

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) created enormous social problems over the 3 years of the pandemic. Globally, nonpharmacological interventions (NPIs) including mask-wearing, hand-washing, and physical distancing reduced viral transmission, but compromised personal relationships and brought social systems to a standstill.12
The Korean health authorities implemented nationwide NPIs to prevent the spread of SARS-CoV-2 from infected to susceptible persons. Classes moved online and daycare centers and schools were closed for 3 years according to nationwide social distancing guidelines based on the number of new COVID-19 confirmed cases.3456 On 20 November 2021, infections had greatly dwindled, and all schools resumed full-time in-person classes. The Korean government lifted all social distancing rules on 18 April 2022.7
Respiratory virus infections in young children are epidemiologically important. Children could transmit viruses to other family members, including older adults, thereby conferring herd immunity.89101112 Therefore, prevention of pediatric respiratory infections may reduce disease transmission within a household.
NPIs reduced the incidence of several infectious diseases, but radically affected daily life and compromised mental health. Children gained weight, given the reduction in physical activity when schools closed and the increased child screen time. Parents became depressed and children developed sleep and behavioral problems.1314151617 Thus, it is important to evaluate whether NPIs are absolutely necessary to prevent respiratory infections, especially severe infections, in children.
This study compares epidemiological changes in severe respiratory infections during pre-NPI, NPI, and post-NPI periods in order to evaluate the effect of that NPI on severe respiratory infections in children.
METHODS
Severe Acute Respiratory Infection (SARI) surveillance
The Korean SARIs surveillance system maintains a prospective nationwide database of infected patients that is based on the World Health Organization operational guidelines for sentinel SARI surveillance; the system has been operational at 13 sentinel sites since July 2017.181920
A SARI is defined as hospitalization with an acute respiratory infection, a fever of 38°C or higher on the day of admission or a history of fever within 10 days prior to admission, and respiratory symptoms such as a cough.20 The Korean Disease Control and Prevention Agency manages the database and publishes weekly reports from the 13 sites on occurrences of respiratory syncytial virus (RSV), influenza virus (IFV), human adenovirus (AdV), human parainfluenza virus (HPIV), human rhinovirus (HRV), human metapneumovirus (HMPV), human bocavirus (HBoV), and human coronavirus (HCoV); atypical bacterial pathogens and pneumococci; and clinical information.19 To December 2019, data were collected during only 9 months of the year (excluding June to August). However, since January 2020, data have been collected during all 12 months.19
Study design and population
We retrospectively reviewed all SARI data from January 2018 to October 2022 and extracted cases that met the following criteria: age ≤ 12 years, hospitalization with an acute respiratory infection, a history of fever within the preceding 10 days or a fever ≥ 38°C on the day of admission, and respiratory symptoms such as a cough.
All causative viruses were identified via polymerase chain reaction (PCR). Epidemiological changes were analyzed in the pre-NPI, NPI, and post-NPI periods. In children, physical distancing including school and daycare closures were more protective than other NPIs; children were less likely than adults to wear masks and wash hands. Therefore, the periods were based on the opening and closing times of schools and daycare centers. The pre-NPI period ran from January 2018 to December 2019 and the NPI period from March 2020 to February 2021, including the period when schools were closed. In Korea, NPIs, thus social distancing and school shutdowns, commenced in March 2020. The number of affected schools changed as the social distancing requirements varied; education was both online and offline. On 20 November 2021, all schools resumed full-time in-person classes.7 Therefore, November 2021 to October 2022 served as the post-NPI period (Supplementary Fig. 1).
Statistical analysis
Continuous variables are presented as medians (minima to maxima) and compared via analysis of variance or the Kruskal-Wallis test (as appropriate in terms of the normality of distribution). Categorical variables are presented as percentages and were compared used the chi-squared or Fisher exact test. To explore differences in the numbers of respiratory virus infections over time, we calculated the number of patients per 1,000 hospitalizations by multiplying each ratio by 1,000 and then used the χ2 or Fisher exact test for comparisons. We graphed the proportions of patients with respiratory virus infections in the pre-NPI, NPI, and post-NPI periods. All statistical analyses employed SAS (version 9.4; SAS Institute, Cary, NC, USA) and R version 4.1.3 (R Foundation, Vienna, Austria). All reported P values are two-sided, and values < 0.05 were considered statistically significant.
