

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Chronic obstructive pulmonary disease (COPD) is a major cause of morbidity and mortality worldwide and the 3rd leading cause of death resulting in more than 3 million deaths per year.12 COPD is associated with several comorbidities including ischemic heart disease (IHD), a common comorbidity of COPD and an important contributor to mortality in COPD, especially in subjects with mild-to-moderate severity.3456 In addition, COPD is prevalent in patients with cardiovascular disease (CVD),7 and the relationship between these two diseases is important. Accordingly, mitigating the risk of IHD in subjects with COPD is crucial to alleviate COPD-related burdens and improve the treatment outcome of COPD.
In previous epidemiologic studies, including systemic review articles, subjects with COPD were shown to have a higher risk of CVD, including IHD, than individuals without COPD.891011121314 However, most studies were cross-sectional in design, overlooking the temporal association between them.9 Although two longitudinal studies have examined the association of COPD with comorbidities, neither study had a control group.1516 Consequently, although many studies on related subjects have been performed, the longitudinal evidence regarding this topic remains insufficient.
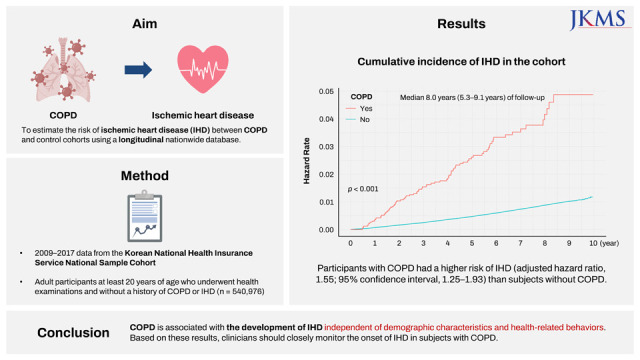
Therefore, we aimed to estimate the incidence rate of IHD and to compare the risk of IHD between subjects with and without COPD using a nationally representative database.
METHODS
Data source and study setting
We used data from the Korean National Health Insurance Service National Sample Cohort (NHIS-NSC), a population-based longitudinal cohort study composed of approximately 2.2% of representative Korean citizens.17 The NHIS is a universal health insurance provider managed by the government, covering 97% of the Korean population. The NHIS dataset includes information on demographic variables (e.g., age, sex, income status, residential area), healthcare utilization, health screening examination, disease diagnosis under International Classification of Diseases, 10th Revision (ICD-10) codes, drug prescription, and death. All Korean employees receive biannual health screening examinations. Regardless of employment, all Koreans ≥ 40 years of age also receive biannual health screening examinations.
The NHIS database linking claims data and health examination data, including a variety of medical and health information, has been widely used in various studies.18
Study population
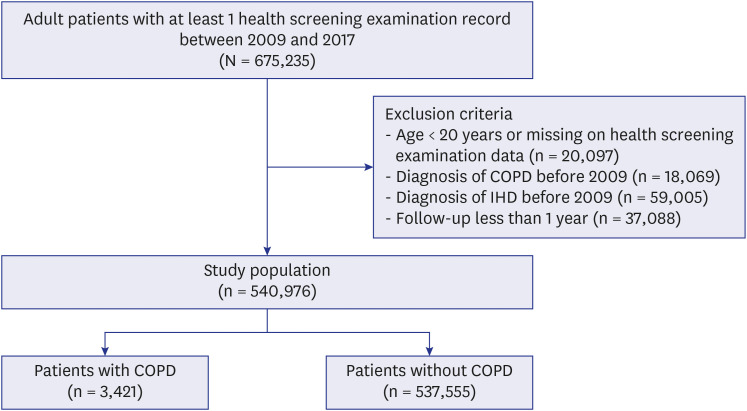
There were 675,235 participants who underwent at least one health screening examination between 2009 and 2017. Among the participants, subjects < 20 years of age or those with missing data on health screening examination (n = 20,097), diagnosis of COPD before 2009 (n = 18,069), diagnosis of IHD before 2009 (n = 59,005), and subjects who were followed up < 1 year (n = 37,088) were excluded. Finally, 540,976 participants were included in this study. Among the study subjects, 3,241 were newly diagnosed with COPD and 537,555 were not diagnosed with COPD (Fig. 1).
