

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cancer is one of the major causes of death, and its burden has been continuously increasing worldwide.123 With curative intention, the most common treatment option for solid cancer is long surgery.4 In 2015, there were 15.2 million new cases of cancer worldwide, over 80% of which required surgery.5 Therefore, the management of patients with cancer who underwent cancer surgery is an important health issue.
Body mass index (BMI) and waist circumference (WC) have been used to evaluate nutritional status and obesity among populations.67 As obesity, overweight, or malnutrition affect clinical outcomes,8 BMI and WC could be used as prognostic factors in the population. Several recent reports have explained the impact of BMI and WC on mortality outcomes.91011 A previous study reported that a lower BMI was associated with a higher risk of mortality, whereas WC and lower BMI were not associated with mortality.11 Another study has reported a linear relationship between WC and all-cause mortality.9 For patients who underwent cancer surgery, a lower BMI was associated with increased postoperative mortality, while a higher BMI was not a significant risk factor for postoperative mortality.121314 However, no study has focused on the impact of preoperative WC and BMI on the mortality of patients who underwent cancer surgery.
This study aimed to examine whether preoperative BMI or WC is associated with mortality after cancer surgery in South Korea.
METHODS
Data source
Data were extracted from the National Health Insurance Service (NHIS) database. As a single public health insurance in South Korea, the NHIS contains and manages data on disease diagnoses and prescriptions for procedures and drugs. Disease diagnoses were registered using the International Classification of Diseases, External 10th Revision (ICD-10 codes). Additionally, the NHIS database contains demographic and socioeconomic status-related information for all patients in South Korea.
Study population
We initially included patients who were admitted to the hospital from January 1, 2016 to December 31, 2020 and underwent major cancer surgery with curative intent. Major cancers included lung, gastric, colorectal, esophageal, small bowel, liver, pancreatic, and bile duct or gallbladder cancers. In South Korea, patients with cancer are registered in the NHIS database to receive financial coverage for treatment expenses. In particular, the government supports most (approximately 95%) of the treatment costs of cancer patients. Among the patients who underwent major cancer surgery, we included those who had undergone standardized health examinations in the year prior to cancer surgery. In South Korea, NHIS subscribers aged ≥ 40 years are recommended to undergo standardized health examinations every two years.15
Preoperative BMI and WC (independent variable)
BMI and WC, which were measured in the year prior to cancer surgery, were obtained from the standardized health examination. Therefore, the average time interval from the date when BMI and WC were measured to the date of surgery was one year. Patients were categorized into five groups according to their BMI: < 18.5, 18.5–24.9, 25.0–29.9, 30.0–34.9, and > 35.0 kg/m2. WC was categorized into three groups (normal, high, and very high). According to a previous study,16 the WC in the normal, high, and very high groups was < 94 cm, 94–101.9 cm, and ≥ 102 cm for men and < 80 cm, 80–87.9 cm, and ≥ 88 cm for women, respectively.
Endpoints
The primary endpoint was 90-day mortality, which was defined as death within 90 days after the date of cancer surgery. The secondary endpoint was 30-day mortality, which was defined as death within 30 days after the date of cancer surgery. The 90-day mortality was determined as the primary endpoint because it reflects mortality from multiple causes, such as complications after surgery, whereas the 30-day mortality reflects surgery-related deaths.17
Covariates
Age and sex were collected as demographic information. Data on employment status, household income level, and residence were collected to reflect the preoperative socioeconomic status of the patients. The NHIS contains data on patients’ household income levels to determine the insurance premiums for the year, and approximately 67% of the medical expenses are subsidized by the government.18 However, individuals from low-income households are enrolled in the Medical Aid Program, wherein the government covers nearly all medical expenses to minimize the financial burden of medical costs. The patients were divided into five groups based on quartile ratios: Q1–Q4 and Medical Aid Program groups. Residences were classified as urban (those residing in Seoul and other metropolitan cities) or rural (those from all other areas). Hospitals in which patients underwent cancer surgery were classified into two groups: tertiary general hospitals and general hospitals. Surgical cases from video-assisted laparoscopic surgery and laparoscopy were collected as covariates. The Charlson comorbidity index was calculated using the ICD-10 codes to determine the comorbidity status of the patients (Supplementary Table 1). All individuals with disabilities must be registered in the NHIS database to receive benefits from South Korea social welfare system. In the database, the patients were divided into six groups according to the severity of their disability. Meanwhile, we divided the patients into two severity groups: patients with grades 1–3 disabilities were assigned to the severe disability group, whereas those with grades 4–6 were assigned to the mild-to-moderate disability group.