Ethics statement
This study was approved by the Institutional Review Board (IRB) of Korea University Guro Hospital (approval No. K2022-1592-002) and adhered strictly to all relevant principles of the Declaration of Helsinki. Patient privacy and anonymity were guaranteed. The need for written informed consent was waived by the IRB.
RESULTS
Clinical characteristics
A total of 86,390 pediatric patients were admitted during the 2-year pre-NPI period, 39,366 during the 1-year NPI period, and 40,632 during the 1-year post-NPI period. Of these, 9,631 (11.1%) were admitted with SARIs during the pre-NPI period, 579 (1.5%) during the NPI period, and 1,580 (3.9%) during the post-NPI period (Fig. 1).
Fig. 1
Flow chart of enrolled patients.
NPI = nonpharmacological intervention, SARI = Severe Acute Respiratory Infection.
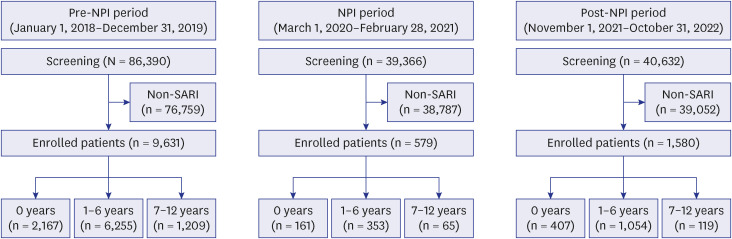
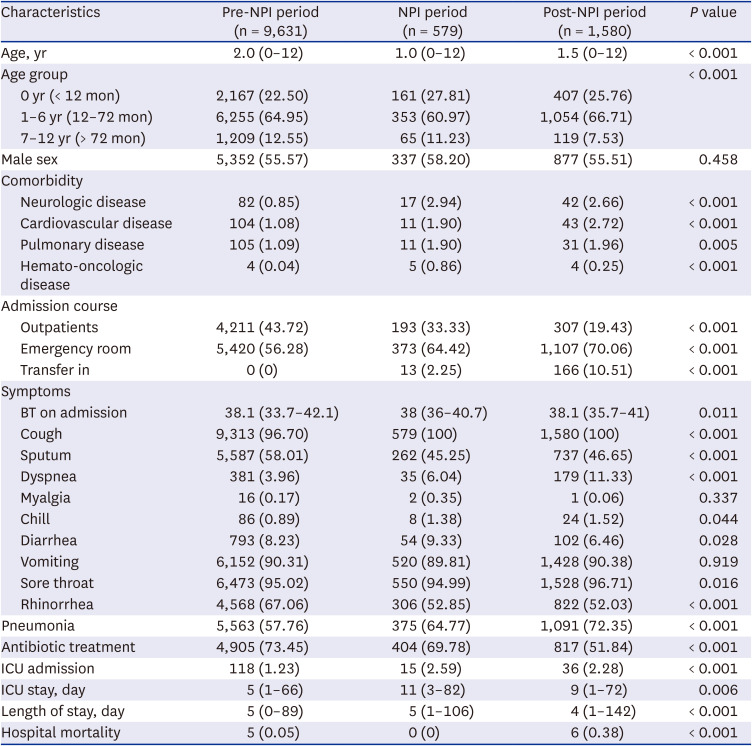
Table 1 lists the demographics of all pediatric patients. The median age during the NPI period was younger than before and after that period, and the proportion of patients younger than 12 months higher in the NPI than in the other periods. However, the proportions of the sexes did not differ in any period. During the NPI period, the proportion of patients with comorbidities was higher than during the other periods, and most patients were admitted via emergency rooms. The proportion of intensive care unit (ICU) admissions was higher in the NPI and post-NPI periods than in the pre-NPI period, and the lengths of ICU stay longer than in the pre-NPI period (Table 1).
