

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Sepsis is characterized by increased circulating levels of catecholamine, which may cause deleterious effects in the cardiovascular system and inflammatory response.1 Tachycardia reduces the diastolic time, which can decrease ventricular filling or coronary blood flow, particularly in the presence of coronary stenosis, although it increases myocardial oxygen consumption.2 Furthermore, it has been suggested that tachycardia is associated with an increased incidence of major cardiac events and mortality and the use of beta-blocker may improve the mortality in critically ill patients.3456 The heart rate, on the other hand, can influence oxygen delivery, which is a factor in determining cardiac output.7 An increase in heart rate may serve as a compensatory process to maintain cellular metabolic demands in patients with inadequate tissue perfusion. Therefore, it is necessary to evaluate whether the effect of tachycardia varies according to the degree of tissue perfusion, but data on this are still scarce. Our study aimed to evaluate the association of tachycardia on mortality among patients with septic shock according to the serum lactate level, which was used as a marker of tissue perfusion.
METHODS
Study design and population
We analyzed prospectively collected data from 19 tertiary referral or university-affiliated hospitals in South Korea between September 2019 and December 2020 as part of an ongoing nationwide, multicenter observational cohort (the Korean Sepsis Alliance registry). The protocols for patient enrollment and data collection have been described previously.8 All consecutive patients who presented to the emergency department or hospitalized patients in wards who were managed by a rapid response team were screened for eligibility, and patients aged ≥ 19 years diagnosed with sepsis based on the third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3)9 were included in the registry.
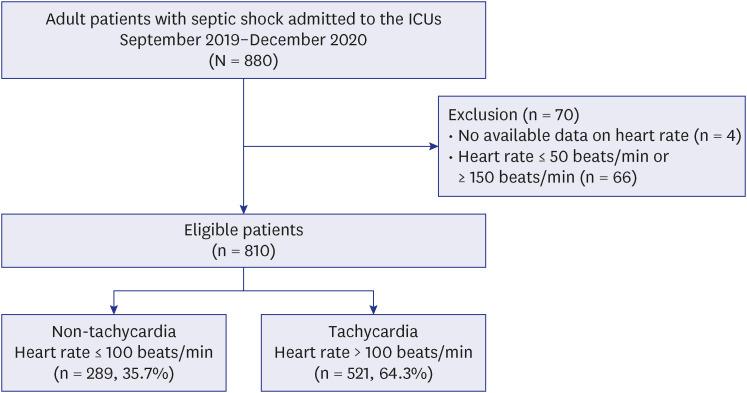
To address the primary research objective of evaluating the effect of tachycardia in patients with shock, only the patients with septic shock who were admitted to the intensive care unit (ICU) were included in the primary analysis. Patients with missing data on heart rate were excluded. In addition, we excluded those with a heart rate of < 50 or > 150 beats/min, which could lead to a decrease in cardiac output, since our interest was to evaluate the role of heart rate as a compensatory mechanism in septic shock.10 Finally, the eligible patients with septic shock were categorized into the tachycardia (heart rate > 100 beats/min) and non-tachycardia (heart rates ≤ 100 beats/min) groups based on the initial heart rate at the time of diagnosis of septic shock.
Diagnosis and management of sepsis
After screening patients with suspected infection using the quick Sequential Organ Failure Assessment (SOFA) score,9 a patient was diagnosed with sepsis if the following two criteria were met: probable or confirmed diagnosis of infection and a change in the total SOFA score of ≥ 2 following infection. Septic shock was defined as persistent arterial hypotension requiring a vasopressor to maintain a mean arterial pressure (MAP) of ≥ 65 mmHg and a serum lactate level of > 2 mmol/L, despite adequate volume resuscitation.9 The decision on management was left to the judgment of each physician in charge without a specific study protocol; however, participating centers provided education program on managing sepsis, including the surviving sepsis campaign guidelines and 1-Hour Surviving Sepsis Campaign bundle to the medical staff.11
Data collection
Data were prospectively collected by trained study coordinators in each participating center using an electronic case report form (http://sepsis.crf.kr/). The patients were followed after enrollment until death or hospital discharge. We collected the following data for all eligible patients: 1) demographic and infection data, including age, sex, comorbidities, SOFA score, physiological and laboratory measurements during enrollment, source and type of infection, and identified pathogens; 2) treatment data, including achievement of the 1-Hour Surviving Sepsis Campaign bundle consisting of measuring the lactate level, obtaining blood cultures prior to the administration of antibiotics, administration of broad-spectrum antibiotics, starting the rapid administration of 30 mL/kg of intravenous crystalloid fluid, application of vasopressors to maintain a MAP ≥ 65 mmHg, and re-measuring the lactate level if the initial lactate level is > 2 mmol/L, choice and appropriateness of empiric therapy, and nonsurgical or surgical source control measures; and 3) clinical outcomes, including ICU and hospital deaths, ICU and hospital lengths of stay, and need for organ support treatment, were collected. To ensure the quality of the data, regular audits were conducted by the research committee members, and each site was provided with data feedback weekly from the committee.
