

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The most frequent causes of unilateral sensorineural hearing loss are sudden deafness, Menière’s disease and cerebellopontine angle tumors. Early diagnosis of acoustic neuroma (AN) or other lesions of the internal auditory meatus or cerebello-pontine angle requires special attention.1 In general, acoustic neuromas have a benign course and slow growth rate of 0 to 1.8 mm per year or growth arrest.234567 Even though an AN is not a life-threatening tumor, it could compromise the quality of life by compressing or irritating the fifth, sixth, or seventh cranial nerves as well as eighth cranial nerves. Long-lasting ANs could also cause brain stem compression or hydrocephalus requiring a ventriculoperitoneal (VP) shunt.
Since an AN was first treated by radiosurgery in 1969,8 stereotactic radiosurgery (SRS) has shown good tumor control and low morbidity rates and has been regarded as an acceptable alternative to surgical resection for ANs. Despite the debate over the optimal treatment for ANs, SRS has become more popular due to its effectiveness and less invasiveness.910
Since Kondziolka et al.11 first reported the long-term outcome of 162 patients who underwent gamma knife radiosurgery (GKS) as an initial or adjuvant treatment for acoustic neuromas in 1998, there has been no report of a comprehensive analysis of what has changed in GKS practice and the long-term outcomes of patients with ANs. The aim of this study was to retrospectively evaluate the very long-term outcomes of patients who underwent GKS for ANs in single institution, including the tumor control rates, hearing preservation, and associated complications, and provide a literature review.
METHODS
Patients
Between December 1997 and December 2004, 272 patients with ANs underwent 285 GKS sessions at the Gamma Knife Center. To investigate the outcome of GKS as an initial treatment option for AN, 98 patients who had previously undergone surgical resection or radiation were excluded. Twenty-six patients diagnosed with neurofibromatosis type II and 47 patients with clinical follow-up periods of less than 10 years were excluded. The remaining 106 patients who had unilateral sporadic ANs and no previous history of surgical resection or radiation were enrolled in this retrospective study.
The mean patient age was 50 years (range, 21–76 years). There were 48 men (45.3%) and 58 women (54.7%). The mean clinical follow-up duration was 153 ± 23 months (median, 148 months; range, 120–216 months). The most common initial presentation was hearing difficulty (69 patients, 65.1%), followed by tinnitus (53 patients, 50.0%), dizziness (23 patients, 21.7%), headache (22 patients, 20.8%), facial paresthesia (10 patients, 9.4%), facial hypesthesia (9 patients, 9.3%), facial palsy (2 patients, 1.9%), and hemifacial spasm (2 patients, 1.9%). Two patients with facial palsy had complete hearing loss and there was no image finding suggestive a facial nerve schwannoma. Ans were incidentally found without clinical symptoms in 3 patients (2.8%). Twenty-five patients (23.6%) had tumors confined to the internal auditory canal (IAC), 12 patients (11.3%) harbored cerebellopontine angle (CPA) cisternal tumors, and 69 patients (65.1%) had tumors occupying both the IAC and CPA cistern. The authors classified all tumors by the tumor component; 89 patients (84.0%) had solid-only tumors, and 17 patients (16.0%) had cystic mixed components. The mean initial tumor volume was 3.68 ± 4.42 cm3 (range, 0.10–23.30 cm3).
Of the 106 patients enrolled in this study, 56 (52.8%) had serviceable hearing based on Gardner Robertson (G-R) scale grades; 32 patients had G-R grade I, and 24 patients had G-R grade II.12 Seventeen patients with G-R grade III, 3 patients with G-R grade IV, and 30 patients with G-R grade V were classified into the non-serviceable hearing group.
Stereotactic radiosurgery
Radiosurgery was performed on the patients under local anesthesia, supplemented with intravenous sedation. Patients were treated using the Leksell Gamma Knife (model B or C, Elekta Instrument AB) with the Leksell Gamma Plan (Elekta, Stockholm, Sweden). The median marginal tumor dose was 12.5 Gy (range, 8.0–15.0 Gy), the median covered ratio was 94% (range, 90–99%), and the isodose line for the tumor margin varied from 45% to 50% (median isodose line 50%). The mean dose and maximal dose to cochlea was 3.60 ± 2.60 Gy and 7.95 ± 2.60 Gy, respectively. And, the mean dose and maximal dose to cochlear nucleus was 4.64 ± 2.46 Gy and 9.17 ± 2.90 Gy, respectively.