Table 1
Clinical characteristics in this study
Number of SARI patients per 1,000 admitted patients and SARI-positive test rates
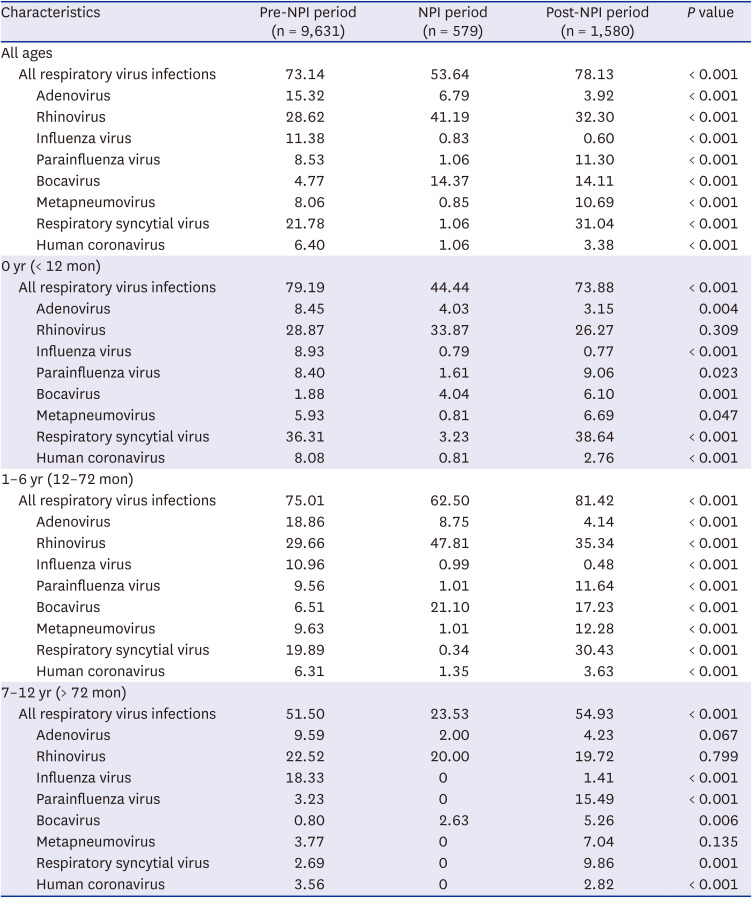
Table 2 lists the changes in the number of SARIs per 1,000 hospitalized patients by age group. During the NPI period, the number of patients with respiratory virus infections decreased dramatically, from 72.1 per 1,000 admitted patients to 6.6 per 1,000. During the post-NPI period, 22.8 per 1,000 admitted patients were treated for SARIs. This trend was consistent across all age groups and for almost all respiratory viruses (not IFV). In the post-NPI period, the incidence of infections with encapsulated viruses such as HPIV, HMPV, and RSV increased, but the incidence of IFV had not increased as of October 2022. The positive test rates were lower in the NPI than in the pre-NPI period. However, in the post-NPI period, the positive test rates recovered to the levels noted before COVID-19 (Table 3).
