

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Pneumonia is the deadliest infectious disease and was ranked fourth globally among all causes of death in 2019.1
Streptococcus pneumoniae, or pneumococcus, is the most common causative agent of community-acquired pneumonia (CAP), accounting for 24–31% of cases.2 Pneumococcus is a gram-positive diplococcus that can cause mucosal (otitis media, sinusitis, and pneumonia) and invasive diseases (bacteremia, meningitis, and empyema). The capsular polysaccharide (CPS), a major virulence factor, can inhibit phagocytosis of pneumococci by host phagocytic cells with CPS-dependent immune evasion and trigger pneumococcal colonization of the nasopharynx, resulting in pneumococcal disease.34 To date, more than 100 capsular serotypes have been identified based on antigenic differences in CPS.5 Commercial serotype-specific pneumococcal vaccines have been developed based on the structure of the CPS.
In South Korea, the 23-valent pneumococcal polysaccharide vaccine (PPSV23) was introduced in 2000 and incorporated into the national immunization program (NIP) for adults aged ≥ 65 years in May 2013. Pneumococcal conjugated vaccines (PCVs) have not yet been included in the NIP for older adults but has been recommended by the Korean Society of Infectious Diseases as part of a sequential administration of 13-valent PCV (PCV13) and PPSV23 since 2019. The PPSV23 coverage rate in older adults reached 66.4% in 2014 and remains at over 60% to date.6 In the pediatric NIP, children aged < 24 months were first vaccinated with PCV7 in 2003 and later with 10-valent PCV (PCV10)/PCV13 by May 2014. By 2015, ≤ 98% of children aged < 24 months were vaccinated with PCV10/PCV13.7
Both direct and indirect herd effects of pneumococcal vaccination can affect serotype replacement in older adults.8910 Owing to immune pressure from pneumococcal vaccines, the incidence of non-vaccine serotype (NVT) pneumococcal diseases has gradually increased worldwide.1011121314 A recent study in Israel showed that NVT invasive pneumococcal disease (IPD) rates increased by 93% in the late PCV13 vaccination period compared to the early PCV vaccination period.15 However, IPD and pneumococcal pneumonia caused by some vaccine serotypes (VTs), such as serotypes 3 and 19A, remain problematic in older adults.91013151617181920
Serotype distribution may vary geographically and is influenced by many factors, including antibiotic use and pneumococcal vaccination status.21 Data on serotype distribution and clinical outcomes are important for introducing a novel extended-valent pneumococcal vaccine into the NIP. Thus, we aimed to evaluate the serotype distribution of pneumococcal CAP (pCAP) following the introduction of PCV13 and according to pneumococcal vaccination status. Based on its prevalence in adults with pCAP in our study, we analyzed the clinical characteristics associated with serotype 3 pCAP.
METHODS
Study design, participants, and definitions
This multicenter prospective hospital-based cohort study included adults (aged ≥ 19 years) with CAP hospitalized at five university hospitals in South Korea (Korea University Guro Hospital, Korea University Anam Hospital, Korea University Ansan Hospital, Hallym University Kangnam Sacred Heart Hospital, and Gyeongsang University Hospital) between September 2018 and July 2021. Pneumonia was defined as acute pulmonary infiltration in chest radiography with relevant new-onset symptoms (fever, cough, or sputum). CAP was defined as pneumonia that occurred within 48 h of admission with infection occurring outside a hospital. Two infectious disease specialists at each hospital independently screened hospitalized patients from emergency room and out-patient clinic daily, cross-checked whether they met the diagnostic criteria for CAP, and determined the causative agents of CAP. We excluded patients transferred from other hospitals, or diagnosed with hospital-acquired pneumonia or ventilator-associated pneumonia. All patients underwent clinical assessments and were treated by their attending physicians.
Pneumococcal pneumonia was diagnosed by the following criteria: 1) S. pneumoniae was isolated from clinical cultures (blood, pleural fluid, or adequate lower respiratory specimen) conducted at the time of diagnosis, and 2) positive BinaxNOW® S. pneumoniae urinary antigen assay, excluding bacterial pathogens other than pneumococcus. Patients diagnosed with pneumococcal pneumonia underwent additional serotyping tests using pneumococcal isolates. Lower respiratory specimens included sputum cultures with high-quality Gram staining (> 25 white blood cells and < 10 squamous epithelial cells/low-power field), transtracheal aspirates, endotracheal aspirates, and bronchial washing samples. The predominant microorganism from semi-quantitative culture with moderate to heavy growth was considered to a causative agent of CAP.