Follow-up and outcome analysis
Patients underwent follow-up clinical evaluations 1, 3, 6, and 12 months after SRS and annually thereafter. Magnetic resonance imaging (MRI) was performed 6, 12, 18, and 24 months after GKS, then biannually thereafter. The radiologic volume status of the tumors was determined by the percentage ratio of the last follow-up tumor volume to the initial volume, and classified as increased (≥ 120%), stationary (80–120%), or decreased (< 80%).
Statistical analysis
The tumor control rate was established using the Kaplan-Meier product-limit method. Differences were assessed using the log-rank test, and statistical significance was accepted at P < 0.050. Stepwise backward multivariate analysis was performed using the Cox proportional hazard function, and P < 0.050 was considered statistically significant. All statistical analyses were performed with the SPSS statistical software package (version 22.0; IBM Corp., Armonk, NY, USA).
Ethics statement
This retrospective study was approved by the Institutional Review Board of Seoul National University Hospital (IRB No. 1704-111-847) and conformed to the principles of the Declaration of Helsinki. Informed consent was waived because of the retrospective design of the study and anonymous clinical data.
RESULTS
Tumor control
All 106 patients enrolled in this study were alive at the point of this study. The MRI volumetric assessment results at the time of the last follow-up were as follows: volume increased in 11 patients (10.4%), remained stationary in 27 (25.5%), and decreased in 68 patients (64.2%). The actuarial 3-, 5-, 10-, 15-year tumor control rates were 95.3 ± 2.1%, 94.3 ± 2.2%, 87.7 ± 3.2%, and 86.6 ± 3.3%, respectively (Fig. 1).
Fig. 1
Cumulative tumor control rates after GKS. (A) Cumulative tumor control rates of all 106 patients. The actuarial 3, 5, 10, and 15-year tumor control rates were 95.3 ± 2.1%, 94.3 ± 2.2%, 87.7 ± 3.2%, and 86.6 ± 3.3%, respectively. (B) Cumulative tumor control rates stratified into 4 groups according to the initial tumor volume. The 10-year actuarial tumor control rates were 92.7 ± 4.1%, 90.0 ± 5.5%, 91.3 ± 5.9%, and 58.3 ± 14.2% in the patient group with initial tumor volumes of < 1 cm3, 1–4 cm3, 4–8 cm3 and ≥ 8 cm3, respectively (P = 0.010). (C) Cumulative tumor control rates stratified into 2 groups according to marginal dose. The 10-year actuarial tumor control rates were 69.2 ± 12.8% and 90.3 ± 3.1% in the patient group with initial marginal doses of < 12 Gy and ≥ 12 Gy, respectively (P = 0.032).
GKS = gamma knife radiosurgery.
