

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Various modalities have been used to treat hepatocellular carcinoma (HCC), including surgical resection, local tumor ablation, liver transplantation, transarterial chemoembolization (TACE), and molecular-targeted therapy.1 In patients with very early or early-stage solitary HCC with adequate hepatic function reserves (Child-Pugh class A) and without major vascular invasion, surgical resection is recommended as the best treatment based on the Barcelona clinic liver cancer (BCLC) staging system.2 However, for patients who are not candidates for surgical resection or liver transplantation, radiofrequency ablation (RFA) or microwave ablation is considered the preferred treatment due to its safety and minimal invasiveness. Recently, updated BCLC guidelines included TACE and transarterial radioembolization (TARE) for early-stage HCC when resection, surgery, or liver transplantation has failed or is not feasible.2
Surgical resection and RFA yield similar progression-free survival (PFS) and overall survival (OS) outcomes in patients with early-stage HCC.2 RFA is a widely used first-line treatment for early-stage HCC in favorable locations3; however, RFA of unfavorably located lesions, such as periportal HCC, subphrenic HCC, or HCC adjacent to the intestines or major vessels, is associated with an increased risk of post-procedural complications4 and local tumor progression (LTP) because of an insufficient ablative margin around the hepatic vessels.5
Drug-eluting bead TACE (DEB-TACE) has the advantages of slow and steady release, high local concentration, and lower incidence of adverse drug reactions than conventional TACE (cTACE).6 The use of DEBs aims to improve the drug delivery system and embolic material, which are problems in cTACE, while maintaining the basic principles of TACE. Theoretically, DEB-TACE could become an acceptable treatment for HCC by controlling anticancer drug reflux to the whole body through reversible ionic exchange of the cancer drug and drug vehicle, and by maximizing a constant concentration of the anticancer drug delivered to the inside of the tumor and periphery of the tumor bed for a certain period.78 Many earlier studies and meta-analyses comparing DEB-TACE and cTACE reported that procedural safety was better in DEB-TACE than cTACE, with fewer side effects and a lower incidence of liver and systemic toxicity.9
Previous studies have shown no significant difference in therapeutic effects, OS, or major complication rates between cTACE and RFA.101112 One short-term study addressed differences between RFA and DEB-TACE for patients with early-stage HCC.13 However, no large comparative study of RFA and DEB-TACE has conducted a long-term follow-up or performed survival analysis. Therefore, the purpose of this study was to compare the long-term therapeutic outcomes of RFA with those of DEB-TACE as a first-line treatment for a single small (≤ 3 cm) HCC.
METHODS
Patients
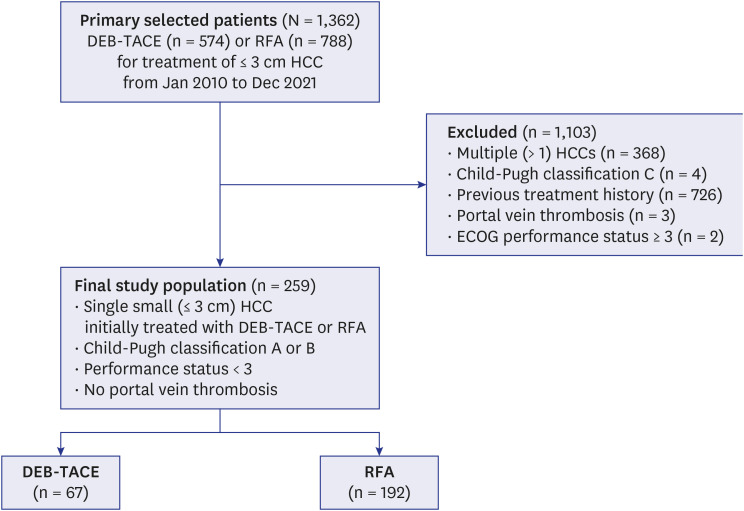
From January 2010 to December 2021, 574 patients with HCC underwent DEB-TACE and 788 underwent ultrasound (US)-guided percutaneous RFA at our institution for early-stage HCC measuring 3 cm or smaller in their greatest dimension. Based on our hospital’s routine practice for patients with small HCC (≤ 3 cm in size, ≤ 3 in number), US-guided RFA was considered when a patient was ineligible for surgical resection or because of the patient’s preference. Patients who were not candidates for RFA or surgery were considered for TACE. DEB-TACE is the preferred method of TACE at our institution because it has a better pharmacokinetic profile than cTACE in patients with advanced age, comorbidities, and decreased liver function. The decision to perform DEB-TACE was ultimately made by the interventional radiologist after a multidisciplinary discussion of each patient.