Data collection
For each patient, we collected demographic information, comorbidities, history of pneumococcal vaccinations (PCV13 and PPSV23), clinical culture results (blood, pleural fluid, and lower respiratory specimen), laboratory test results (BinaxNOW® S. pneumoniae urinary antigen assay, respiratory viral polymerase chain reaction [PCR, Anyplex®; Seegene, Seoul, Korea], pneumonia bacterial PCR [Seeplex®, Seegene], and serologic tests for Mycoplasma pneumoniae) and clinical outcome (30-day all-cause mortality).
Comorbidities were classified as “high-risk,” “at-risk,” and “low-risk.” “High-risk” comorbidities included human immunodeficiency virus infection, solid organ/hematopoietic stem cell transplantation, solid/hematologic cancer, functional/anatomical asplenia, chronic kidney disease, or use of immunosuppressive agents (Supplementary Data 1). “At-risk” included chronic lung disease, congestive heart failure, chronic liver disease, neurologic disease, or diabetes mellitus and excluded “high-risk” conditions. The patients without medical comorbidities were defined as “low-risk.”
Pneumococcal serotyping
Serotyping of pneumococcus was conducted for all available S. pneumoniae isolates using a multi-bead assay with monoclonal antibodies specific for 27 different serotypes (1, 2, 3, 4, 5, 6A, 6 B, 6C, 6D, 7F, 8, 9 N, 9 V, 10A, 11A, 11E, 12F, 14, 15 B, 17F, 18C, 19A, 19F, 20, 22F, 23F, and 33F). We also conducted multiplex serotyping PCR for another 15 serotypes (7C, 10F/C, 12F, 12A, 15A, 16F, 23A, 23B, 24A/F, 29, 31, 34, 35B, 35F, and 45). The details of serotyping were presented in Supplementary Data 1.
Statistical analysis
Statistical analyses were conducted using SPSS version 20 (IBM SPSS, Armonk, NY, USA). To compare differences between groups, a χ2 test or Fisher's exact test was used for categorical variables, while Student’s t-test or a one-way analysis of variance was used for continuous variables. Binary logistic regression analyses were used to identify the risk factors of mortality in hospitalized patients with pCAP, as measured by the odds ratio (OR) with 95% confidence intervals (CIs). All significant variables (P < 0.05) in univariate analysis and clinically relevant variables (age, sex, and PPSV23 vaccination) were included in the multivariate analysis. Statistical significance was set at P < 0.05.
Ethics statement
This study was approved and informed consent was waived by the Institutional Review Boards of each hospitals (Korea University Guro Hospital [2018GR0296], Korea University Anam Hospital [2018AN0312], Korea University Ansan Hospital [2018AS0206], Hanllym University Kangnam Sacred Heart Hospital [2018-07-026], and Gyeongsang University Hospital [2018-07-011-002]). The study protocols conformed with the Declaration of Helsinki and good clinical practice guidelines.
RESULTS
Study participants
A total of 5,009 hospitalized patients with CAP were included in this study: 1,404 at Korea University Guro Hospital, 817 at Korea University Anam Hospital, 847 at Korea University Ansan Hospital, 869 at Hanlym University Kangnam Sacred Heart Hospital, and 1,072 at Gyeongsang University Hospital. The mean age of the study population was 70.3 ± 16.0 years and males comprised 63.1% of the population (Table 1). The proportion of patients with at least one comorbidity was 71.3%. PPSV23 and PCV13 vaccinations were administered to 44.4% and 7.7% of patients, respectively.