Table 2
Changes in the number of severe acute respiratory virus infections per 1,000 hospitalized patients by age group
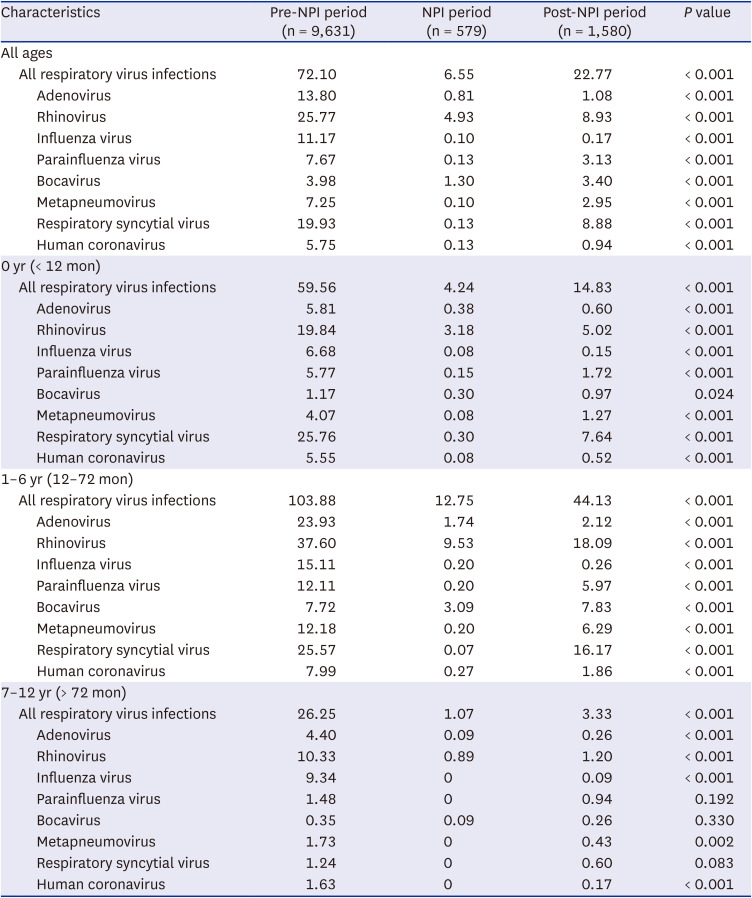
Table 3
Changes in the test positive rate (%) of each respiratory virus in the pre-NPI period, NPI period, and post-NPI period
Distributions of age and clinical characteristics
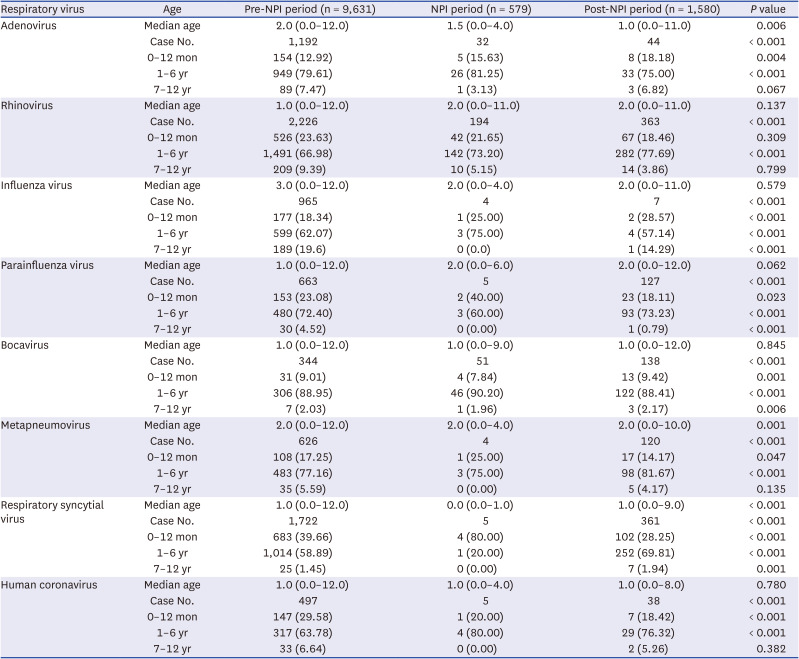
The median age of patients infected with AdV in the post-NPI period was lower than that in the pre-NPI period. The ages of patients infected with HRV, HPIV, HCoV, or HMPV did not change between 2018 and 2022. The proportion of RSV-infected children younger than 1 year decreased over time, from 39.7% in the pre-NPI period to 28.3% in the post-NPI period, but the proportion of RSV patients aged 1–6 years increased from 58.9% to 69.8% (Table 4).