Exposure
The main exposure was COPD defined as ICD-10 diagnosis codes of J431, J432, J438, J439, or J44 with COPD medication prescribed at least twice. COPD medications included long-acting muscarinic antagonist (LAMA), long-acting beta-2 agonist (LABA), inhaled corticosteroids (ICS) plus LABA (ICS+LABA), LABA plus LAMA (LABA+LAMA), ICS plus LABA plus LAMA (ICS+LABA+LAMA), short-active muscarinic antagonists, short-acting beta-2 agonist, phosphodiesterase-4 inhibitor, systemic bronchodilators, or theophylline.
Outcomes
The primary outcome was the comparison of the incidence and risk of IHD between the COPD and matched cohorts. IHD was defined as claims under the ICD-10 diagnosis codes I20–I25 and concomitant hospitalization history. The study population was followed until the date of the first occurrence of an IHD event, death, or December 31, 2019, whichever came first. Among patients with COPD, we only considered there is a causal inference between COPD and IHD when IHD occurs at least one year after COPD diagnosis.
Covariates
Data for basic demographic characteristics of age, sex, income status, and residential area were collected from the dataset. Income status was divided into the highest 20% (high), the lowest 20% (low), and the rest (middle); individuals supported by the medical aid program were classified as the low-income group. The residential area was classified into metropolitan cities, middle- and small-sized cities, and rural areas.
Health-related behaviors, such as smoking status (never, ex-smoker, and current smoker), alcohol consumption (none, 1–2 times a week, 3–4 times a week, and almost every day), and physical activity were determined based on a self-reported questionnaire. Regular physical activity was defined as follows: 1) ≥ 30 minutes of walking at least 5 times per week, 2) ≥ 30 minutes of moderate physical activity at least 5 times per week, or 3) ≥ 20 minutes of vigorous physical activity at least 3 times per week. Body mass index (BMI) was calculated as body weight divided by the square of height (kg/m2) and classified into four groups as follows: low (< 18.5 kg/m2), normal (18.5–22.9 kg/m2), overweight (23.0–24.9 kg/m2), and obese (≥ 25 kg/m2).
Comorbidities were defined using ICD-10 codes as follows: hypertension (I10–I15, except for I14), diabetes mellitus (E10–E14), dyslipidemia (E78), and chronic kidney disease (N18).
Statistical analysis
Descriptive statistics are presented as number (percentage) for categorical variables and mean ± standard deviation for continuous variables. The two groups were compared using the χ2 test for categorical variables and the t-test for continuous variables. The incidence rate of IHD was calculated by dividing the number of incident cases per 10,000 person-years. A cumulative incidence plot was used to compare the incidence of IHD between the COPD and matched cohorts, and a log-rank test was used to evaluate significant differences between the groups.
Cox proportional hazards regression analyses were used to evaluate the risk of incident IHD in the COPD cohort versus matched cohort. The multivariable analysis was fully adjusted for age, sex, BMI, smoking status, alcohol consumption, economic status, residential area, regular physical activity, and comorbidities (hypertension, diabetes mellitus, dyslipidemia, chronic kidney disease). Stratified analyses were performed based on age, sex, BMI, smoking status, and regular physical activity.
To validate the multivariable analysis, a sensitivity analysis was performed using 1:4 matching. The sensitivity analysis included 3,241 participants with COPD and 13,674 participants matched for age, sex, BMI, smoking status, alcohol consumption, income status, residential area, regular physical activity, and comorbidities (hypertension, diabetes mellitus, dyslipidemia, chronic kidney disease).
A two-sided P value < 0.05 was considered statistically significant, and all analyses were conducted using SAS 9.4 (SAS Institute Inc., Cary, NC, USA).