Statistical analyses
Descriptive statistics were performed to compare the characteristics and clinical outcomes between the tachycardia and non-tachycardia groups. Continuous variables were expressed as medians and interquartile ranges (25th and 75th percentiles) and were compared with a Mann-Whitney U test. Categorical variables were summarized with numbers and percentages and were analyzed using χ2 tests or Fisher’s exact tests, where applicable.
A subpopulation treatment effect pattern plot analysis was performed to assess the interaction between tachycardia and lactate levels and to determine the clinical relevant cutoff point of lactate to be used to dichotomize the study population into low and high lactate level groups.1213 Then, logistic regression models were used to adjust for potential confounding factors in the association between tachycardia and hospital mortality. The multivariable model was adjusted for all variables with a P value < 0.1 on the univariate analyses, as well as priori variables that were clinically relevant. The results are reported as odds ratio (OR) of each variable with 95% confidence interval (CI).
For a sensitivity analysis, even after multivariable logistic regression analyses, we performed propensity score-matched analysis to reduce the effects of possible confounding factors as much as possible.14 Propensity scores were estimated using a logistic regression model with patients’ clinical and treatment characteristics. The patients were matched 1:1 based on the propensity scores by nearest-neighbor matching without replacement.15
For all analyses, a two-tailed test with a P value of < 0.05 was considered statistically significant. Statistical analyses were performed using STATA (version 16.0; Stata Corp., College Station, TX, USA).
Ethics statement
The study was approved by the Institutional Review Boards of each participating hospital, including Samsung Medical Center (approval No. 2018-05-108), and the requirement for obtaining patient informed consent was waived because of the observational nature of the study. Additionally, the patients’ information was anonymized and de-identified prior to analysis. This study was reported following the Strengthening the Reporting of Observational Studies in Epidemiology guidelines for observational cohort studies.16
RESULTS
Among the 880 patients with septic shock admitted to the ICU during the study period, 4 patients without available data on heart rate and 66 patients with a heart rate of < 50 or > 150 beats/min were excluded (Fig. 1). Of the 810 eligible patients, 521 (64.3%) had tachycardia at the time of diagnosis of septic shock.
Patient characteristics
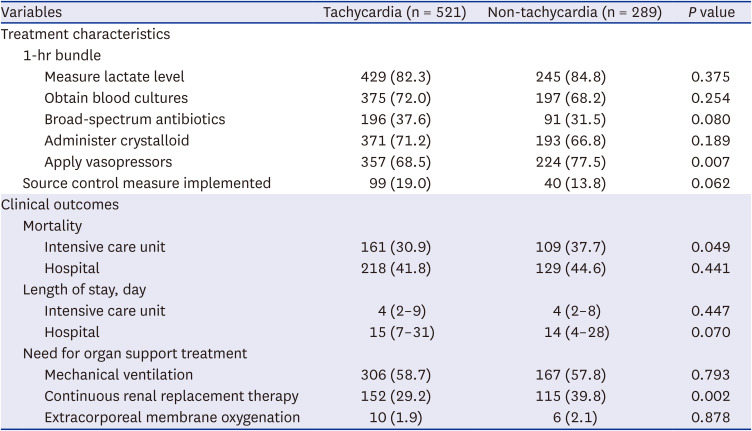
The baseline characteristics of the tachycardia and non-tachycardia groups are compared in Table 1. The tachycardia group was younger and had a lower proportion of chronic neurological disease than the non-tachycardia group. In the initial vital signs, the mean blood pressure (61 vs. 58 mmHg, P = 0.001), respiratory rate (24 vs. 22 breaths/min, P < 0.001), and body temperature (37.5°C vs. 36.6°C, P < 0.001), in addition to the heart rate (120 vs. 86 beats/min, P < 0.001), were higher in the tachycardia group than in the non-tachycardia group. The SOFA scores in the tachycardia and non-tachycardia groups were 8 and 9 (P = 0.042), respectively. In both groups, the respiratory, gastrointestinal, and urinary tracts were common sites of infection; approximately half of the cases were community-acquired infections. There was no significant difference in the initial treatment between the two groups, except for the use of vasopressor within the first hour (77.5% vs. 68.5%, P = 0.007) (Table 2).