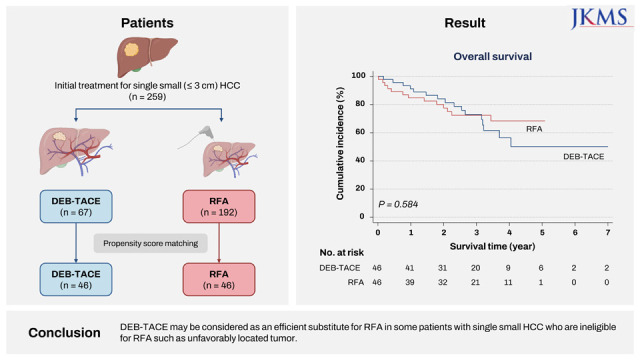
As shown in Fig. 1, this comparison study excluded the following patients: 1) patients with multiple (> 1) HCCs; 2) patients with Child-Pugh class C liver function; 3) patients who had received any other treatment (e.g., surgical resection, intervention, chemotherapy, radiotherapy, targeted therapy, or immunotherapy) for HCC before the initial DEB-TACE or RFA treatment and the first imaging follow-up; 4) patients with portal vein thrombosis; 5) patients with extrahepatic metastasis or large vessel invasion; and 6) patients with an Eastern Cooperative Oncology Group performance status ≥ 3. Finally, 259 consecutive patients were enrolled in this study; among whom, 192 underwent RFA and 67 underwent DEB-TACE as a first-line treatment for single nodular HCC measuring ≤ 3 cm at their greatest dimension on computed tomography (CT). HCC was diagnosed according to a percutaneous biopsy or typical imaging findings based on current clinical criteria.214
DEB-TACE protocol
DEB-TACE was conducted by three interventional radiologists with at least 5 years of experience. A 5-Fr catheter (Yashiro; Terumo, Tokyo, Japan) was introduced through the right common femoral artery to assess the arterial anatomy and to identify arteriovenous shunts and the feeding arteries of the tumor by the superior mesenteric artery, celiac axis, and common hepatic artery through angiography. After locating the feeding arteries, superselective catheterization was performed using a 2- or 1.7-Fr microcatheter (Valoute, Asahi Intecc, Seto, Japan; Progreat, Terumo). Subsequently, taking 30 mL of non-ionic iodized contrast agent (Xenetix®; Guerbet, Aulnay-sous-Bois, France), a mixture of 50 mg doxorubicin (Adriamycin; Ildong, Seoul, Korea) and one vial of 70–150 μm (DC Bead®; Biocompatibles UK, Farnham, UK) was injected slowly at a rate of approximately 1 mL/min into the tumor under fluoroscopic guidance (Allura Clarity FD20; Philips Healthcare, Best, The Netherlands) to avoid reflux and non-target embolization. The total dosage of DEBs for the procedure was established by the interventional radiologists considering the size of the tumor, with a maximal dose limit of 100 mg of doxorubicin per patient. The particles were injected until stasis of arterial flow to the tumor was observed. The procedure was performed according to the Society of Interventional Radiology Reporting Standards for transcatheter therapy for HCC to ensure consistency.15
Percutaneous RFA protocol
After planning US, RFA was performed percutaneously with real-time US guidance by one of two experienced radiologists, each of whom had at least 10 years of experience performing this procedure at the time of the study. All patients received local anesthesia with 2% lidocaine HCL (lidocaine; Gwangmyeong Pharmacy, Seoul, Korea) at the RF electrode entry point before treatment, and fentanyl (fentanyl; Hana Pharmacy, Seoul, Korea) was administered intravenously in 2 mL for moderate sedation.
In cases where the tumor was located near the diaphragm or colon, artificial ascites were introduced using normal saline under US guidance. A 3-channel RF generator (480-kHz VIVA multi RF Generator; STARmed, Goyang, Korea) with either single (STARmed) or separable clustered electrodes (Octopus electrode; STARmed), and an internally cooled electrode system with a 3-cm exposed tip (STARmed) was used based on the tumor size or location. The aim of RFA was to obtain at least 0.5 cm of normal hepatic parenchyma surrounding the tumor as a tumor-free margin in as many cases as possible.