Statistical analysis
The clinicopathological characteristics of all patients were presented as median values with interquartile range (IQR) for continuous variables and numbers with percentages for categorical variables. First, the log odds of 30- or 90-day mortality after cancer surgery according to preoperative BMI or WC (continuous variables) were examined using restricted cubic splines (RCSs). Next, we performed univariate analyses for 30- or 90-day mortality after cancer surgery to examine individual association between many covariates and 30- or 90-day mortality. Then, we selected covariates with P values less than 0.1 and included them in the multiple logistic regression analyses in addition to preoperative BMI and WC. The results were presented as odds ratios (ORs) with 95% confidence intervals (CIs). We performed subgroup analyses for 90-day mortality according to the type of cancer surgery to examine whether the type of cancer surgery affected the main results. There was no multicollinearity between variables in the models with the criterion of variance inflation factors < 2.0. All statistical analyses were performed using R software (version 4.0.3; R Foundation for Statistical Computing, Vienna, Austria), and statistical significance was set at P < 0.05.
Ethics statement
This study involved human participants, and all procedures were conducted in accordance with the guidelines provided by the relevant ethics boards. The study protocol was reviewed and approved by the relevant Institutional Review Board (X-2105-686-904) and the NHIS (NHIS-2022-1-336). The requirement for informed consent was waived because data analyses were performed retrospectively using anonymous data derived from the South Korean NHIS database.
RESULTS
Study population
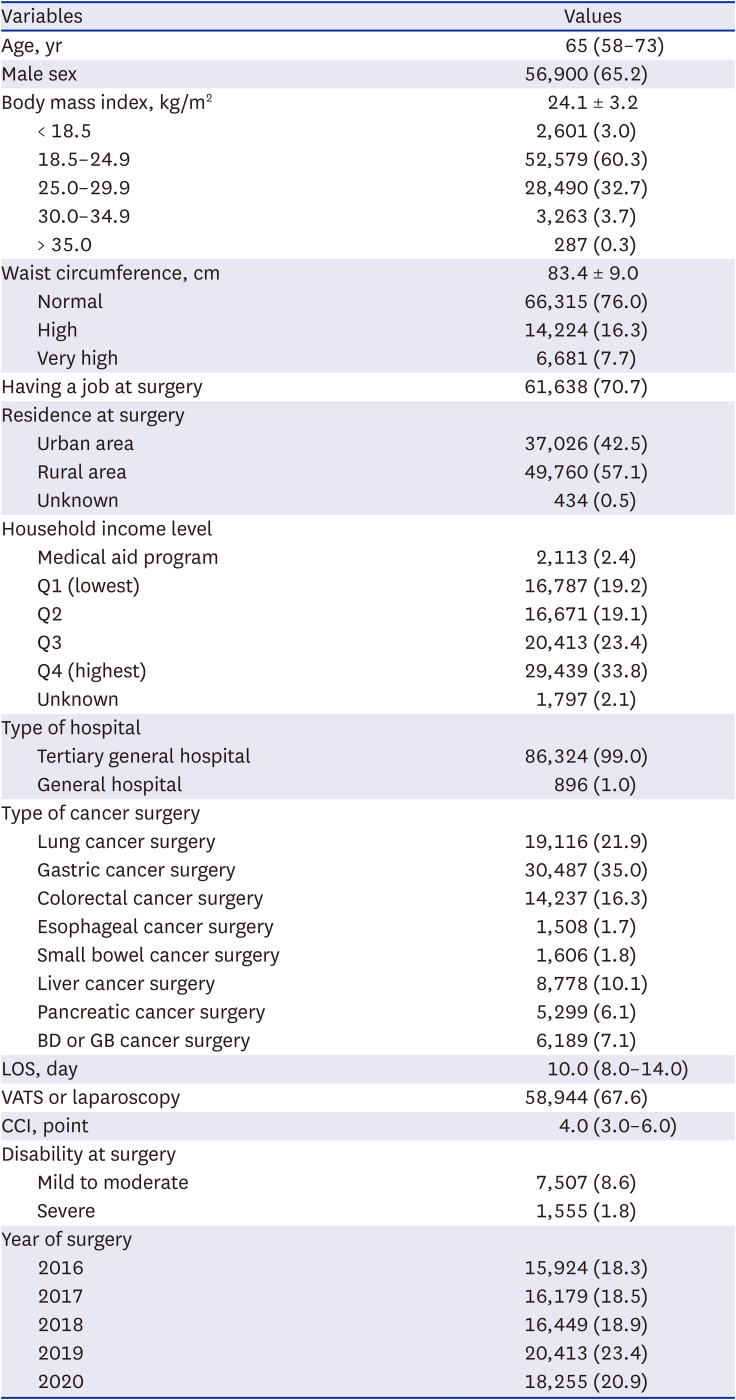
Fig. 1 shows a flowchart depicting the patient selection process in this study. From January 1, 2016 to December 31, 2020, 253,538 patients underwent major cancer surgery with curative intent in South Korea. Among them, 166,311 patients who did not have data regarding standardized health examinations in the year prior to cancer surgery and seven patients who did not have WC data were excluded from the final analysis. Thus, 87,220 patients were included in the final analysis. A total of 454 (0.6%) and 1,374 (1.6%) patients died within 30 days and 90 days after the date of cancer surgery, respectively. Table 1 shows the clinicopathological characteristics of patients. The median age was 65.0 years old (IQR, 58–73 years), and the proportion of males was 65.2% (56,900/87,220).
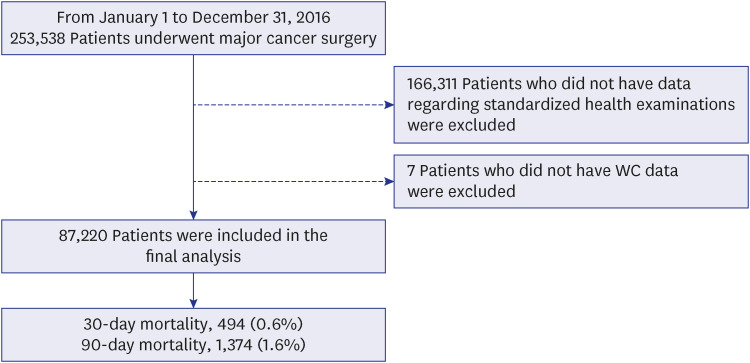
Table 1
Clinicopathological characteristics of patients
RCS
Supplementary Figs. 1 and 2 show the RCS, which represents log odds of 90- or 30-day mortality after cancer surgery according to preoperative BMI or WC. Both the log odds of 90- and 30-day mortality increased with lower BMI. Compared to BMI, WC did not show a significant trend for log odds in both 90- and 30-day mortality.