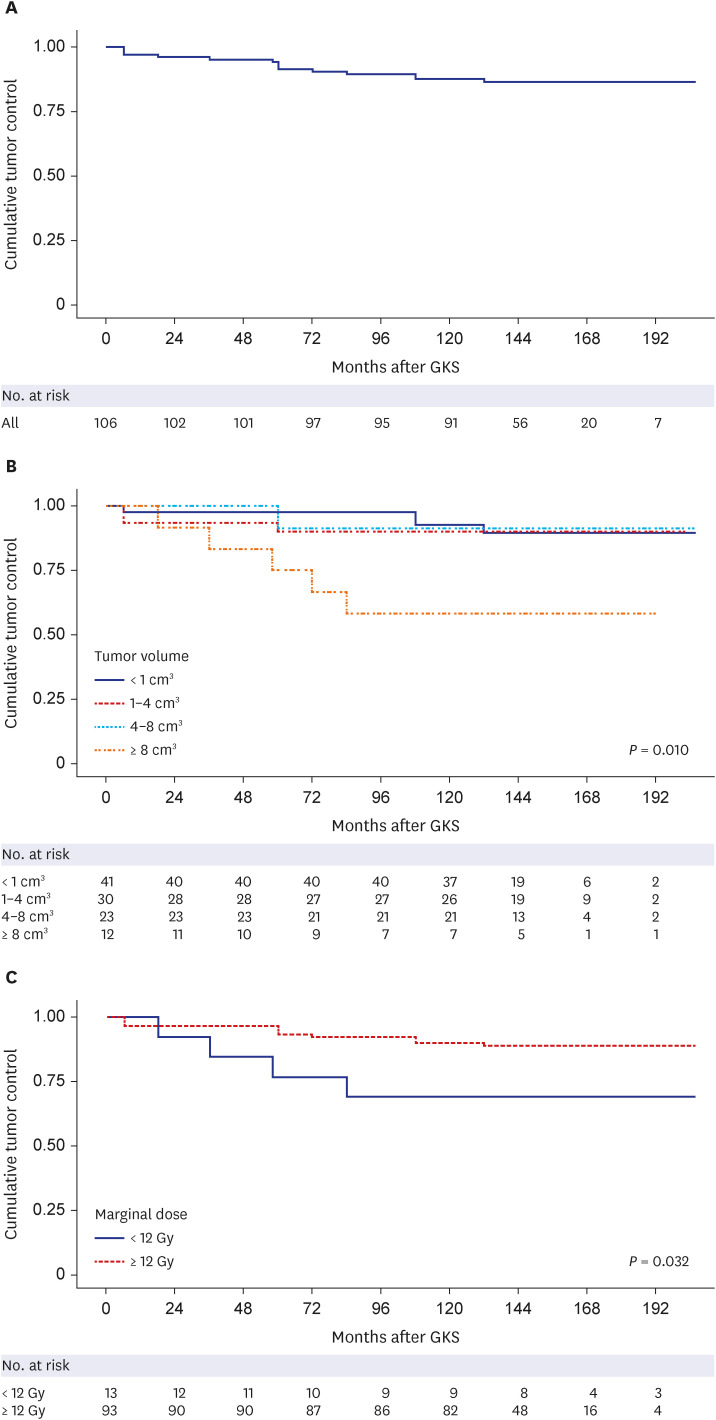
There was no statistically significant prognostic factor correlated with tumor control failure in either the uni- or multivariate analyses (Supplementary Table 1).
Within 24 months after GKS, an immediate tumor volume expansion of more than 120% compared to the initial volume was observed in 35 patients (33.3%). The median interval between GKS and the occurrence of tumor volume expansion occurrence was 6 months (range, 6–24 months), and the mean rate of volume expansion was 148.9% (range, 120.51–559.5%). About 60% of the patients showed a central loss of contrast enhancement in the MRI at 3- or 6-month follow-ups (Supplementary Table 2). We could not find significant correlation between changes in contrast enhancement and tumor control (P = 0.913).
Hearing preservation
Fifty-six patients (52.8%) had serviceable hearing before GKS; 32 patients had G-R scale I and 24 patients had G-R scale II. The hearing outcome was determined by G-R scale grades at the final follow-up visit. Of the 56 patients who had serviceable hearing at the time of GKS, 16 patients (28.6%) maintained the same G-R scale grade, 26 patients (46.4%) maintained serviceable hearing, and 40 patients (71.4%) experienced hearing deterioration defined as a PTA increase of ≥ 20 dB. The G-R scale grade at baseline and the last follow-up visit are described in Table 1 and Supplementary Fig. 1. There was no statistically significant difference in cochlear dose at the time of GKS between the serviceable hearing preservation group (mean ± SD, 4.50 ± 2.21 Gy) and the loss group (4.87 ± 2.95 Gy, P = 0.569).