RESULTS
Baseline characteristics
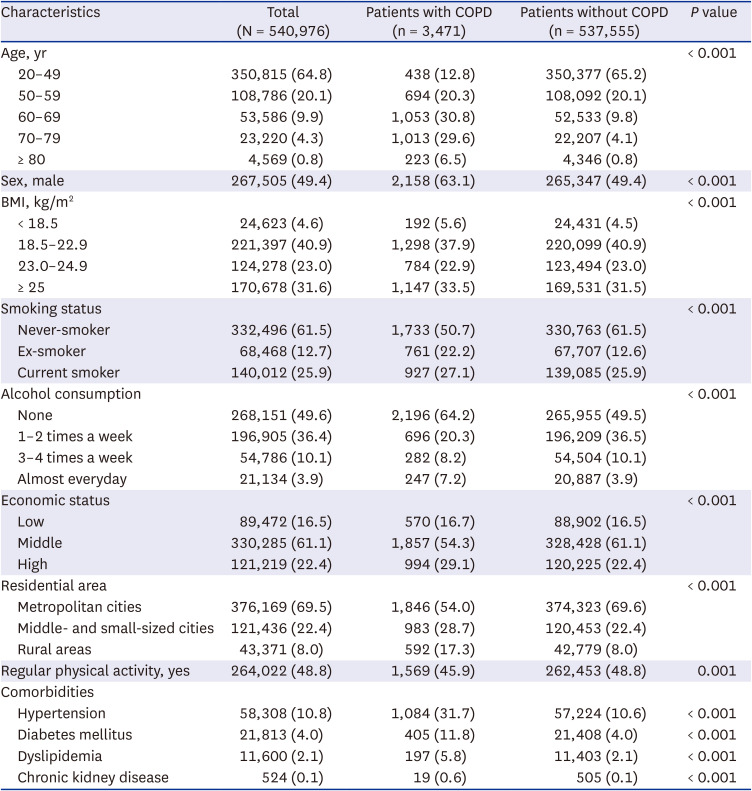
The baseline characteristics of the study participants are shown in Table 1. Participants with COPD were more likely to be older and male than were those without COPD. Participants with COPD had higher rates of ever smokers but also non-drinkers compared to those without COPD. Participants with COPD were more likely to have a higher economic status but less likely to live in metropolitan cities. The proportion of subjects who regularly performed physical activity was larger in participants without COPD than in individuals with COPD, and all comorbidities (hypertension, diabetes mellitus, dyslipidemia, chronic kidney disease) were more common in participants with COPD.
Table 1
Patient baseline characteristics
Incidence and risk of IHD
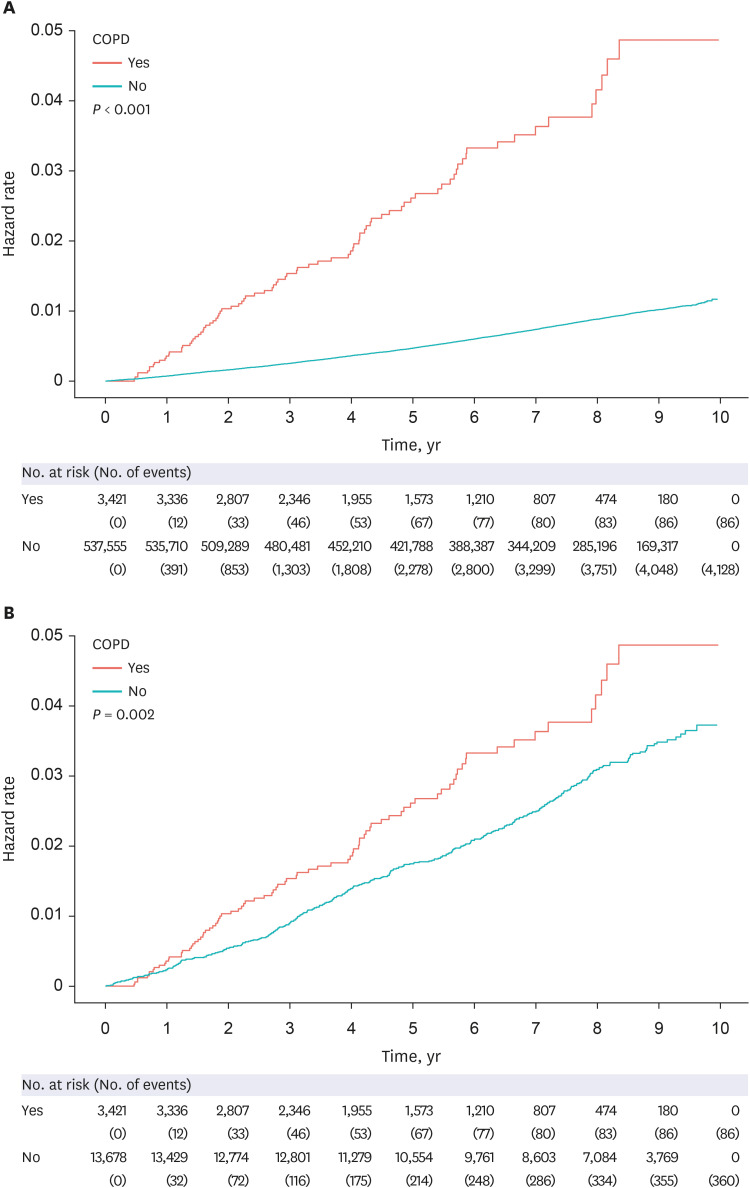
During a median of 8.0 years (5.3–9.1 years) of follow-up, 2.51% of the participants with COPD (86/3,421) and 0.77% of the patients without COPD (4,128/537,555) developed IHD, with an incidence of 52.24 and 10.91 per 10,000 person-years, respectively. Similarly, there was a significant difference in the cumulative incidence rate of IHD between patients with and without COPD (log-rank P < 0.001). As shown in Table 2, patients with COPD had a higher risk of IHD (adjusted hazard ratio [aHR], 1.55; 95% confidence interval [CI], 1.25–1.93) than subjects without COPD.