Table 1
Demographics, comorbidities, and mortality rates of hospitalized patients with CAP
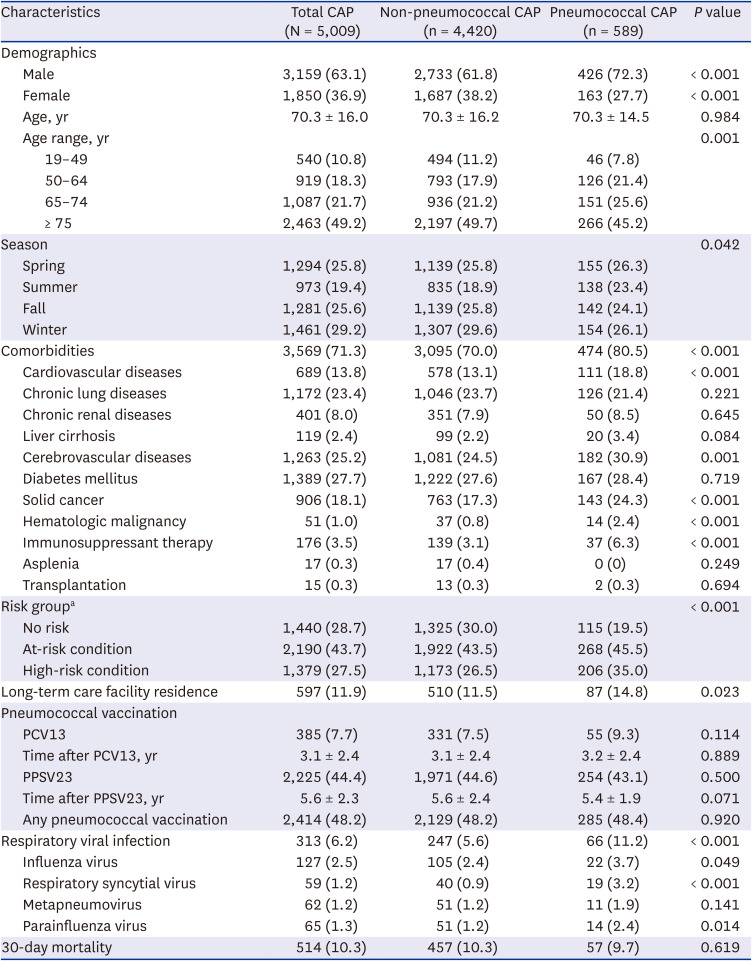
Data are shown as mean ± standard deviation or number (%).
P values were derived from the comparison of non-pneumococcal CAP and pneumococcal CAP.
CAP = community-acquired pneumonia, PCV13 = 13-valent pneumococcal conjugated vaccine, PPSV23 = 23-valent pneumococcal polysaccharide vaccine;
aNo risk: without any comorbidity; at-risk condition: presence of chronic lung disease, congestive heart failure, chronic liver disease, neurologic disease, or diabetes mellitus without any “high-risk” condition; high-risk condition: presence of human immunodeficiency virus infection, solid organ/hematopoietic stem cell transplantation, solid/hematologic cancer, functional/anatomical asplenia, chronic kidney disease, or use of immunosuppressive agents.
Microbiological distribution of CAP
Sputum and blood cultures were conducted in all hospital cohorts. S. pneumoniae urinary antigen assays and respiratory viral PCR were performed in 2,624 (52.4%) and 1,763 (35.2%) patients, respectively. Either a serological or PCR test for M. pneumoniae was conducted in 3,009 (60.1%) patients. Causative agents were identified in 41.3% of patients (n = 2,068; Supplementary Table 1). Among the causative agents identified cases, the proportion of gram-negative bacterial infections was higher than that of gram-positive bacterial infections (59.9% vs. 40.1%). S. pneumoniae (28.5%) was the most common causative agent of CAP, followed by Klebsiella pneumoniae (14.9%), Pseudomonas aeruginosa (14.4%), M. pneumoniae (11.8%), and Staphylococcus aureus (10.4%).
Comparison of pneumococcal and non-pneumococcal CAP
Of 5,009 patients with CAP, 11.8% (n = 589) had pCAP (Table 1). The diagnostic methods for pneumococcal pneumonia are shown in Supplementary Fig. 1. Compared to non-pCAP, the proportion of pCAP was significantly higher in patients that were male (61.8% vs. 72.3%, P < 0.001), with comorbidities (70.0% vs. 80.5%, P < 0.001), long-term care facility residence (11.5% vs. 14.8%, P = 0.023), and concomitant respiratory viral infection (5.6% vs. 11.2%, P < 0.001) (Table 1). The rates of pneumococcal vaccination and mortality were indistinguishable between the two groups. When stratified by age and comorbidities, the PCV13 uptake rate did not differ among the four subgroups (Table 2), while the PPSV23 uptake rate was higher in the ≥65 year-age group than in the < 65 year-age group (61.7% vs. 2.4%). The group aged <65 years with comorbidities showed low vaccine uptake rate (10.4%) and the highest rate of pCAP (17.7%) among the four subgroups. Mortality rates were highest in the group of ≥ 65 years of age with comorbidities (13.7%) and lowest in the group of < 65 years of age without comorbidities (1.8%).