Follow-up after initial treatment
In the DEB-TACE group, three-phase (arterial, portal, and equilibrium phases) contrast-enhanced CT (CECT) was performed within 1 month after the initial treatment and every 3 months thereafter for the first 2 years. Follow-up visits were extended to once every 6 months after 2 years in both groups. Blood tests, including liver function tests and serum α-fetoprotein (AFP) analysis, were performed at each of these visits. If LTP and/or intrahepatic distant recurrence (IDR) were detected on imaging during the follow-up period, various treatment options were recommended based on the results of a discussion among our multidisciplinary team, considering the characteristics of the recurrent tumor, patient request, liver function, and general patient condition.
To evaluate the technical success, immediate therapeutic response, and complications, all patients underwent three-phase CECT immediately after the first session of RFA. If immediate follow-up CT revealed tumoral enhancement around the RFA zone, additional RFA treatments or other treatment methods, such as TACE or surgical resection, were performed. For follow-up, all patients underwent three-phase CECT 1 month after the initial treatment, 2 months after the initial treatment for the second follow-up visit, and every 3 months thereafter in the RFA group. This study was censored on January 1, 2022.
Assessment of therapeutic outcomes
The therapeutic outcomes, including LTP, IDR, PFS, OS, major complication rates, and length of hospital stay, were compared between the two groups before and after propensity score (PS) matching. The terminology used for the description of the RFA procedure (e.g., technical success), therapeutic outcomes (e.g., LTP), and complications in our study followed the proposed guidelines.16 Additionally, the study outcome and survival analyses were based on the proposed definitions.17 LTP was defined as newly appearing tumoral enhancement in or at the margin of the ablated zone in the RFA group and in or around the necrotized HCC in the DEB-TACE group. Distant recurrence was defined as a newly appearing recurrent tumor in the untreated liver (IDR) or extrahepatic regions.18 PFS was defined as the time between initial treatment and tumor recurrence (LTP, IDR) or death. OS was defined as the time between the first treatment and either death or the last follow-up visit to the outpatient clinic before December 31, 2021.
Major complications were defined as events that occurred after the procedure that were life threatening if left untreated, that led to substantial morbidity and disability, or that increased the care level and resulted in an increased length of hospital stay.16 This included any case in which a blood transfusion or additional interventional procedure was required. All other complications were considered minor. Follow-up imaging studies and clinical medical records were examined to assess major complications such as liver abscess, active bleeding, and pleural effusion.
Statistical analysis
All statistical analyses were performed using Stata/SE software v16.1 (StataCorp, College Station, TX, USA). The patient demographics and clinical characteristics were compared between the DEB-TACE and RFA groups using the Wilcoxon rank-sum test and independent t-test for continuous variables, and Fisher’s exact test and χ2 test for categorical variables.
The cumulative LTP, IDR, PFS, and OS rates during the follow-up period were estimated using the Kaplan-Meier method, and the differences in curves between two groups were compared using a log-rank test before and after PS matching. The PS was estimated using logistic regression, and 1:1 patient matching using the nearest-neighbor matching method with a 0.05 caliper was performed. The variables used for PS matching between two groups were age, sex, body mass index, tumor size, tumor location (perivascular/non-perivascular and peripheral/central), underlying chronic liver disease (hepatitis B virus [HBV], hepatitis C virus [HCV]), Child-Pugh class, presence of portal hypertension, initial serum AFP and alanine aminotransferase (ALT) levels. Serum AFP was divided into two categories (> 100 μg/mL and ≤ 100 μg/mL) according to known predictors of post-treatment recurrence and prognosis19 because of its broad range and difficulty in matching. Perivascular HCC was defined as an index tumor with any contact with first- or second-degree branches of a portal or hepatic vein measuring ≥ 3 mm in axial diameter.20 Peripheral and central HCC were defined as HCC located < 3 cm from the liver capsule or ≥ 3 cm away from the liver capsule, respectively.21
The prognostic factors and association between treatment methods for PFS and OS before and after PS matching were assessed using Cox proportional hazard models in univariate and multivariate analyses. Any variables with a statistically significant P value < 0.05 in the log-rank test were candidates for multivariate Cox proportional hazards regression analysis. Potential prognostic factors for PFS rates included age, sex, cause of liver disease, Child-Pugh class, size of the index tumor, perivascular tumor location, initial AFP level, antiviral therapy during the follow-up period, and presence of portal hypertension. As prognostic factors for the OS rate, the location of the index tumor and the presence of LTP or IDR after RFA or DEB-TACE were considered. The results are given as the median ± standard deviation. A P value < 0.05 was considered statistically significant.