Table 2
Risk of IHD based on the presence of COPD

IHD = ischemic heart disease, COPD = chronic obstructive pulmonary disease, HR = hazard ratio, CI = confidence interval, BMI = body mass index.
aAdjusted for age, sex, BMI, smoking status, alcohol consumption, economic status, residential area, regular physical activity, and comorbidities (hypertension, diabetes mellitus, dyslipidemia, chronic kidney disease).
Sensitivity analysis using a 1:4 age- and sex-matched cohort showed the COPD cohort to have a higher risk of IHD (aHR, 1.50; 95% CI, 1.18–1.91) compared with the matched cohort (Supplementary Tables 1 and 2).
The cumulative incidence of IHD in the unmatched cohort and the 1:4 matched cohort are shown in Fig. 2.
Subgroup analysis
Stratified analyses regarding the risk of IHD among patients with COPD compared with subjects without COPD are shown in Table 3. Regardless of age, sex, BMI, smoking status, and physical activity, the COPD patients had a higher risk of IHD compared with the matched cohort (P for interaction > 0.050 for all).
Table 3
Subgroup analysis of risk factors of IHD in patients with COPD
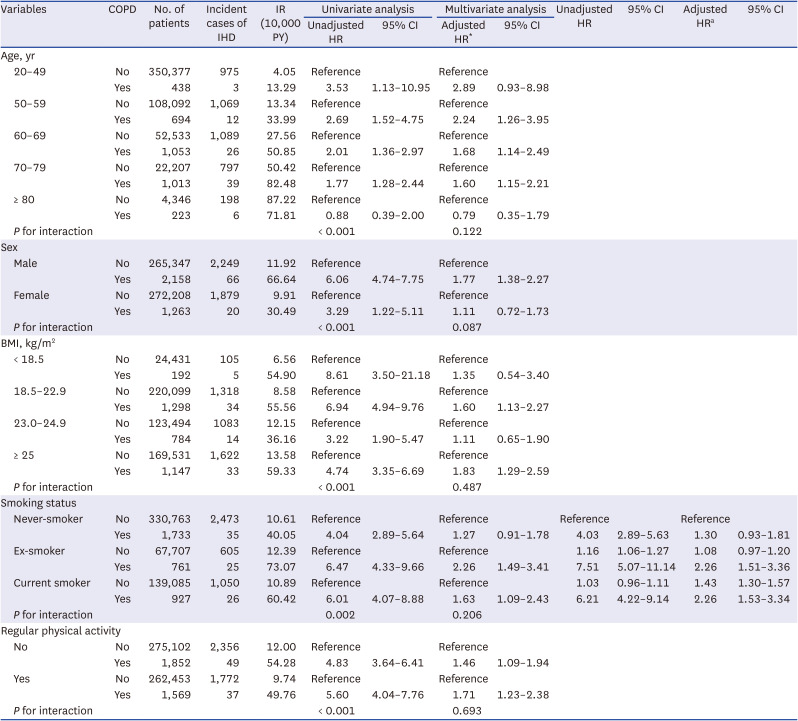
COPD = chronic obstructive pulmonary disease, IHD = ischemic heart disease, IR = incidence rate, PY = person-years, HR = hazard ratio, CI = confidence interval, BMI = body mass index.