BMI, WC and mortality
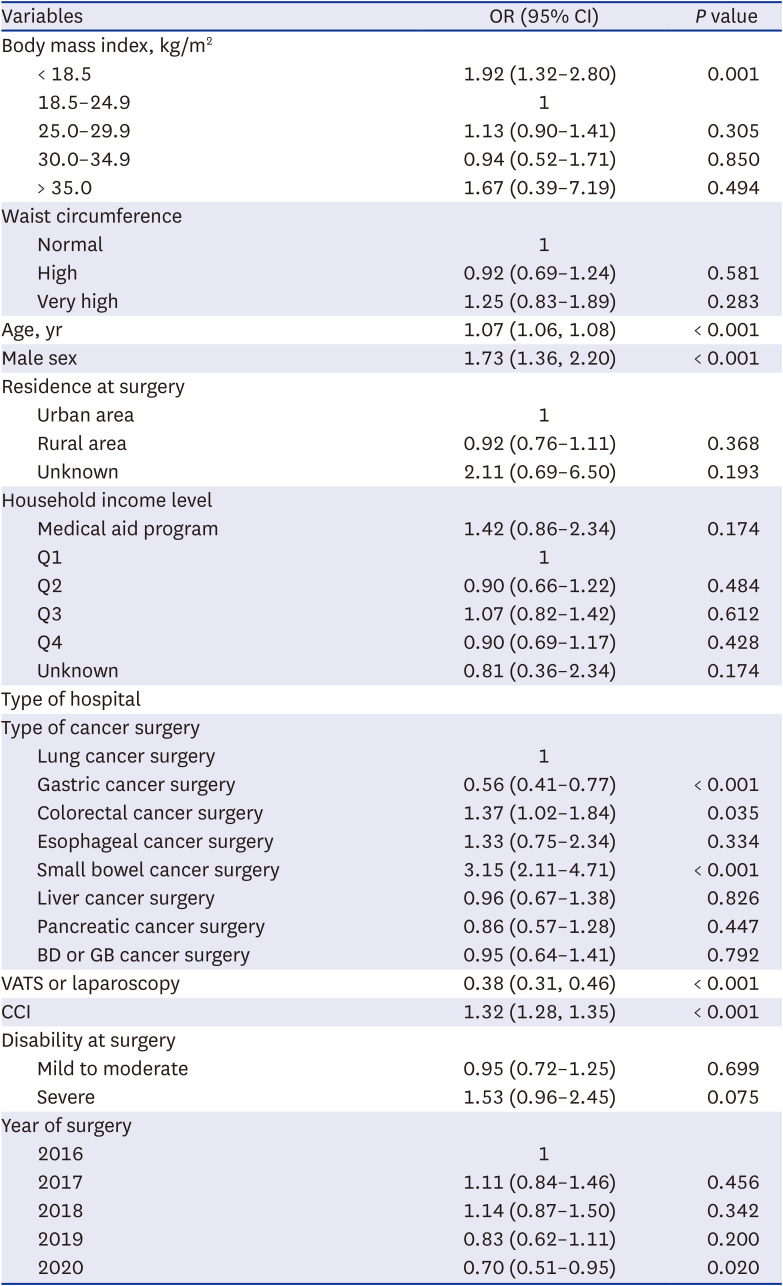
Supplementary Tables 2 and 3 present the results of univariate logistic regression analyses for 90- and 30-day mortality after cancer surgery. Table 2 shows the results of the multiple logistic regression model for 90-day mortality after cancer surgery. Compared to the BMI 18.5–24.9 kg/m2 group, the BMI < 18.5 kg/m2 and > 35 kg/m2 groups show 1.98-fold (OR, 1.98; 95% CI, 1.58–2.49; P < 0.001) and 2.60-fold (OR, 2.60; 95% CI, 1.25–5.40; P < 0.001) higher 90-day mortality after cancer surgery. The BMI 25.0–29.9 kg/m2 (P = 0.144) and 30.0–34.9 kg/m2 (P = 0.105) groups did not show significant differences compared to the BMI 18.5–24.9 kg/m2 group. The high WC group (P = 0.052) and very high WC group (P = 0.232) also did not show significant differences in terms of 90-day mortality compared with the normal WC group. Table 3 shows the results of the multiple logistic regression model for 30-day mortality after cancer surgery. Compared to the BMI 18.5–24.9 kg/m2 group, the BMI < 18.5 kg/m2 group shows 1.92-fold (OR, 1.92; 95% CI, 1.32–2.80; P < 0.001) higher 30-day mortality after cancer surgery. The BMI 25.0–29.9 kg/m2 (P = 0.305), 30.0–34.9 kg/m2 (P = 0.850), and > 35 kg/m2 (P = 0.494) groups did not show significant differences compared to the BMI 18.5–24.9 kg/m2 group. The high (P = 0.581) and very high WC groups also did not show significant differences in terms of 30-day mortality compared with the normal WC group (P = 0.283).