Ethics statement
This retrospective comparative study involved patients who underwent either DEB-TACE or RFA at a single tertiary care center (Chonnam National University Hwasun Hospital, Hwasun, Republic of Korea). Our Institutional Review Board (IRB) approved the study, and the need for written informed consent from the patients was waived due to the retrospective nature of the study (IRB No. CNUHH-2022-188). The study was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
RESULTS
Baseline characteristics of patients
The baseline characteristics of all study patients before PS matching are shown in Table 1. The median follow-up period was 31.8 (range: 4.9–130.2) months in the DEB-TACE group and 27.4 (range: 0.3–59.9) months in the RFA group (P = 0.796). The DEB-TACE group had older patients (P < 0.001), fewer patients with HBV (P = 0.012), more patients with HCV (P = 0.011), lower ALT levels (P = 0.011), higher Protein induced by vitamin K absence-II levels (P = 0.016), higher Modified Union for International Cancer Control stages (P < 0.001), and larger tumor sizes (P < 0.001) than the RFA group. The tumor location was not significantly different between the two groups. After PS matching, 46 patients were matched in each group, and the two groups showed no significant differences in any variables (Table 2).
Table 1
Patient demographics and clinical characteristics before propensity score matching
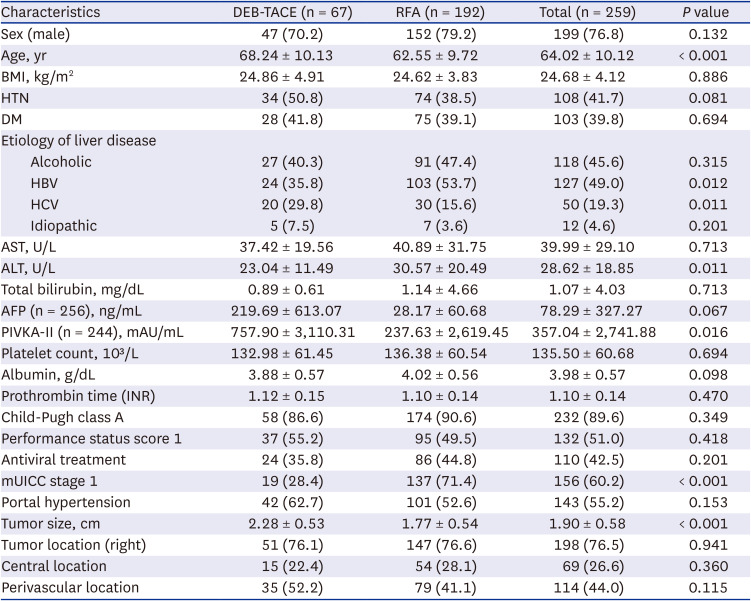
Data are reported as the number of patients with percentages in parentheses or mean ± standard deviation.
DEB-TACE = drug-eluting bead transarterial chemoembolization, RFA = radiofrequency ablation, BMI = body mass index, HTN = hypertension, DM = diabetes mellitus, HBV = hepatitis B virus, HCV = hepatitis C virus, AST = aspartate aminotransferase, ALT = alanine aminotransferase, AFP = α-fetoprotein, PIVKA-II = protein induced by vitamin K absence-II, INR = international normalized ratio, mUICC = Modified Union for International Cancer Control.