Table 2
Comparison of clinical characteristics, pneumococcal vaccination status, and incidence of pneumococcal CAP by age and comorbidities
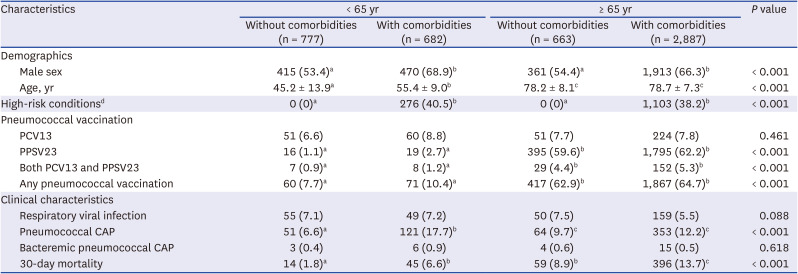
Data are shown as mean ± standard deviation or number (%).
CAP = community-acquired pneumonia, PCV13 = 13-valent pneumococcal conjugated vaccine, PPSV23 = 23-valent pneumococcal polysaccharide vaccine.
a,b,cThe values with different superscript letters (e,g. a–b, b–c, a–c) in a column mean statistically significant difference (P < 0.05), while those with same superscript letters (e,g. a–a, b–b, c–c) in a column mean statistical insignificance (P > 0.05).
dHigh-risk condition: presence of human immunodeficiency virus infection, solid organ/hematopoietic stem cell transplantation, solid/hematological cancer, functional/anatomical asplenia, chronic kidney disease, or use of immunosuppressive agents.
Serotype distribution of pCAP
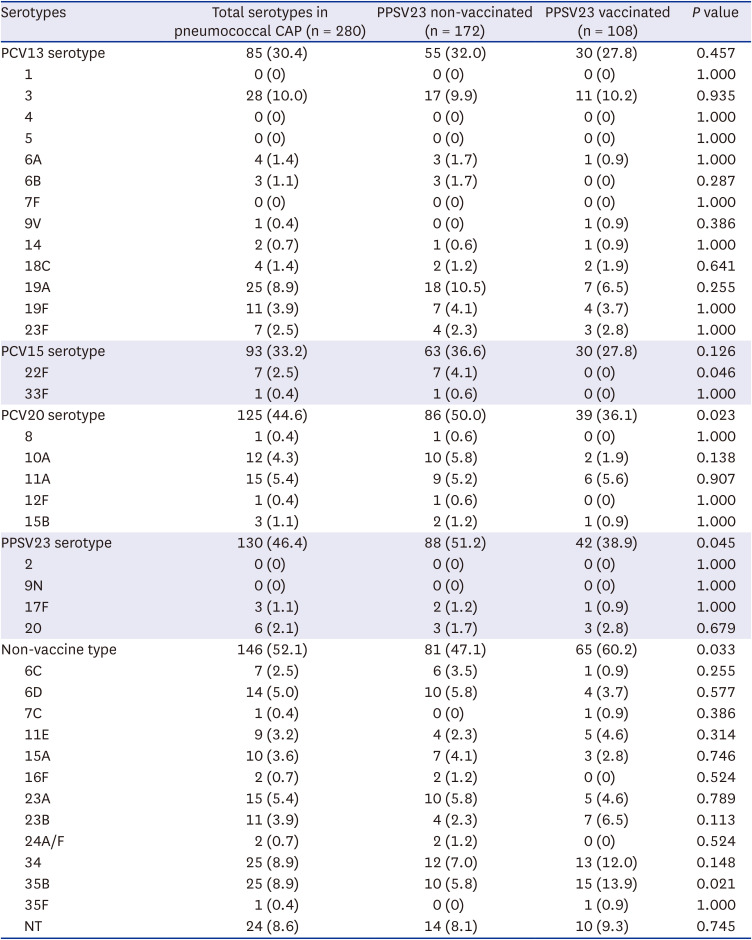
Of the 589 pCAP cases, pneumococcus was recovered by sputum or blood culture in 422 cases, and pneumococcus serotypes were identified in 280 cases (280/422, 66.4%). Among the serotype identified cases (n = 280), serotype 3 (10%) was the most common, followed by serotypes 19A (8.9%), 34 (8.9%), 35 B (8.9%), and nontypeable (8.6%) (Fig. 1A). The prevalence rates of PCV13, PCV15, PCV20, PPSV23, and NVT were 30.4%, 33.2%, 44.6%, 46.4%, and 52.1%, respectively (Table 3). We evaluated the serotype distribution according to PPSV23 vaccination status (172 cases in PPSV23-non-vaccinated group and 108 cases in PPSV23-vaccinated group). We found that the proportions of the PCV20 and PPSV23 serotypes were significantly higher in the PPSV23-non-vaccinated group than in the vaccinated group (50.0% vs. 36.1%, P = 0.023, and 51.2% vs. 38.9%, P = 0.045, respectively), whereas the proportions of the PCV13 and PCV15 serotypes did not differ between the groups. The proportion of NVTs was significantly higher in the PPSV23-vaccinated group than in the