Table 1
Baseline patient characteristics
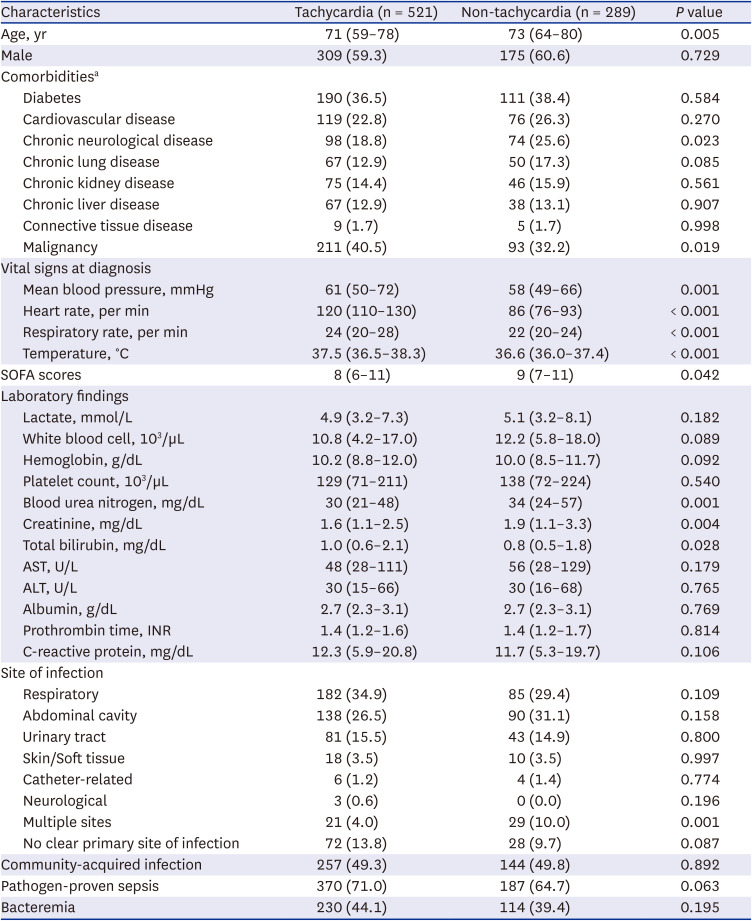
Values are median with interquartile range or number (%).
ALT = alanine aminotransferase, AST = aspartate aminotransferase, SOFA = Sequential Organ Failure Assessment.
aCardiovascular disease includes ischemic heart disease and heart failure; chronic neurological disease includes stroke, neuromuscular disease, epilepsy, and movement disorder; chronic lung disease includes chronic obstructive pulmonary disease, asthma, bronchiectasis, interstitial lung disease, pulmonary tuberculosis, post-tuberculosis related lung disease and non-tuberculous mycobacterium lung disease; chronic kidney disease includes renal impairment lasting more than 3 months (glomerular filtration rate less than 60 mL/min/1.73 m2); chronic liver disease includes liver disease lasting more than 6 months, but does not include hepatocellular carcinoma; malignancy includes solid tumor and hematological malignancy (leukemia, lymphoma, and multiple myeloma).
Table 2
Treatments and clinical outcomes
Clinical outcomes
Overall, 270 (33.3%) and 77 (15.1%) patients died in the ICU and hospitalized in other wards, respectively (Table 2). There was no statistically significant difference in the hospital mortality rate between the two groups (44.6% vs. 41.8%, P = 0.441). Tachycardia was not associated with hospital mortality in the multivariable logistic regression analysis (adjusted OR, 0.86, 95% CI, 0.61–1.22, P = 0.402) (Table 3). Although the tachycardia group was less likely to receive renal replacement therapy than the non-tachycardia group (29.2% vs. 39.8%, P = 0.002), the need for mechanical ventilation or extracorporeal membrane oxygenation support were similar in the two groups. There was no difference in ICU and hospital length of stay between the two groups.