Table 4
Distributions of age and clinical characteristics in children with viral respiratory infections
Trends in pediatric respiratory infections requiring hospitalization
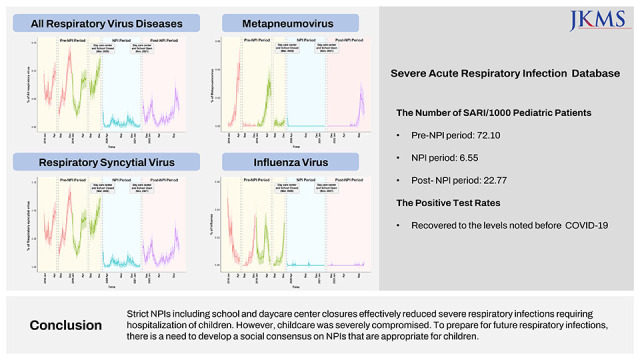
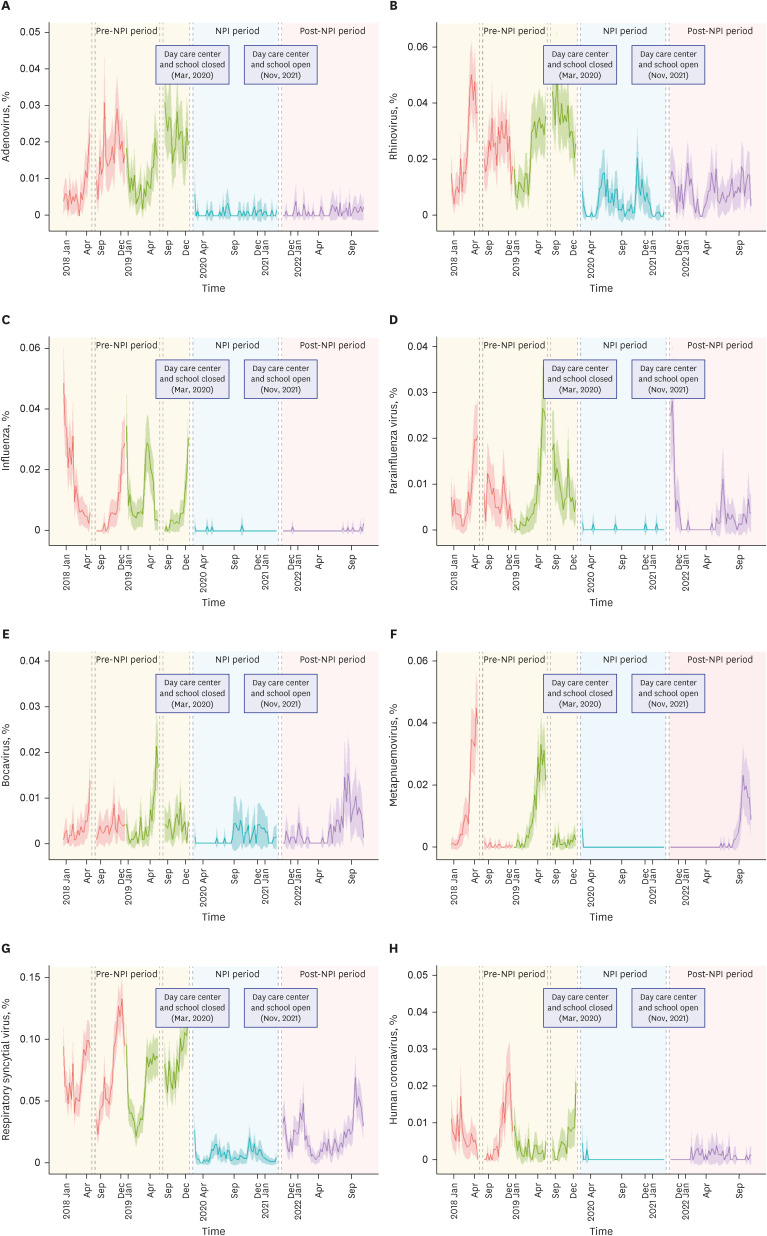
Fig. 2 shows the proportions of patients with all SARIs relative to total hospitalizations in the pre-NPI, NPI, and post-NPI periods. Fig. 3 shows the proportions with individual virus infections. During the NPI period, the incidence of most viruses decreased and then increased slowly during the post-NPI period. The incidence rates of HCoV, HMPV, RSV, and IFV infections decreased dramatically during the NPI period, becoming near-zero by the end of 2020. However, the incidence rates of HBoV and HRV did not markedly decrease. In contrast, the HBoV incidence increased from the autumn to winter of the NPI, compared to the pre-NPI period. During the post-NPI period, the proportion of patients with respiratory viruses among all hospitalized patients increased for all viruses except IFV. The HPIV graphs show outbreaks in November and December of 2021 and a high frequency of infection after June 2022, compared to that in the summer before the NPI period. We observed a high frequency of HMPV infection in October 2022 but no IFV outbreak before that time.