aAdjusted for age, sex, BMI, smoking status, alcohol consumption, economic status, residential area, regular physical activity, and comorbidities (hypertension, diabetes mellitus, dyslipidemia, chronic kidney disease).
Furthermore, the risk of IHD was evaluated based on smoking status and the presence of COPD; compared with never-smokers without COPD, smokers with COPD had the highest risk of IHD (ex-smoker, aHR 2.26; 95% CI, 1.51–3.36; current smoker, aHR 2.26; 95% CI, 1.53–3.34), followed by smokers without COPD (aHR 1.43; 95% CI, 1.30–1.57). Although the risk of IHD tended to increase in never-smokers with COPD and ex-smokers without COPD (never-smoker, aHR 1.30; 95% CI, 0.93–1.81; ex-smoker without COPD, aHR 1.08; 95% CI, 0.97–1.20), the difference was not significant.
DISCUSSION
This study provides longitudinal evidence of the association between COPD and IHD using nationwide data with a median of 8.0 years of follow-up. The analyses showed that participants with COPD had an IHD incidence rate of 52.24 per 10,000 person-years, which is 1.55-fold higher compared with subjects without COPD. This relationship was consistent regardless of demographics as well as health-related behaviors, including smoking status.
Previous studies have reported an increased risk of CVD, including IHD, in patients with COPD.8910111213141516 However, most studies provided evidence based on a cross-sectional design, which is limited in providing longitudinal data.9 Although the risk of CVD was evaluated in some longitudinal studies, an objective comparison was difficult because the control group was not defined.1516 In addition, because most studies included various heart and CVDs, studies in which only the risks of IHD were investigated are scarce.12141920 Furthermore, due to the heterogeneity of study designs and outcome measures, few meta-analyses and systematic reviews have been performed on this subject89; Müllerova et al.8 reviewed 25 studies and reported the association between COPD and CVD, including IHD, heart failure, arrhythmias, stroke, arterial hypertension, and peripheral arterial disease. Based on the results, the prevalence of IHD ranged from 4.7–60% in patients with COPD; in one study from the UK, the incidence of acute myocardial infarction in patients with COPD was 6.3 per 1,000 person-years.19 In a previous review article, a relationship between IHD and COPD was found in nine studies, and the adjusted risk ratio for IHD ranged from 0.7–6.8.131419202122232425 Five of these nine studies reported a significant positive association with increased incidence of IHD in COPD patients.2021222324 Chen et al.9 updated and extended the qualitative review by Müllerova and colleagues8 and found an approximately 2.5-fold increased risk of CVD overall and a nearly 2.3-fold increased risk of IHD in patients with COPD, which is higher than our results. The discrepancy might be caused by the different study populations and designs. For example, many studies included in the previous review articles were cross-sectional in design or analyzed hospitalized patients in whom the risk of IHD is presumed to be higher. In comparison, a Danish study with 140 million person-years of population data has a similar study design to ours and reported a 1.26 aHR of myocardial infarction with lifetime association with COPD,13 which is comparable to the present study.
The major advantage of our study is the longitudinal study design using a nationwide representative database including health screening examination data that allowed analysis of information associated with income status, residential area, and health-related behavior (smoking status, alcohol consumption, and physical activity). In addition, numerous factors affecting the association between COPD and IHD were comprehensively considered in the analyses and showed that the increased risk of IHD in COPD was independent of these factors. Furthermore, the results showed a complex relationship between smoking status, COPD, and the risk of IHD. Further subgroup analysis of the study population based on smoking status and presence of COPD showed a significantly higher risk of IHD in ever-smokers with COPD compared with never-smokers without COPD, who were presumed to be the lowest-risk group for IHD.