Table 2
Patient demographics and clinical characteristics after propensity score matching
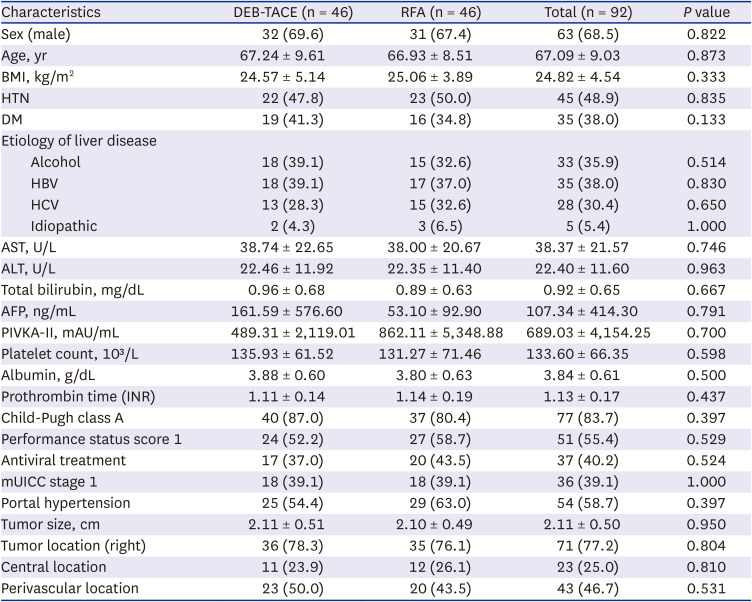
Data are reported as the number of patients with percentages in parentheses or mean ± standard deviation.
DEB-TACE = drug-eluting bead transarterial chemoembolization, RFA = radiofrequency ablation, BMI = body mass index, HTN = hypertension, DM = diabetes mellitus, HBV = hepatitis B virus, HCV = hepatitis C virus, AST = aspartate aminotransferase, ALT = alanine aminotransferase, AFP = α-fetoprotein, PIVKA-II = protein induced by vitamin K absence-II, INR = international normalized ratio, mUICC = Modified Union for International Cancer Control.
Comparison of therapeutic outcomes
Cumulative recurrence, survival rate and associated factors with multivariate analysis
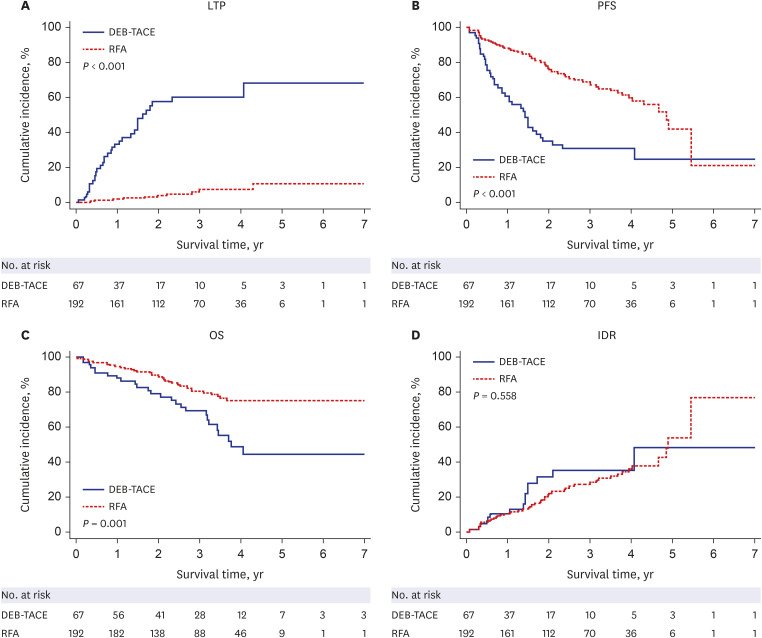
The comparison between the DEB-TACE and RFA groups before PS matching showed a significant difference in the cumulative intrahepatic LTP (P < 0.001), PFS (P < 0.001), and OS (P = 0.001) rates (Fig. 2).
Fig. 2
LTP, PFS, and OS rates between the DEB-TACE and RFA groups in all 259 patients before propensity score matching. The (A) cumulative LTP, (B) PFS, and (C) OS rates were significantly better in the RFA group than in the DEB-TACE group. The (D) IDR rates showed no significant difference between the two groups.
DEB-TACE = drug-eluting bead transarterial chemoembolization, RFA = radiofrequency ablation, LTP = local tumor progression, PFS = progression-free survival, OS = overall survival, IDR = intrahepatic distant recurrence.