Table 1
G-R scale before and after GKS
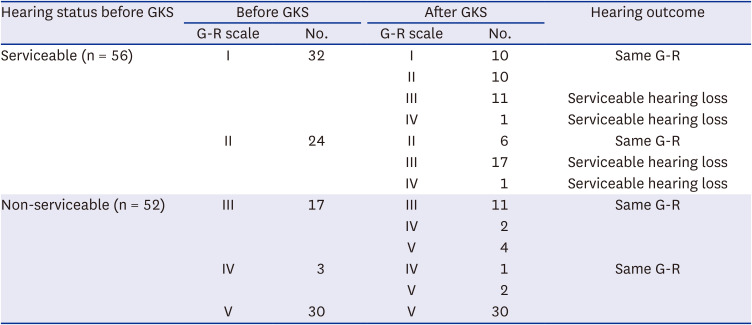
The hearing outcome was determined by G-R scale at the final follow-up visit. Of the 56 patients who had serviceable hearing at the time of GKS, 16 patients (28.6%) maintained the same G-R scale, 26 patients (46.4%) maintained serviceable hearing, and 40 patients (71.4%) suffered hearing deterioration defined as PTA increase ≥ 20 dB. This table describes the G-R scale at baseline and the last follow-up visit. We subdivided 56 patients who had pre-GKS serviceable hearing into four groups according to the pure tone average: ≤ 10 dB (n = 3), 10−20 dB (n = 12), 20−30 dB (n = 17), and 30−50 dB (n = 24). There was a significant difference in the G-R scale of the patients in each group after GKS (P = 0.004). As described in Fig. 2, among the patients who had serviceable hearing with pure tone average of 20 dB or less before GKS, 10 out of 15 (66.7%) maintained serviceable hearing of G-R scale I or II. However, 10 out of 17 patients (58.8%) in the patients with pure tone average 20–30 dB and 6 out of 24 (25.0%) in the patients with 30–50 dB maintained serviceable hearing. Even within the group of patients who had the same serviceable hearing before GKS, the higher the remaining hearing, the higher the serviceable hearing preservation rate.
G-R = Gardner Robertson, GKS = gamma knife radiosurgery.
Facial neuropathy
Both of the two patients who experienced facial neuropathy expressed as facial palsy before GKS experienced an improvement in facial palsy with a decline in the House-Brackmann (H-B) facial nerve grade. Over the follow-up periods after GKS, the facial nerve preservation rate was 97.2%. Three patients (2.8%) experienced newly developed facial neuropathy. The tumor volume of the patients who experienced newly developed facial neuropathy was significantly larger than that of the patients without further facial neuropathy (9.44 ± 9.34 cm3 vs. 3.57 ± 4.19 cm3, P = 0.023). The marginal doses of each patient were 9, 12, and 12 Gy, and the doses were not higher than those of other patients. Only 1 of 3 patients had transient volume enlargement, but the tumor eventually shrank and was controlled.
Trigeminal neuropathy
Nineteen patients (17.9%) had trigeminal neuropathy such as paresthesia (10 patients) and hypesthesia (9 patients) before GKS. Of the 10 patients presenting with paresthesia, 5 patients (50.0%) obtained symptom relief, and 5 patients (50.0%) remained stationary after GKS. The trigeminal nerve preservation rate after GKS was 94.3%. Trigeminal neuropathy was newly developed in 5 patients (5.7%), with hypesthesia in 3 patients, and paresthesia in 2 patients. Transient volume enlargement occurred in 2 of 5 patients, but tumors were controlled in all 5 patients. The mean initial tumor volume of the patients who experienced newly developed trigeminal neuropathy was significantly larger than that of the patients without further trigeminal neuropathy (9.71 ± 10.73 cm3 vs 2.46 ± 2.71 cm3, P < 0.001).
Hydrocephalus associated with acoustic neuroma
At the time of the GKS, 5 patients (4.7%) presented with hydrocephalus defined as an Evans ratio of > 0.3. Four of them displayed hydrocephalus-related symptoms, and 2 of them received a VP shunt for cerebrospinal fluid (CSF) diversion before radiosurgery. Newly developed hydrocephalus over the follow-up periods was discovered in 5 patients (4.9%). Two patients required a VP shunt for symptom-related hydrocephalus. The interval time between GKS and placement of the VP shunts was 3 and 12 years, respectively.
Delayed cyst formation
Of the 89 patients who had solid tumors, 7 patients (7.9%) experienced delayed cyst formation over the follow-up periods; intratumoral cysts developed in 6 patients and an extratumoral cyst in 1 patient (Supplementary Fig. 2). The median interval time between GKS and cyst formation was 6 months (range, 6–60 months). Five patients received close observation for cysts, and 2 patients underwent surgical resection 58 and 84 months after GKS, respectively.