non-vaccinated group (60.2% vs. 47.1%, P = 0.033). In particular, the proportions of serotype 22F and 35 B were significantly higher in the PPSV23-non-vaccinated group and PPSV23-vaccinated group, respectively (Table 3). The most prevalent serotype in the PPSV23-vaccinated group was 35 B (13.9%), followed by 34 (12.0%), 3 (10.2%), nontypeable (9.3%), 19A (6.5%), and 24 B (6.5%) (Fig. 1C). The most prevalent serotype in the PPSV23-non-vaccinated group was 19A (10.5%), followed by serotypes 3 (9.9%), nontypeable (8.1%), and 34 (7.0%) (Fig. 1B).
Fig. 1
Serotype distribution of pneumococcal community-acquired pneumonia in South Korea from 2018 to 2021. (A) Serotype distribution of overall pneumococci. (B) Serotype distribution of pneumococci in PPSV23-non-vaccinated in individuals (C) Serotype distribution of pneumococci in PPSV23-vaccinated in individuals.
PPSV23 = 23-valent pneumococcal polysaccharide vaccine, PCV13 = 13-valent pneumococcal conjugated vaccine, PCV15 = 15-valent pneumococcal conjugated vaccine, PCV20 = 20-valent pneumococcal conjugated vaccine, NT = nontypeable, VT = vaccine serotype, NVT = non-vaccine serotype.
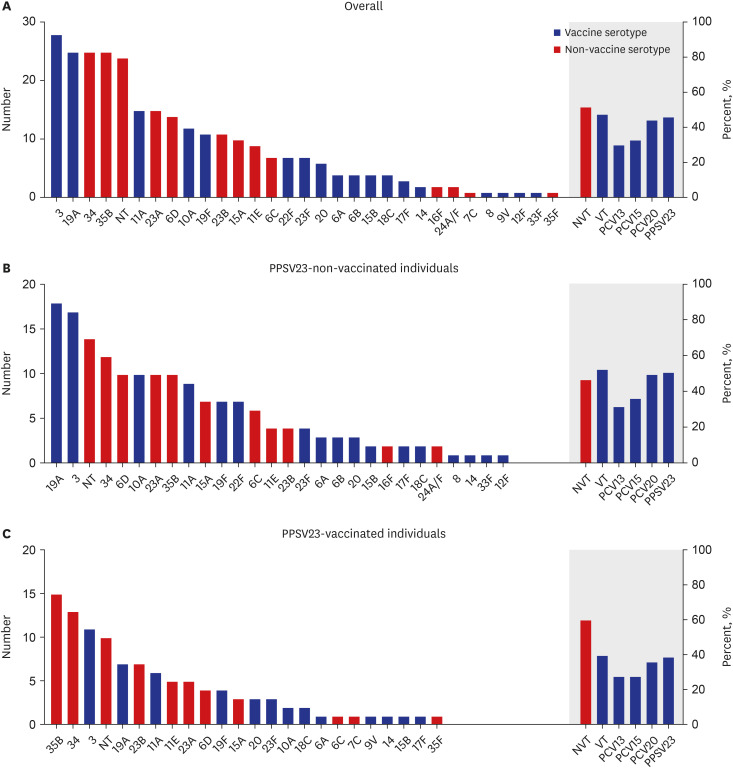
Table 3
Serotype distribution of pneumococcal community-acquired pneumonia and comparison of serotype distribution by PPSV23 vaccination status
Serotype 3 pCAP
We compared the demographic and clinical features of patients with serotype 3 pCAP (n = 28) and those with other serotypes of pCAP (n = 252) and found no variation in mean age and sex between groups (Table 4). Serotype 3 pCAP was more common in spring (50% vs. 25.4%) and individuals with chronic lung diseases (42.9% vs. 20.6%, P = 0.008) than other pCAP serotypes. PPSV23/PCV13 vaccination rates did not differ between the two groups (PPSV23: 39.3% vs. 38.5%, P = 0.935; PCV13: 7.1% vs. 11.1%, P = 0.750). The rate of respiratory viral infection was higher in serotype 3 pCAP than in other pCAP serotypes, although statistically insignificant (17.9% vs. 9.1%, P = 0.176).