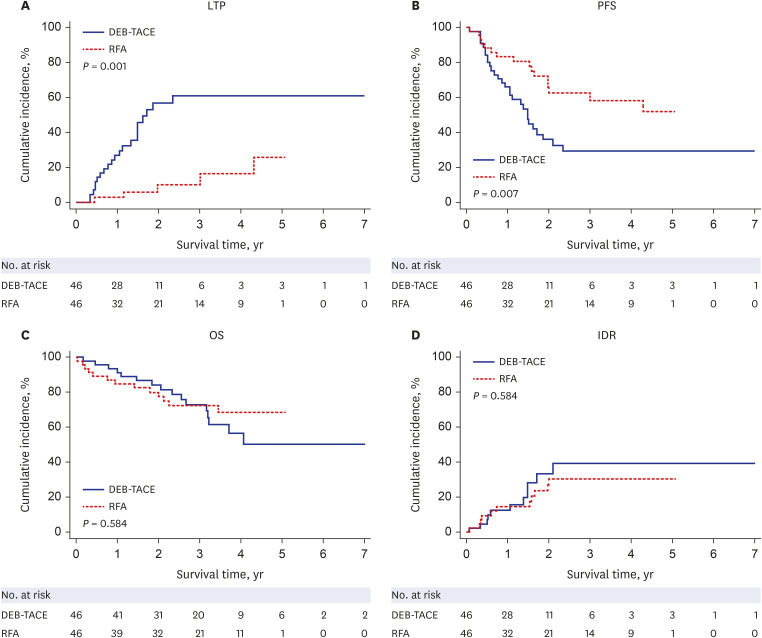
After PS matching, the cumulative 1-, 2-, 3-, and 5-year LTP rates in the RFA group were lower than those in the DEB-TACE group (2.7%, 9.8%, 16.3%, and 25.6%, respectively, in the RFA group, and 26.7%, 56.6%, 60.9%, and 60.9%, respectively, in the DEB-TACE group; P < 0.001 by log-rank test) (Fig. 3A). The 1-, 2-, 3-, and 5-year PFS rates in the RFA group were higher than those in the DEB-TACE group (83.3%, 62.7%, 58.2%, and 51.8%, respectively, in the RFA group, and 66.1%, 62.7%, 29.3%, and 29.3%, respectively, in the DEB-TACE group; P = 0.007 by log-rank test) (Fig. 3B). Additionally, there was no significant difference in the 1-, 2-, 3-, and 5-year cumulative OS (84.8%, 77.5%, 72.4%, and 68.4%, respectively, in the RFA group, and 91.2%, 84.1%, 72.9%, and 50.2%, respectively, in the DEB-TACE group; P = 0.584 by log-rank test) and IDR (14.4%, 30.3%, 30.3%, and 30.3%, respectively, in the RFA group, and 12.2%, 33.2%, 39.3%, and 39.3%, respectively, in the DEB-TACE group; P = 0.554 by log-rank test) between the two groups (Fig. 3C and D).
Fig. 3
LTP, PFS, and OS rates between the DEB-TACE and RFA groups in all 92 patients after propensity score matching. The (A) cumulative LTP and (B) PFS rates were significantly better in the RFA group than in the DEB-TACE group. The (C) OS and (D) IDR rates were not significantly different between the two groups.
DEB-TACE = drug-eluting bead transarterial chemoembolization, RFA = radiofrequency ablation, LTP = local tumor progression, PFS = progression-free survival, OS = overall survival, IDR = intrahepatic distant recurrence.
Among all variables, univariate analysis of all study patients (n = 92) showed that treatment type (hazard ratio [HR], 0.44; 95% confidence interval [CI], 0.23–0.81; P = 0.009) was a significant risk factor for poor PFS (Table 3). Additionally, a lower albumin level (P = 0.003) and Child-Pugh class B disease (P = 0.018) were significant factors associated with poor OS. The results of multivariate analysis showed that a lower serum albumin level was the sole significant factor for poor OS (HR, 0.37; 95% CI, 0.16–0.85; P = 0.019). Treatment type was not a statistically significant risk factor for cumulative OS in univariate and multivariate analyses, with a HR of 0.81 (95% CI, 0.39–1.70; P = 0.584) and 0.65 (95% CI, 0.30–1.42; P = 0.281), respectively (Table 3).