Salvage treatment
After GKS, 8 patients required additional treatments. There were 6 cases of surgical resection due to uncontrollable tumor growth, and 2 cases of VP shunt for hydrocephalus causing associated symptoms. The median interval between GKS and further surgical resection of the 6 patients who underwent surgical resections was 66 months (range, 18–132 months). The histological diagnosis was compatible with schwannoma in all 6 patients.
DISCUSSION
The actuarial tumor control rates in this study were 94.3% at 5 years and 87.7% at 10 years, which was consistent with previous reports.
In the tumor control group, all tumors were decreased, which is plotted in Fig. 2A. Based on this plot, we proposed a formula that could predict the change in tumor volume after the first 2 years after SRS using linear regression analysis. Using this formula, the approximate percent change in tumor volume (y) at t months after SRS can be predicted: y(t) = 100 − 0.471t.
Fig. 2
Chronological tumor volume plotting. (A) Tumor volume plotting of the tumor control group. GKS treatment not only prevented tumor growth but also gradually induced tumor volume shrinkage over time after GKS, resulting in an average of about 60% after 150 months compared to 100% of the tumor volume at the time of GKS. In the first 2 years, the tumor was temporarily swollen due to the vascular insult caused by radiation, making it difficult to predict, but after 2 years it was generally consistent with the change in tumor volume. We proposed a formula that could predict the change in tumor volume after the first 2 years after SRS using linear regression analysis. Using this formula, the approximate percent change in tumor volume (y) at t months after SRS could be predicted as shown in this figure: y(t) = 100 − 0.471t. (B) Tumor volume plotting of all 126 patients with imaging follow-up of at least 2 years. As the subjects of this study included patients who had been followed for more than 10 years, bias may occur due to study design. To overcome this, this figure represents tumor volume plotting of all 126 patients who were clinically followed for less than 10 years, if they underwent follow-up image for at least 2 years.
GKS = gamma knife radiosurgery, SRS = stereotactic radiosurgery.
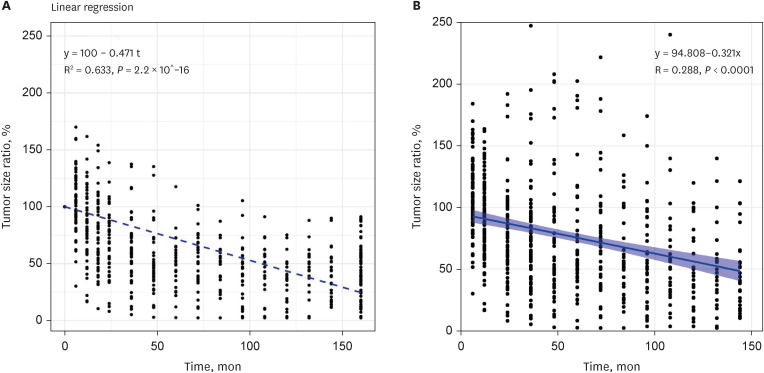
We also plotted the tumor volume of all 126 patients including tumor control failure group and patients with imaging follow-up of at least 2 years, who were excluded from this study because of the follow-up period of less than 10 years (Fig. 2B). Of the 14 patients with tumor control failure in this study, 6 patients experienced sudden tumor volume enlargement in the late periods between 5 and 11 years after GKS. We recommend more than 5 years of imaging follow-up to assess the tumor control outcomes in patients with AN after GKS.
We found that tumor volume expansion occurred within 24 months after GKS in 33.3% of the patients. The incidence rates of transient volume expansion vary from 5% to 39% in the literature review, and expansion is known to persist until 24–30 months after GKS.1314151617181920 Of the 35 patients with volume expansion after GKS in this study, 28 patients (80%) eventually obtained tumor control, and 7 patients (20%) experienced sustained tumor growth (Supplementary Fig. 3). Of the 7 patients with continuous tumor growth, one patient underwent surgical resection due to increased tumor volume associated with relevant symptoms. Another one patient has been under close observation without surgery due to old age and comorbidities despite the deterioration of dizziness, and the remaining 5 patients have been under close observation without any associated symptoms.