Table 4
Comparison of serotype 3 with other serotypes of CAP
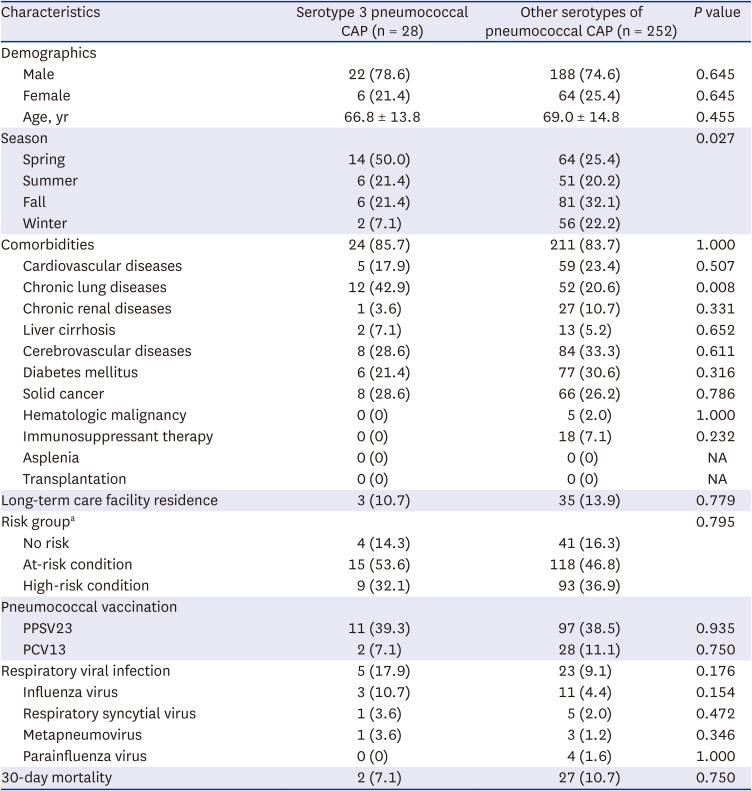
Data are shown as mean ± standard deviation or number (%).
CAP = community-acquired pneumonia, PPSV23 = 23-valent pneumococcal polysaccharide vaccine, PCV13 = 13-valent pneumococcal conjugated vaccine, NA = not available.
aNo risk: without any comorbidity; at-risk condition: presence of chronic lung disease, congestive heart failure, chronic liver disease, neurologic disease, or diabetes mellitus without a “high-risk” condition; high-risk condition: presence of human immunodeficiency virus infection, solid organ/hematopoietic stem cell transplantation, solid/hematologic cancer, functional/anatomical asplenia, chronic kidney disease, or use of immunosuppressive agents.
Risk factors of mortality in hospitalized patients with pCAP
The comparison of demographics, comorbidities, and clinical characteristics of patients with pCAP by 30-day mortality were presented in Supplementary Table 2. Compared to survived patients (n = 532), the non-survived patients (n = 57) were significantly older (69.8 ± 14.8 vs. 74.7 ± 11.0, P = 0.015), higher rate of comorbidities (79.3% vs. 91.2%, P = 0.031), higher rate of long-term care facility residence (13.5% vs. 26.3%, P = 0.010), and higher rate of bacteremia (3.9% vs. 12.3%, P = 0.005) (Supplementary Table 2). In the univariate analysis, age, high-risk condition, long-term care facility residence and bacteremia significantly increased the risk of 30-day all-cause mortality (Table 5), while the PPSV23 vaccination status was not associated with mortality (OR, 0.789; 95% CI, 0.445–1.401). In the multivariate analysis, advanced age (adjusted OR [aOR], 1.040; 95% CI, 1.011–1.071), long-term care facility (aOR, 2.161; 95% CI, 1.071–4.357) and bacteremia (aOR, 4.193; 95% CI, 1.604–10.962) were independent risk factors of mortality. PPSV23 vaccination showed a protective effect against mortality (aOR, 0.507; 95% CI, 0.267–0.961) in the multivariate analysis. The characteristics of PPSV23-vaccinated and non-vaccinated individuals with pCAP were presented in Supplementary Table 3.