Fig. 2
Epidemic proportion curves (95% confidence intervals) for severe acute respiratory virus infection relative to total hospitalization in the pre-NPI period, NPI period, and post-NPI period.
NPI = nonpharmacological intervention.
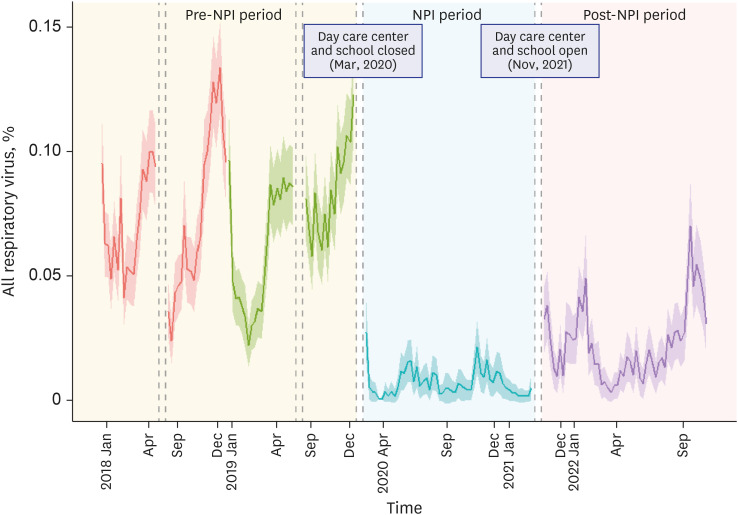
Fig. 3
Epidemic proportion curves (95% confidence intervals) for each respiratory virus infection relative to total hospitalization in the pre-NPI period, NPI period, and post-NPI period. (A) Adenovirus. (B) Rhinovirus. (C) Influenza virus. (D) Parainfluenza virus. (E) Bocavirus. (F) Metapneumovirus. (G) Respiratory syncytial virus. (H) Human coronavirus.
NPI = nonpharmacological intervention.
DISCUSSION
This study focused on epidemiological changes in severe respiratory infections of Korean children requiring hospitalization over the pre-NPI, NPI, and post-NPI periods. During the NPI period, the number of such patients decreased dramatically, from 72.1 per 1,000 hospitalizations to 6.6 per 1,000. However, after NPIs ceased, the number gradually increased to 22.8 per 1,000. In the post-NPI period, the positive test rates recovered to the pre-NPI levels. Thus, the NPI strategies including school and daycare center closures effectively controlled severe respiratory infections requiring hospitalization in pediatric patients.
The emergence of COVID-19 has been life-changing, and has profoundly affected the epidemiology of other respiratory infections. Such infections plummeted when physical distancing, including lockdowns, was mandated.21222324 Our data are in line with those of other studies conducted during the NPI period. After physical distancing ceased, respiratory infections gradually increased worldwide.252627 However, few studies have been conducted on severe respiratory infections requiring hospitalization in pediatric patients.
We found that infections with HRV and HBoV (both non-enveloped viruses) persisted over the entire study period, including the NPI period; however, enveloped viral infections, especially HPIV, HMPV, and RSV infections, increased after physical distancing ceased (Fig. 3). HPIV outbreaks occurred in November and December of 2021, June to July 2022 and September to October 2022, RSV outbreaks from December 2021 to March 2022 and September to October 2022, and HMPV infections in October 2022.