Table 3
Associations of tachycardia with hospital mortality after adjustments for potential confounding factors

| Tachycardia | Variables in the equation | ||||
|---|---|---|---|---|---|
| Coefficient | SE | P value | OR | 95% CI | |
| Crude state | −0.11 | 0.15 | 0.441 | 0.89 | 0.67–1.19 |
| Adjusted statea | −0.15 | 0.18 | 0.402 | 0.86 | 0.61–1.22 |
SE = standard error, OR = odds ratio, CI = confidence interval.
aAdjusted for diabetes, chronic neurological disease, solid tumor/hematological malignancies, mean blood pressure, respiratory rate, Sequential Organ Failure Assessment score, white blood cell, hemoglobin, albumin, prothrombin time, site of infection, community-acquired infection, pathogen-proven sepsis, administer crystalloid, and apply vasopressors.
Effect of tachycardia on hospital mortality according to lactate level
The subpopulation treatment effect pattern plot shows the different effects of tachycardia on hospital mortality across subpopulations stratified according to the blood lactate level (Fig. 2). Among the patients with a lactate level of ≥ 5.3 mmol/L, the tachycardia group had significantly a lower hospital mortality rate than the non-tachycardia group (48.7% vs. 60.3%, P = 0.030) (Fig. 3, Supplementary Table 1). However, there was no statistical difference in the mortality rate between the two groups in patients with a lactate level of < 5.3 mmol/L (36.5% vs. 29.7%, P = 0.156). Logistic regression analysis revealed that tachycardia was independently associated with a reduced hospital mortality rate only in patients with a lactate level of ≥ 5.3 mmol/L (OR, 0.63, adjusted OR, 0.59, 95% CI, 0.35–0.99, P = 0.045), but not in patients with a lactate level of < 5.3 mmol/L (OR, 1.36, adjusted OR, 1.39, 95% CI, 0.82–2.35, P = 0.227) (Table 4). When comparing the initial and follow-up lactate levels between the two groups, there was no significant difference in patients with a lactate level of < 5.3 mmol/L. However, in patients with a lactate level of ≥ 5.3 mmol/L, there was no difference in the initial lactate level, but the follow-up lactate levels were significantly lower in the tachycardia group compared to the non-tachycardia group (Supplementary Table 2).
Fig. 2
Subpopulation treatment effect pattern plot. A subpopulation treatment effect pattern plot of (A) the hospital mortality of patients with or without tachycardia according to subpopulations stratified according to the serum lactate level and (B) the differences in hospital mortality rate between patients with and without tachycardia according to subpopulations stratified according to the serum lactate level.
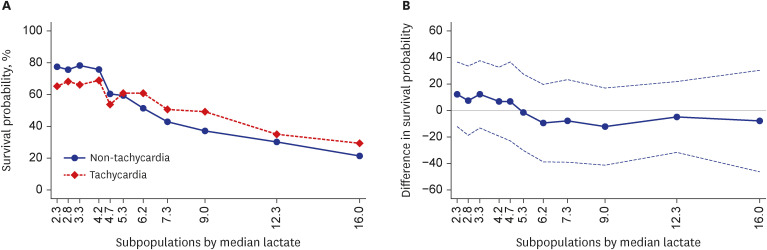
Fig. 3
Hospital mortality according to the lactate level. The hospital mortality rate of the non-tachycardia (blue bar) and tachycardia (red bar) groups according to the lactate level in the (A) overall patients and (B) propensity-matched patients.