Table 5
Univariate and multivariate analyses of mortality rates in hospitalized patients with pneumococcal CAP
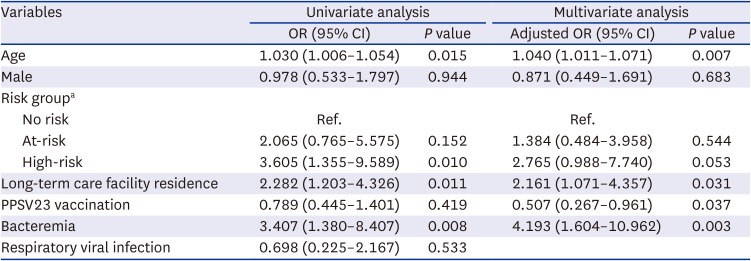
CAP = community-acquired pneumonia, OR = odd ratio, CI = confidence interval, Ref = reference, PPSV23 = 23-valent pneumococcal polysaccharide vaccine.
aNo risk: without any comorbidity; at-risk condition = presence of chronic lung disease, congestive heart failure, chronic liver disease, neurologic disease, or diabetes mellitus without a “high-risk” condition; high-risk condition: presence of human immunodeficiency virus infection, solid organ/hematopoietic stem cell transplantation, solid/hematologic cancer, functional/anatomical asplenia, chronic kidney disease, or use of immunosuppressive agents.
DISCUSSION
This prospective hospital-based cohort study generated the following key findings: 1) S. pneumoniae was the leading causative agent of CAP, particularly in individuals aged < 65 years with chronic medical conditions, for whom pneumococcal vaccine uptake rate was low; 2) individuals who received the PPSV23 had a significantly lower rate of pCAP caused by the PPSV23 or PCV20 serotypes compared to those who were not vaccinated; 3) serotype 3 was the most common cause of pCAP, followed by serotypes 19A, 34, and 35B; 4) compared to other serotypes, serotype 3 pCAP appeared to be more common in individuals with chronic lung disease; and 5) old age, immunocompromised conditions, and concomitant respiratory viral infections were associated with increased 30-day mortality in patients with CAP. Our findings suggested that PPSV23 vaccination may lower 30-day mortality risk.
In our study, pneumococcus was the most common causative agent of CAP (11.8%), which is consistent with other studies conducted in the US (12.3%), Canada (11.4%), and Italy (13.1%).192022 We found that the pneumococcal vaccination coverage (≥ 1 dose of PPSV23 or PCV13) among adults aged ≥ 65 years was 61.7%, which is not much lower than that in the US (67.5%). However, coverage among adults aged < 65 years with chronic medical diseases was considerably lower (10.4%) than that in the US (23.9%).23 Given the low uptake of pneumococcal vaccines and the high incidence of pCAP in this population, increased vaccination efforts in South Korea could potentially reduce disease burden.
Previous studies showed that the introduction of PCV resulted in a serotype replacement of VT-related with NVT-related pneumococcal diseases.1011121314161724 Serotype replacement can offset the overall benefit of pneumococcal vaccination if the incidence of NVT pneumococcal disease increases or if it is highly invasive. One study reported that the introduction of PCV did not affect overall pneumococcal carriage rate but increased the carriage rate of NVT pneumococcus.25 Although IPD was notably reduced in both children and adults after the introduction of PCV, a considerable effect on overall CAP or pCAP burden has not been demonstrated.17202627 In the present study, the overall NVT pCAP rate was 52.1% and its prevalence was significantly higher in PPSV23-vaccinated individuals compared to that in non-vaccinated individuals (60.2% vs. 47.1%, P = 0.033). It could be presumed that PPSV23 vaccination provided some degree of protective effect against pCAP of VTs, including both PCV13 and non-PCV13/PPSV23 serotypes. Therefore, the prevalence, virulence, and clinical characteristics of NVT pneumococci should be carefully monitored in response to serotype replacement and may necessitate the development and introduction of a novel extended-valent pneumococcal vaccine.