Table 2
Multiple logistic regression model for 90-day mortality after cancer surgery
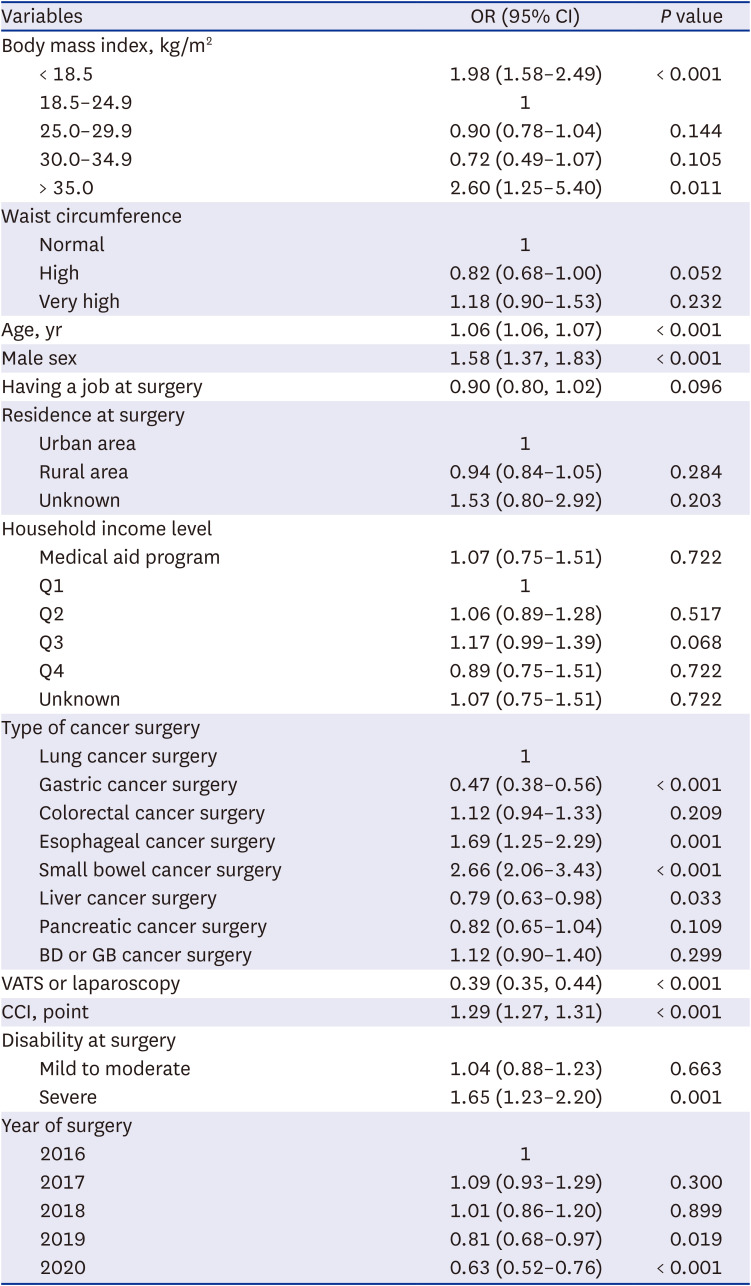
Table 3
Multiple logistic regression model for 30-day mortality after cancer surgery
Subgroup analyses
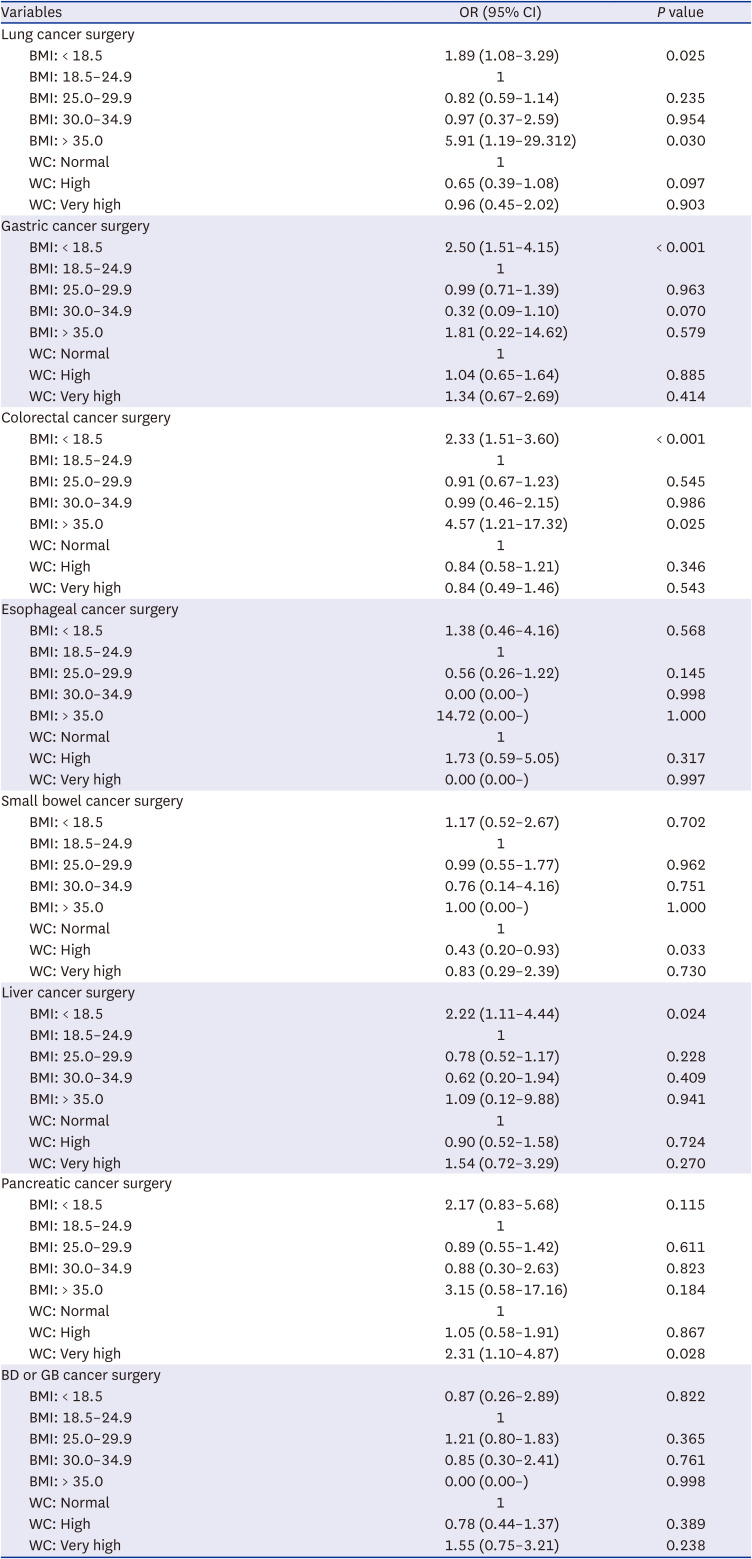
Table 4 shows the results of the subgroup analyses for 90-day mortality according to cancer surgery type. Compared to the BMI 18.5–24.9 kg/m2 group, the BMI < 18.5 kg/m2 group showed higher 90-day mortality after lung (OR, 1.89; 95% CI, 1.08–3.29; P = 0.025), gastric (OR, 2.50; 95% CI, 1.51–4.15; P < 0.001), colorectal (OR, 2.33; 95% CI, 1.51–3.60; P < 0.001), and liver (OR, 2.22; 95% CI, 1.11–4.44; P = 0.024) cancer surgeries. Preoperative WC did not affect the 90-day mortality after all types of cancer surgery (all P > 0.05).