Although the risks of other cranial nerve neuropathies after GKS were dramatically decreased, the risk of serviceable hearing preservation still ranged between 40% and 70%.2122 Because of the earlier use of higher-quality MRI followed by an increasing number of patients with useful or normal hearing, hearing preservation has become a more important issue.
In this study, the rates of maintaining the same G-R scale grade and preserving serviceable hearing were 28.6% and 46.4%, respectively, after GKS with a median tumor marginal dose of 12.5 Gy. And the lower the pure tone average before GKS, the higher the rate of maintaining serviceable hearing after GKS. In a follow-up study without treatment, the average annual hearing loss speed was 2.3 dB/year.23 Other studies comparing observation and surgical intervention recommend active therapy rather than observation in terms of hearing preservation.2425
Since the Pittsburgh group investigated the superiority of low dose of 12–13 Gy compared to high doses of 16 Gy or more, GKS for AN with 12–13 Gy has provided high rates of tumor control and low rates of serviceable hearing loss and cranial nerve neuropathy occurrence.2627 The factors we considered for GKs planning were mainly tumor volume and serviceable hearing preservation. In most cases where the tumors were not very large, a marginal dose of 12 Gy was prescribed. If there is no serviceable hearing on the tumor side, 13 Gy was prescribed to obtain satisfactory tumor control. In cases with large tumor size and serviceable hearing, a marginal dose of 12 Gy or less was prescribed for serviceable hearing preservation. To investigate the optimal dose for ANs, we stratified the tumor marginal dose into 5 classes (< 12 Gy, 12 Gy, 12.5 Gy, 13 Gy, and > 13 Gy) and compared the tumor control rates, serviceable hearing preservation rates, and cranial neuropathy occurrence rates. As shown in Supplementary Table 3, patients who received marginal doses of less than 12 Gy revealed higher tumor control failure rates (P = 0.129) and newly occurred facial or trigeminal neuropathy rates (P = 0.040 and P = 0.313, respectively).
Recently published studies have shown that biologically effective dose (BED), rather than absolute dose, has a significant correlation with clinical outcomes including hearing preservation and tumor control rates.4950 By accounting for various factors, including the total radiation dose, the fractionation scheme, and the tumor’s radiobiological parameters, the BED aims to provide a more accurate estimation of the biological effectiveness of a radiation treatment. When determining the optimal dose, it is necessary to refer to recent research results on BED.
After Kondziolka et al.11 demonstrated long-term outcomes after radiosurgery for acoustic tumors in 1998, radiosurgery has emerged as an alternative treatment for microsurgery, especially for intracanalicular or small- or medium-sized tumors. Since then, the number of radiosurgical cases for ANs has increased steadily every year. According to data suggested by Elekta, ANs accounted for about 8.8% of all GKS cases in 2019, and the number of cumulative patients who received GKS with AN increased by 11.7 times from 10,730 in 1998 to 125,710 in 2019.
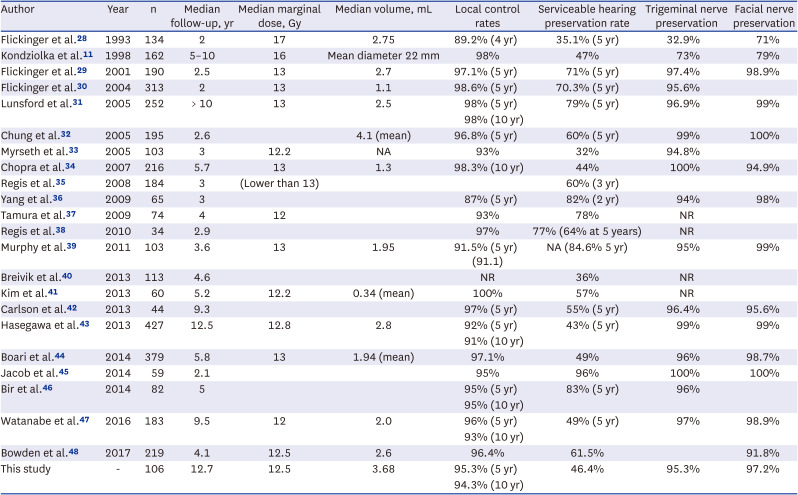
Table 2 summarizes the literature reporting the long-term outcomes of radiosurgery for AN. Compared to the first report by the Kondziolka group,11 there has been a change in the trend of radiosurgery for ANs. Although the marginal dose has gradually decreased from 16–17 Gy at the beginning to 12–13 Gy now, the tumor control rate was maintained at above 95% in most studies. Because the marginal dose was reduced, facial and trigeminal nerve preservation was better than before, but the hearing preservation rate did not change significantly.