Hypotheses have been proposed in several previous studies to explain the relationship between COPD and IHD.262728 First, the two share the same risk factors of smoking, hypertension, and age,27 indicating a strong epidemiological link between them. However, in a previous study, even after adjustments for traditional cardiovascular risk factors such as hypertension, obesity, smoking, and serum total cholesterol, patients with COPD had a 2–3-fold increase in the risk of CVD.29 In the multivariable-adjusted and stratified analyses in the present study, COPD patients had a consistently higher risk of IHD compared with patients without COPD regardless of many cardiovascular risk factors. Sharing risk factors that contribute to CVD is insufficient to explain this increased risk.
Second, COPD is not a local but a systemic inflammatory disease.26 This systemic inflammatory reaction might play a role in the increased coronary risk in patients with COPD.3031 In previous studies, inflammatory mediators such as interferon-γ, interleukin (IL)-1, tumor necrosis factor α, IL-6, and acute phase inflammatory proteins (fibrinogen, C-reactive protein, and amyloid protein) were shown to be involved in the airway as well as in systemic inflammation in COPD.323334 Because many of these inflammatory mediators are also involved in the activation of immune cells in atheromatous plaques in coronary heart disease,3536 COPD-related inflammation may trigger or enhance atherosclerosis in coronary arteries. Third, systemic oxidative stress in COPD may increase the risk of IHD. COPD is associated with enhanced local pulmonary and systemic oxidative stress,37 and oxidative stress plays a pivotal role in the pathogenesis of atherosclerosis, particularly its detrimental effects on vascular endothelial function.38 Other hypotheses suggest that factors such as impaired vasodilatory capacity39 and activation of the sympathetic nervous system4041 also contribute to IHD in patients with COPD. Because such a complex systemic response can increase the risk of IHD in COPD patients even if they do not have cardiovascular risk factors, we believe cardiovascular monitoring is important in managing COPD patients.
COPD is the 3rd leading cause of death worldwide,12 and IHD is the leading cause of death in this population.4 Thus, to improve the long-term treatment outcomes in COPD, it is important to reduce the risk of IHD and its related mortality. The results of the present study provide clinical relevance by emphasizing the importance of prevention and proper management of IHD in COPD. The highest risk of IHD in ever-smokers with COPD highlights the importance of screening modifiable risk factors (dyslipidemia, diabetes mellitus, hypertension, regular physical activity) and early diagnosis of IHD. Notably, in our study, the increased risk of IHD in never-smokers with COPD was not significantly different from that of never-smokers without COPD. However, careful interpretation of this result is necessary due to the relatively small number of IHD events and further studies are needed to investigate this issue.
Our study has some limitations. First, because this study was conducted in Korea, generalization of the results to other ethnic groups and countries may be difficult. Second, COPD and comorbidities were determined using the ICD-10 codes, diagnoses may be over- or underestimated. However, the clinical diagnosis of IHD should be accurate because IHD was defined in hospitalized cases in whom the evaluation for diagnosis was likely sufficient. Third, due to the lack of laboratory results in the NHIS claim data, the risk of IHD was not analyzed based on GOLD severity (based on forced expiratory volume in one second), COPD classification (A, B, and C), or other phenotypes of COPD (e.g., emphysema, chronic bronchitis, eosinophilic COPD). Future large-scale studies on these associations are needed. Lastly, the proportion of smokers in the COPD group in our study was relatively low. Although the reasons for this phenomenon cannot be fully explainable, we carefully suggest the lower participation rate in health screening examinations in smokers compared to never-smokers might be an explanation. Previous studies evaluating COPD patients using the health screening data of the NHIS-NSC dataset also showed a relatively low smoking rate and a low proportion of males among COPD patients.4243
In conclusion, the data from a nationwide longitudinal database showed a higher risk of IHD in patients with COPD than in subjects without COPD regardless of demographic characteristics and health-related behaviors. We suggest that clinicians should closely monitor for the onset of IHD in COPD patients.
 XML Download
XML Download