous metaplasia and high Ki-67 proliferation index (15%) (Fig. 5).
DISCUSSION
RCC are typically asymptomatic, but sometimes present with clinical symptoms such as headache (50%), visual loss (46%–55%), and endocrine dysfunction (70%) [11]. As in our case, symptomatic RCC are usually managed surgically, and several surgical techniques have been utilized in order to treat symptomatic RCC. Radical opening of the cyst wall with full evacuation of the cyst contents was first suggested by Fager and Carter [12] in 1966. In 1984, Baskin and Wilson [13] recommended that simple transsphenoidal drainage and partial removal of the cyst wall is a safe and effective treatment option, and more recently, surgical marsupialization has been employed to drain cyst contents into sphenoid sinus [14]. In order to reduce recurrence, a more aggressive surgical resection is often performed, however, controversy exists on whether GTR is necessary since this radical approach is more frequently associated with postoperative diabetes insipidus and hormonal defects [5611].
Cyst characteristics including inflammation, presence of stratified epithelium, squamous metaplasia, high proliferation index (Ki-67), and cyst wall enhancement on MRI have been suggestive of factors associated with cyst recurrence. Epithelial changes may occur due to repeated intracystic inflammation which could lead to transition from typically single columnar or cuboidal RCC epithelium to stratified, squamous epithelium. When compared to single, columnar epithelium, stratified and squamous epithelium possess higher potential of proliferation and high rate of positive Ki-67 distribution [15]. Above all, the presence of squamous metaplasia has been proposed as the most important risk factor for recurrence [356789]. In fact, RCC with squamous metaplasia show more aggressive nature, and their potential association with craniopharyngioma has been advocated by several authors [101516].
Craniopharyngiomas are relatively common locally aggressive neoplasms that arise from squamous epithelia cell rests occurring anywhere along the craniopharyngeal duct, the canal that connects the stomodeal ectoderm with the invaginating Rathke’s pouch [1718]. In their study, Alomari et al. [10] presented a unique case of a 7-year-old boy whose postoperative pathology showed histologic features of both RCC and craniopharyngioma, suggesting a progressive transformation from RCC to craniopharyngioma [10]. Moreover, in 2014, Ogawa et al. [15] presented a case of a 47-year-old male patient who underwent two consecutive surgeries in 7-month period, due to repeated expansion of a suprasellar cyst. The patient was diagnosed with RCC at the first surgery but was found to be craniopharyngioma after the second surgery which also supports the above viewpoint [12]. Interestingly, both cases showed squamous metaplasia within their RCC components.
In our case, unusual early recurrence of RCC was noted and further molecular and histopathological studies were necessary for accurate diagnosis. Our patient showed negative V600E mutation in the BRAF oncogene which is a well-recognized factor that is identified in 95% of cases of papillary craniopharyngiomas [19]. Moreover, we noted high proliferation index (Ki-67) of 15% which also suggests more aggressive tumor nature and potential recurrence in the future. We believe further studies on the molecular pathogenesis of these lesions are required to clarify underlying mechanism of cyst progression. Unfortunately, it is difficult to predict whether the cyst will show aggressive nature or not until postoperative histologic characteristics are revealed. As in our case, intraoperative frozen biopsy could misdiagnose RCC with craniopharyngioma. Therefore, the presence of rim enhancement on preoperative contrast-enhanced MRI could be an important finding which may suggest inflammation, vessel proliferation, and recurrence potential, as proposed by several authors [711].
This case report of recurrent RCC provides additional support to current understanding of factors associated with aggressive nature RCC. Patients with symptomatic RCC whose histopathological studies show squamous metaplasia and high proliferation index (Ki-67) should be closely followed postoperatively and cyst wall enhancement on contrast MRI may provide valuable information regarding recurrence potential of the cyst.
 XML Download
XML Download