Table 2
Prior studies reporting long-term outcomes of GKS for ANs
| Author | Year | n | Median follow-up, yr | Median marginal dose, Gy | Median volume, mL | Local control rates | Serviceable hearing preservation rate | Trigeminal nerve preservation | Facial nerve preservation |
|---|---|---|---|---|---|---|---|---|---|
| Flickinger et al.28 | 1993 | 134 | 2 | 17 | 2.75 | 89.2% (4 yr) | 35.1% (5 yr) | 32.9% | 71% |
| Kondziolka et al.11 | 1998 | 162 | 5–10 | 16 | Mean diameter 22 mm | 98% | 47% | 73% | 79% |
| Flickinger et al.29 | 2001 | 190 | 2.5 | 13 | 2.7 | 97.1% (5 yr) | 71% (5 yr) | 97.4% | 98.9% |
| Flickinger et al.30 | 2004 | 313 | 2 | 13 | 1.1 | 98.6% (5 yr) | 70.3% (5 yr) | 95.6% | |
| Lunsford et al.31 | 2005 | 252 | > 10 | 13 | 2.5 | 98% (5 yr) | 79% (5 yr) | 96.9% | 99% |
| 98% (10 yr) | |||||||||
| Chung et al.32 | 2005 | 195 | 2.6 | 4.1 (mean) | 96.8% (5 yr) | 60% (5 yr) | 99% | 100% | |
| Myrseth et al.33 | 2005 | 103 | 3 | 12.2 | NA | 93% | 32% | 94.8% | |
| Chopra et al.34 | 2007 | 216 | 5.7 | 13 | 1.3 | 98.3% (10 yr) | 44% | 100% | 94.9% |
| Regis et al.35 | 2008 | 184 | 3 | (Lower than 13) | 60% (3 yr) | ||||
| Yang et al.36 | 2009 | 65 | 3 | 87% (5 yr) | 82% (2 yr) | 94% | 98% | ||
| Tamura et al.37 | 2009 | 74 | 4 | 12 | 93% | 78% | NR | ||
| Regis et al.38 | 2010 | 34 | 2.9 | 97% | 77% (64% at 5 years) | NR | |||
| Murphy et al.39 | 2011 | 103 | 3.6 | 13 | 1.95 | 91.5% (5 yr) (91.1) | NA (84.6% 5 yr) | 95% | 99% |
| Breivik et al.40 | 2013 | 113 | 4.6 | NR | 36% | NR | |||
| Kim et al.41 | 2013 | 60 | 5.2 | 12.2 | 0.34 (mean) | 100% | 57% | NR | |
| Carlson et al.42 | 2013 | 44 | 9.3 | 97% (5 yr) | 55% (5 yr) | 96.4% | 95.6% | ||
| Hasegawa et al.43 | 2013 | 427 | 12.5 | 12.8 | 2.8 | 92% (5 yr) | 43% (5 yr) | 99% | 99% |
| 91% (10 yr) | |||||||||
| Boari et al.44 | 2014 | 379 | 5.8 | 13 | 1.94 (mean) | 97.1% | 49% | 96% | 98.7% |
| Jacob et al.45 | 2014 | 59 | 2.1 | 95% | 96% | 100% | 100% | ||
| Bir et al.46 | 2014 | 82 | 5 | 95% (5 yr) | 83% (5 yr) | 96% | |||
| 95% (10 yr) | |||||||||
| Watanabe et al.47 | 2016 | 183 | 9.5 | 12 | 2.0 | 96% (5 yr) | 49% (5 yr) | 97% | 98.9% |
| 93% (10 yr) | |||||||||
| Bowden et al.48 | 2017 | 219 | 4.1 | 12.5 | 2.6 | 96.4% | 61.5% | 91.8% | |
| This study | - | 106 | 12.7 | 12.5 | 3.68 | 95.3% (5 yr) | 46.4% | 95.3% | 97.2% |
| 94.3% (10 yr) |
Table 2 summarizes the literature reporting the long-term outcome of radiosurgery for AN. Compared to the first report of the Kondziolka group,11 there has been a change in the trend of radiosurgery for ANs. Although the marginal dose was gradually decreased from 16–17 Gy at the beginning to 12–13 Gy now, the tumor control rate has been maintained above 95% in most studies. Because the marginal dose was reduced, the facial and trigeminal nerve preservation was better than before, but the hearing preservation rate did not change significantly.