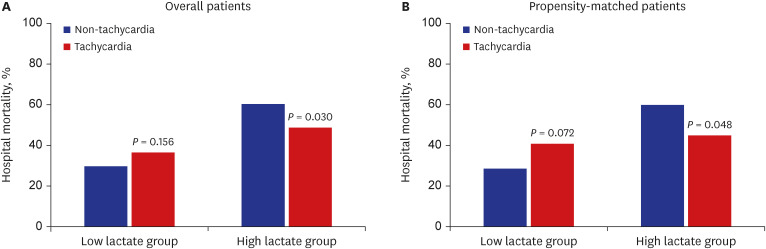
Table 4
Associations of tachycardia with hospital mortality after adjustments for potential confounding factors according to the lactate level
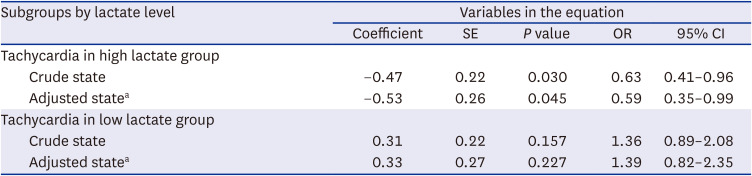
SE = standard error, OR = odds ratio, CI = confidence interval.
aAdjusted for diabetes, chronic neurological disease, solid tumor/hematological malignancies, mean blood pressure, respiratory rate, Sequential Organ Failure Assessment score, white blood cell, hemoglobin, albumin, prothrombin time, site of infection, community-acquired infection, pathogen-proven sepsis, administer crystalloid, and apply vasopressors.
Sensitivity analysis
After propensity score matching, 185 patients in the tachycardia group were matched to 185 patients in the non-tachycardia group. The baseline characteristics of all cases are summarized in Supplementary Table 3. Among the propensity score-matched patients, hospital mortality was similar between the two groups (43.2% vs. 42.7%, P = 0.916). In the subgroups stratified according to the lactate level, tachycardia was associated with reduced hospital morality in patients with a lactate level of ≥ 5.3 mmol/L (44.8% vs. 59.8%; adjusted OR, 0.45, 95% CI, 0.22–0.92, P = 0.028) (Fig. 2, Supplementary Table 4). On the other hand, tachycardia was associated with increased odds of hospital death in patients with a lactate level of < 5.3 mmol/L (adjusted OR, 2.74, 95% CI, 1.30–5.77, P = 0.008).
DISCUSSION
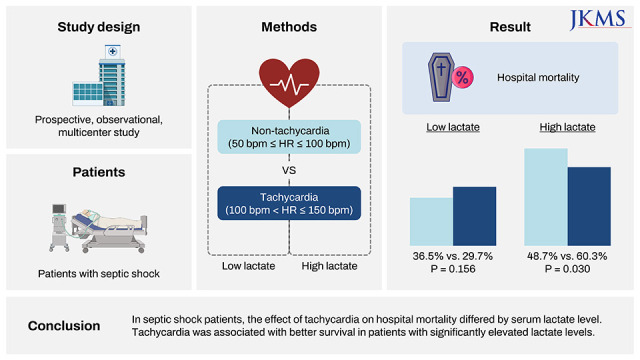
Using the prospective sepsis registry data by the Korean Sepsis Alliance, we investigated the effect of tachycardia on hospital mortality in patients with septic shock according to the serum lactate level. Our findings suggest that the effect of tachycardia might be different according to the degree of lactate elevation; as compared to patients without tachycardia, patients with tachycardia and a significantly elevated lactate level had a better prognosis, whereas patients with tachycardia and a mildly to moderately elevated lactate level tended to have a poorer prognosis.
During septic shock, the circulating fluid volume decreases due to reduced systemic vascular resistance and increased capillary permeability, and in some cases myocardial contractility is also depressed.17 These hemodynamic changes result in reduced cardiac output and impaired oxygen delivery to tissues. In general, in circulatory shock, the sympathetic nervous activity increases to maintain homeostasis of the cardiovascular system, resulting in an increase in heart rates. However, tachycardia can occur in sepsis due to autonomic dysfunction, characterized by excessive sympathoadrenal activation and desensitization of adrenergic receptors, not as part of a compensatory mechanism.1819 A hyperadrenergic state can cause myocardial dysfunction and can also have deleterious effects on the non-cardiovascular systems, such as promotion of catabolic state, acceleration of thrombus formation, and inhibition of the immune system.20 Therefore, despite being a compensatory response to circulatory shock, tachycardia has been suggested as an independent risk factor for poor outcomes in critically ill patients, including sepsis and septic shock. Sander et al.3 have found a higher incidence of major cardiac events during ICU stay in patients with a heart rate > 95 beats/min for > 12 hours, as compared to those who did not, among critically ill patients with a high risk of cardiac complications. Hoke et al.21 identified that a heart rate > 90 beats/min at the time of diagnosis of multiple organ dysfunction was associated with an increased 28-day mortality in critically ill patients, including 43% of patients with severe sepsis and septic shock.