Table 3
Univariate and multivariate analyses for PFS and OS for all 92 patients
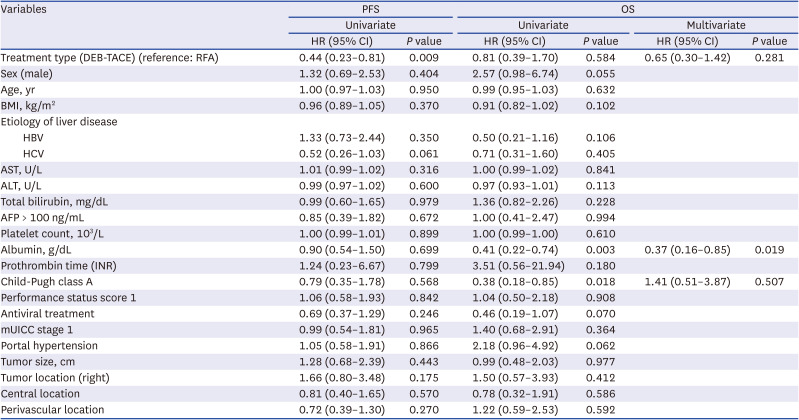
The results of univariate analysis of all included patients (n = 92) showed that the treatment type (HR, 0.44; 95% CI, 0.23–0.81; P = 0.009) was a significant risk factor for poor PFS. Furthermore, a lower albumin level (P = 0.003) and Child-Pugh class B disease (P = 0.018) were significant factors associated with poor OS in univariate analysis. The results of multivariate analysis showed that a lower serum albumin level was the sole significant factor for poor OS (HR, 0.37; 95% CI, 0.16–0.85; P = 0.019). Treatment type was not a statistically significant risk factor for cumulative OS in univariate and multivariate analyses, with a HR of 0.81 (95% CI, 0.39–1.70; P = 0.584) and 0.65 (95% CI, 0.30–1.42; P = 0.281), respectively.
PFS = progression-free survival, OS = overall survival, HR = hazard ratio, CI = confidence interval, DEB-TACE = drug-eluting bead transarterial chemoembolization, RFA = radiofrequency ablation, BMI = body mass index, HBV = hepatitis B virus, HCV = hepatitis C virus, AST = aspartate aminotransferase, ALT = alanine aminotransferase, AFP = α-fetoprotein, INR = international normalized ratio, mUICC = Modified Union for International Cancer Control.
Complications after each treatment
Regarding complications, there was no significant difference in major complication rates between the DEB-TACE group (1 of 46 patients, 2.2%) and RFA group (2 of 46 patients, 4.3%) (P = 1.000) (Table 4). One patient in the DEB-TACE group (2.2%) experienced pleural effusion, which was treated with percutaneous catheter drainage, and two patients in the RFA group (4.3%) experienced hemoperitoneum with evidence of active bleeding, which was managed with transarterial embolization in both patients. Additionally, there was no evidence of treatment-related seeding after RFA, and no deaths were considered to be related to treatment with RFA or DEB-TACE. The median length of hospital stay was longer in the RFA group (4.93 ± 2.32 days) than that in the DEB-TACE group (3.85 ± 3.46 days) (P = 0.001).

Recurrence and post-procedural treatment
Recurrence occurred in 29 of 46 patients in the DEB-TACE group and 16 of 46 patients in the RFA group. In the DEB-TACE group, 18 patients were treated with cTACE, five with cTACE and RFA, and two with cTACE and radiation therapy. Moreover, one patient was treated with RFA; one with cTACE and sorafenib; one with cTACE, radiation therapy, and sorafenib; and one with sorafenib.
In the RFA group, four patients were treated with cTACE and six with RFA. One patient received cTACE and RFA, one received cTACE and radiation therapy, and one received TARE and radiation therapy. Three patients had no medical record of further treatment. One patient was confirmed death 17 months after recurrence without treatment due to follow-up loss, one patient died at our hospital 1 month after recurrence, and another patient was transferred to another hospital because of the patient’s preference.