GKS = gamma knife radiosurgery, AN = acoustic neuroma, NA = not applicable, NR = not reported.
To reiterate the role of radiosurgery in ANs, a meta-analysis comparing radiosurgery and microsurgery as a primary treatment for small- to medium-sized sporadic ANs was conducted, which showed that although the tumor control rate was better in the microsurgery group, the facial nerve and hearing preservation outcomes and quality of life were superior in the radiosurgery group.51
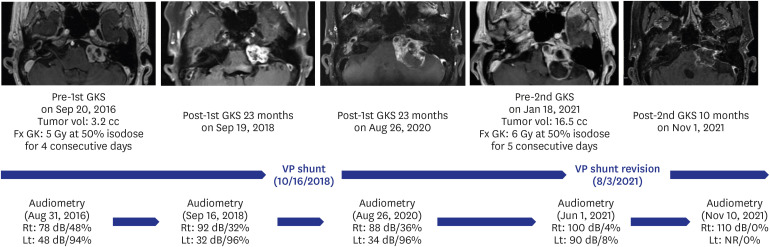
The remaining controversy in presenting GKS as a primary treatment for AN is as an alternative for the management of large-sized ANs and better hearing preservation. We can consider the inclusion of brain MRI with audiometry in the health screenings of people over 40 for early diagnosis before the onset of hearing loss. Subtotal resection with functional preservation followed by GKS or fractionated GKS (FGKS) can be suggested as an alternative for the treatment of large-sized ANs (Fig. 3). With the recent introduction of ICON™, clinical experience with frameless FGKS is gradually accumulating, and dose optimization may be done using the accumulated results in the near future.
Fig. 3
Case of one patient who underwent FGKS using a frame for AN. We implemented FGKS using a frame before the introduction of ICON™. This case represents one of the patients who underwent FGKS for an AN. An adult patient with a left AN of 3.2 mL underwent FGKS at a marginal dose of 5 Gy per fraction for 4 consecutive days. Afterward, an additional ventriculoperitoneal shunt was required for progressive hydrocephalus. After 52 months, the second stage of FGKS was performed with a marginal dose of 6 Gy per fraction for 5 consecutive days. The ten-month follow-up MRI confirmed that shrinkage occurred along with necrosis inside the tumor.
FGKS = fractionated gamma knife radiosurgery, AN = acoustic neuroma, MRI = magnetic resonance imaging, VP = ventriculoperitoneal.
This study included patients who underwent very long-term follow-up compared to previous studies. However, this study had some drawbacks. One of them is the retrospective study design; the information that could be obtained from medical records was limited. In addition, selection bias could have occurred since only patients with more than 10 years of follow-up were included. More systematic studies under prospective control are required.
In conclusion, GKS as an initial treatment for small ANs that are detected early could be helpful in terms of tumor control, the preservation of serviceable hearing, and the prevention of cranial neuropathy, which can be the rationale for early GKS for ANs. Better treatment outcome of GK SRS can be expected, when the size of the AN is small and the hearing is preserved. It is recommended to perform GKS as soon as possible not only for tumor control in unilateral ANs with hearing loss but also for hearing preservation in those without hearing loss.
 XML Download
XML Download