The detection rates of non-enveloped viruses (HRV, HBoV, and AdV) did not change during the pandemic. Indeed, the detection rate of HRV in children younger than 6 years increased, compared to that in the pre-NPI era, perhaps because this non-enveloped virus is resistant to environmental challenges and exhibits a long shedding time in children.
During the post-NPI period (to October 2022), the number of children admitted with IFV infections was 0.17 per 1,000 patients; in the pre-NPI period, the figure was 11.17 per 1,000. During the 2020–2022 seasons, we found no influenza outbreak in Korea. The disappearance of such outbreaks for two consecutive seasons despite the cessation of NPIs indicates that the origins of such outbreaks are not domestic. International travel restrictions eliminated virus import.28 The incubation period (1–4 days) and duration of shedding (5–10 days) for IFV are shorter than those for SARS-CoV-2.293031 Therefore, IFV influx was rendered impossible by the 1–2 weeks of quarantine and symptom monitoring imposed on travelers. However, H3N2 IFV outbreaks were reported in the USA. Currently, overseas travel regulations have eased and quarantine obligations lifted; an IFV influx from abroad and a domestic outbreak are expected.323334
The proportion of RSV-infected children younger than 1 year decreased by 39.7% after the pandemic. A recent study also found that the age of children with community-acquired pneumonia was higher during the NPI than in the pre-NPI period. Most children are infected more than once with respiratory viruses such as RSV before the age of 2 years. Korean infants born since the emergence of COVID-19 have encountered many fewer respiratory viruses since birth than have children born earlier. Thus, the preschoolers of today may lack substantial immunity against respiratory viruses. Such virus-naïve children who started attending daycare centers in the post-NPI period are likely to have contributed to the marked resurgences observed.30
The proportion of patients with dyspnea requiring ICU admission increased during the NPI and post-NPI periods, compared to the pre-NPI period; thus, the severity of respiratory virus infections increased in pediatric patients. During the pandemic, parents may have been more reluctant to take children to hospital than before the pandemic because they were concerned that children could be infected with COVID-19 in hospital. In other words, children presenting to emergency rooms tended to be seriously ill. However, changes in the severity of infectious diseases during and after the pandemic have been but little studied. Further work should explore changes in the severity of respiratory viral infections among pediatric patients before, during, and after the pandemic.
Our work had several potential limitations. First, all patient ages were recorded in years (not months). Data on children younger than 12 months were thus not analyzed in detail. Second, we lacked information on virus subtypes and co-infections. Third, as all viruses were diagnosed via PCR, we cannot distinguish true pathogens from non-pathogenic colonizers. Fourth, surveillance bias was in play because the system focused on patients hospitalized with respiratory infections. However, most pediatric patients with respiratory infections recover without complications. Therefore, data on SARIs requiring hospitalization are important when evaluating the effectiveness of NPIs for children. Finally, the detection rate differed by age. The proportions of SARIs were highest among those aged 1–6 years in all study periods. In Korea, children attend daycare or kindergarten at such ages and it is thus challenging to impose NPIs; the children are in close contact. Those aged 1 year are minimally exposed to pathogens because they live at home isolated from other babies, and children aged over 6 years can be protected by NPIs imposed by schools. Despite these limitations, this is the first nationwide study on epidemiological changes in the severe respiratory infections of children requiring hospitalization during pre-NPI, NPI, and post-NPI periods in Korea.
In conclusion, the number of pediatric patients with severe respiratory infections requiring hospitalization decreased dramatically during the NPI period, from 72.1 per 1,000 hospitalizations to 6.6 per 1,000. However, after NPIs ceased, the number gradually increased to 22.8 per 1,000. Strict NPIs including school and daycare center closures effectively reduced severe respiratory infections requiring hospitalization of children. However, childcare was severely compromised. To prepare for future respiratory infections, there is a need to develop a social consensus on NPIs that are appropriate for children.
 XML Download
XML Download