DISCUSSION
Our results revealed that the PFS and LTP rates were significantly better in the RFA group, which may be due to differences in the mechanism of each treatment. RFA can produce a safety margin of up to 0.5 cm, which can limit the local recurrence rate by ablating possible microsatellite lesions and preventing microscopic invasion of HCC cells in the portal vein22; in contrast, DEB-TACE involves the use of small microspheres (75–150 μm) that penetrate into the vascular network of the tumor and induce cytotoxic and ischemic effects, leading to tumor necrosis and intense inflammatory and fibrotic reactions in the tissue surrounding the tumor.23 However, despite treatment success, DEB-TACE is unable to produce a safety margin due to the lack of portal vein embolization and the possibility of residual daughter nodules, which may lead to local tumor recurrence.2425 Kim et al.13 reported that the DEB-TACE and RFA groups had similar PFS, LTP, IDR, and tumor response rates for patients with single small (≤ 3 cm) HCC. The different PFS results compared to those reported in the present study may be explained by the inclusion of more patients with Child-Pugh class A liver function in the present study, resulting in a better prognosis with RFA.
In this study, the long-term OS was not statistically significantly different between the RFA and DEB-TACE groups, which may be because additional treatments such as TACE were actively performed for recurrent HCC in both treatment groups. Although several previous studies have compared the long-term survival and treatment responses of cTACE and RFA as first-line treatments in patients with single HCC measuring ≤ 3 cm,91011 little is known about the survival benefit of DEB-TACE in patients with single small HCC as an initial treatment compared to RFA. Hsu et al.12 compared the OS among patients with HCC treated with cTACE or RFA as an initial treatment and reported that the RFA group had a significantly better long-term OS than the cTACE group before PS matching, but that there was no significant difference in long-term OS after PS matching. Other studies have reported that cTACE could provide similar OS and PFS rates compared to RFA in patients with single small (≤ 3 cm, ≤ 2 cm, and 2–3 cm) HCC.91011 Although the findings of these previous studies were similar to the OS findings in this study, the previous studies were limited to cTACE.
The majority of earlier studies and meta-analyses comparing cTACE and DEB-TACE reported better procedural safety with fewer side effects and a lower incidence of liver and systemic toxicity with DEB-TACE than with cTACE.26 However, the clinical outcome findings remain controversial between studies. Some studies reported no significant differences in the tumor response rate between the two treatments,2728 while others found greater OS rates and tumor response in patients treated with DEB-TACE than in those treated with cTACE.2930 Additionally, it is difficult to compare the clinical results because most patients were converted to other treatments during the follow-up period when local tumor recurrence was observed.
The multivariate analysis in the present study showed that a lower serum albumin level was a significant predictive factor for poor OS, which is well correlated with the findings of a previous study of prognostic indicators in cirrhotic patients showing that serum albumin was a significant prognostic variable for survival.31 Indeed, albumin is influenced by hepatic synthetic function and transvascular escape of clearance favored by sepsis and ascites.32
Both treatment groups had low rates of major complications (4.3% in the RFA group and 2.2% in the DEB-TACE group) with no significant difference (P = 1.000), which is in accordance with previous studies reporting major complication rates ranging from 0.4% to 5.7%.113334 Most complications following these procedures could be successfully managed with endovascular or percutaneous interventional therapies.
This study has several limitations. First, this was a retrospective study with a relatively small cohort, although PS matching analysis was performed to decrease the bias. Therefore, larger prospective randomized studies are needed to confirm our results. Second, as this was a single-center study, the results may not be generalizable. Indeed, the applicability of our findings to patients with HCC at other centers may be limited due to detailed differences in treatment protocols and strategies. Third, although long-term OS was assessed, the median follow-up duration was only 31.8 and 27.4 months in the DEB-TACE and RFA groups, respectively, representing a relatively short follow-up period.
The present study is the first to directly compare the long-term OS, PFS, and LTP rates of DEB-TACE versus RFA in patients with a single small (≤ 3 cm) HCC. Selection bias was minimized using PS matching to maintain the homogeneity of the patient selection criteria between the two groups and to avoid related confounding variables that may exist between the groups in observational studies.
In conclusion, the present study demonstrated that the LTP and PFS rates of RFA were superior to those of DEB-TACE as a first-line treatment for single HCC measuring ≤ 3 cm after PS matching. However, DEB-TACE can be as useful as RFA for treating a single small HCC in terms of OS, with a shorter length of hospital stay. RFA is still recommended as a first-line treatment for single small HCC; however, DEB-TACE may be considered as an efficient substitute for RFA in some patients who are ineligible for RFA because of an unfavorably located tumor.
 XML Download
XML Download