Beta-blockade therapy targeting heart rate reduction was attempted to reduce these adverse effects and it improved the cardiac efficiency, microcirculation, and metabolic function in animal and human studies.222324 Furthermore, the infusion of esmolol, a short-acting beta-blocker, targeting a heart rate of 80–94 beats/min showed significant survival benefits in patients with septic shock with a heart rate of ≥ 95 beats/min after 24 hours of preload optimization.4 Despite the promising findings, however, subsequent studies have shown controversial results. In the J-Land 3S study, landiolol, an ultra-short-acting beta-blocker, was administered to patients with sepsis requiring catecholamine for at least 1 hour and the heart rate of ≥ 100 beats/min was maintained for at least 10 minutes.6 Landiolol reduced the incidence of new-onset arrhythmia, but it did not improve the severity of organ failure as assessed by using the SOFA score and 28-day mortality risk. Levy et al.25 administered esmolol to septic shock patients receiving norepinephrine for at least 6 hours with a heart rate > 100 beats/min and showed that blood pressure and cardiac index decreased without significant deterioration of tissue perfusion. However, in 3 of 9 patients included in this study, esmolol was discontinued early due to marked norepinephrine requirements and persistent cardiac failure.
Differences in the effect of beta-blockers on survival in sepsis may be related to whether tachycardia is compensatory or non-compensatory for the patient’s hemodynamic status. Previous studies on the use of beta-blockers in septic shock defined an optimal hemodynamic status based on the values of the cardiac index and central venous pressure/pulmonary artery occlusion pressure.42324 Monitoring of hemodynamic parameters and correcting derangement are important to improve tissue hypoperfusion in patients with shock; however, hemodynamic parameters within the normal range do not guarantee adequacy of tissue perfusion.26 In our study, the higher survival rates of patients with tachycardia in the subgroup with high lactate levels support that tachycardia in this subgroup is compensatory rather than non-compensatory. Patients who do not have increased heart rate due to sepsis may not be adequate to restore tissue perfusion.27 Our findings suggest that lactate level may have a role in assessing the adequacy of the heart rate in patients with septic shock. In other words, the decision to lower the heart rate using beta-blockers in patients with high lactate levels should be made carefully, even in cases wherein the hemodynamic parameters are within the normal range.
Although this study is the first to provide information on the interaction between the heart rate and lactate level in septic shock using a multicenter cohort study, several limitations should be noted. First, the significance of our findings might have been influenced by the inherent selection bias of this observational study. Although this was addressed by adjusted multivariate analysis and propensity score matching, the potential for bias due to an unmeasured risk factor remains. However, the data were prospectively collected from all consecutive patients diagnosed with sepsis from 19 hospitals in Korea, improving the generalizability of our findings. Nonetheless, there was a potential for selection bias because only tertiary or university-affiliated hospitals were included in the study. Second, previous studies demonstrated that arrhythmia and the presence of diastolic or right ventricular dysfunction, are associated with poor outcomes in patients with sepsis282930; unfortunately, we did not analyze these factors. In addition, we defined tachycardia using only the heart rate measured at the time of diagnosis of septic shock. Therefore, the effect of changes in heart rate while managing septic shock on clinical outcomes could not be evaluated. Third, because we did not obtain data on the changes in hemodynamic parameters such as central venous pressure, stroke volume, or cardiac output in both groups, the interpretation of the causal relationship between tachycardia and hospital mortality from our study findings is limited. In addition, we have not obtain data on factors that may affect heart rate such as drugs or volume status. Further research is needed to better understand the influence of tachycardia on mortality in septic shock.
In conclusion, the effect of tachycardia on hospital mortality differed according to the serum lactate level. In particular, tachycardia was associated with better outcomes in patients with high lactate levels. Further studies should be conducted to evaluate the pathophysiology of tachycardia in patients with septic shock and to develop specific therapeutic strategies to improve the outcome of these patients.
 XML Download
XML Download