Serotypes 3 and 19A are problematic worldwide.24282930 In previous studies in South Korea, serotypes 3 and 19A were the most common causes of pCAP, accounting for 12.5% and 14.3% in 2007–2011 and 19.6% and 9.3% in 2015–2017, respectively.2830 In the present study, serotypes 3 and 19A remained the most common causes of pCAP, accounting for 10.0% and 8.9% of cases in 2018–2021, respectively. Previous studies have shown that a higher level of functional antibodies is required to protect against these compared to other serotypes based on the immune correlate of protection.3132 One study of 10 European countries showed a direct and indirect effect of pediatric PCV13 vaccination in reducing the incidence of IPD caused by serotype 19A.10 Another study estimated that it could take 7.6 years to reduce 90% of IPD cases caused by serotype 19A in all age groups after pediatric PCV13 introduction.9 Therefore, it is possible that the indirect effects of pediatric PCV13 in South Korea have not been fully realized. In our study, the prevalence of serotype 19A pCAP (8.9%) in 2018–2021 was lower than the estimated incidence of 14.3% in 2007–2011 and 9.3% in 2015–2017.2830 This reduction in serotype 19A pCAP incidence may be related to the indirect effects of pediatric PCV13 vaccinations. Moreover, the lower incidence of serotype 19A pCAP in PPSV23-vaccinated individuals in our study may be related to the direct effects of adult pneumococcal vaccination. However, the prevalence of serotype 3 pCAP did not differ according to PPSV23 vaccination status in our study. The thick CPS of serotype 3 pneumococcus and CPS shedding may interfere with antibody-dependent bacterial death. The mucoid property of serotype 3 pneumococcus may also promote immune evasion and colonization in the nasopharynx.3334 Considering the low PCV13 vaccination rate in adults, it would be necessary to encourage individual PCV13 vaccination for adult risk groups (elderly people and chronically ill patients). Particularly, in our study, serotype 3 pCAP was more common in individuals with chronic lung disease. Predisposing factors for serotype 3 pCAP have not been well demonstrated; however, considering the properties of serotype 3 pneumococci and the higher bacterial colonization rate in individuals with chronic lung disease, chronic lung disease is a likely risk factor for infections with serotype 3 pCAP, though further investigation is necessary. Some clinical trials of PCV15 have reported superior immunogenicity against serotype 3 pneumococcus compared to PCV13.3536 Although the real-world effectiveness of PCV15 is unclear, our study highlights the need for increased efforts in the development of better immunogenic pneumococcal vaccines against serotype 3 pneumococci to overcome disease burden.
Among the PPSV23-vaccinated individuals in our study, serotype 35 B (13.9%) was the most common, followed by serotype 34 (12.0%), which are NVT pneumococci. Serotypes 34 and 35 B were the second-most common serotypes (both 8.9%), occurring at the same level as serotype 19A. The proportions of serotypes 34 and 35 B pCAP were considerably higher than previously reported: 3.6% and 4.2% in 2007–2011 and 5.6% and 2.8% in 2015–2017, respectively.2830 Although serotypes 34 and 35 B reportedly have lower invasive disease potential, monitoring their future trends is important because the rate of invasive disease caused by these serotypes has increased since the introduction of PCVs.3738
The mortality risk of pneumonia is associated with diverse factors including advanced age, male sex, medical comorbidities, and disease severity.39 In our study, advanced age, long-term care facility, PPSV23 vaccination and bacteremia were independent risk factors for mortality. The non-significant finding of PPSV23 vaccination in the univariate analysis might be attributed to the advanced age and higher rate of comorbidities among PPSV-23-vaccinated individuals. However, after adjusting for these factors, PPSV23 vaccination demonstrate statistically significant. A recent study reported that PPSV23 was no longer effective in protecting against all-cause CAP and pCAP after the introduction of pediatric PCV.40 However, PPSV23 vaccination significantly lowered the risk of all-cause mortality in patients with pCAP in our study and was still beneficial in this respect.
This study had some limitations. First, serotyping data were available for only 280 of the 589 pCAP cases. Second, respiratory viral PCR was conducted in only 35.2% of patients with CAP; therefore, concomitant respiratory viral infections might be underestimated. A major strength of our study is that the analyses and evaluation of pneumococcal serotype distribution were based on data collected from multiple centers.
In conclusion, serotype 3 pneumococci were the most common cause of pCAP in the adult South Korean population in the era of PCV13, particularly in patients with chronic lung disease. PPSV23 vaccination might reduce the mortality rates in patients with pCAP.
 XML Download
XML Download