Table 4
Subgroup analyses for 90-day mortality according to cancer surgery type
DISCUSSION
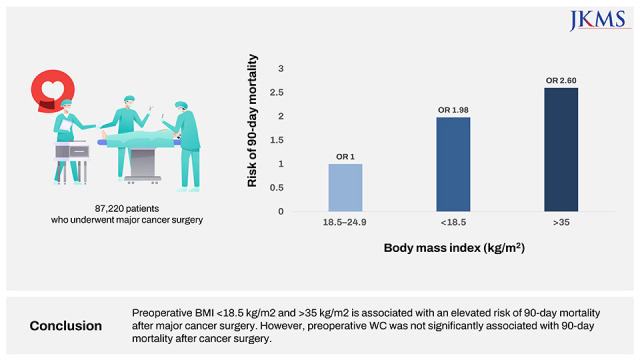
This population-based cohort study showed that a preoperative BMI < 18.5 kg/m2 and > 35 kg/m2 groups has an increased risk of 90-day mortality after major cancer surgery. However, preoperative WC was not significantly associated with the 90-day mortality after cancer surgery. Moreover, this association was more evident in patients who underwent lung, gastric, colorectal, and liver cancer surgeries. Our results suggest that having low or very high preoperative BMI might be risk factors for increased mortality after cancer surgery unlike preoperative WC.
Patients who are underweight, with a BMI < 18.5 kg/m2, were reported as a high-risk group for increased postoperative mortality in several previous studies.121314 Low BMI is a well-known factor reflecting malnutrition; a BMI of 17.0 kg/m2 and 17.8 kg/m2 defines malnutrition for younger and older patients, respectively.19 The BMI < 18.5 kg/m2 used in this study is similar to the value of 17.0–17.8 kg/m2, and reflects preoperative malnutrition in patients who underwent major cancer surgeries. Interestingly, a preoperative BMI < 18.5 kg/m2 was associated with higher 90-day mortality in patients who underwent lung, gastric, colorectal, and liver cancer surgeries. Gastric, colorectal, and liver cancers are important gastrointestinal tract cancers that might have a higher risk for malnutrition than do other types of cancer.20 Preoperative malnutrition is associated with a higher risk of mortality and morbidity after major intra-abdominal, gastric, colorectal, and liver cancer.12131421
A BMI > 35 kg/m2 was associated with a higher risk of 90-day mortality after major cancer surgery. The BMI ≥ 35 kg/m2 group classified as having grades 2 and 3 obesity was associated with significantly higher all-cause mortality, whereas a BMI of 30–35 kg/m2 (grade 1 obesity) was not associated with mortality.22 Moreover, a recent meta-analysis reported that being underweight (BMI < 18.5 kg/m2) or having class II/III obesity (BMI > 35 kg/m2) at the time of colorectal cancer surgery may result in worse long-term survival outcomes,23 which is similar to the results of our study. Thus, our results suggest that patients with class II/III obesity (BMI > 35 kg/m2) need to optimize BMI before undergoing major cancer surgery. However, another recent cohort study in South Korea reported that a BMI ≥ 30 kg/m2 (obese) was associated with a lower risk of mortality after cancer surgery.24 As the study did not evaluate the impact of preoperative BMI > 35 kg/m2 on mortality after cancer surgery,24 additional studies are needed to confirm the effect of high preoperative BMI on mortality after cancer surgery.
In the subgroup analyses, BMI ≥ 35 kg/m2 was significantly associated with increased 90-day mortality in patients who underwent lung cancer or colorectal cancer surgery. Obesity is a known risk factor for postoperative lung complications, such as pneumonia, prolonged mechanical ventilation, and respiratory failure.2526 As postoperative pulmonary events are known complications after lung cancer surgery,27 the impact of severe obesity (BMI ≥ 35 kg/m2) might be significant in patients undergoing this surgery. Moreover, a nationwide inpatient sample study in the United States reported that morbid obesity (BMI ≥ 40 kg/m2) was associated with increased surgical complications and postoperative mortality.28 In an Asian colorectal cancer surgery, BMI ≥ 30 kg/m2 was associated with longer operation time, longer postoperative hospital stays, and higher conversion rate. Hence, obesity could be an independent risk factor for postoperative complications in patients undergoing colorectal surgery, possibly influencing the results in this study.
The novel finding of our study is that preoperative WC was not a significant predictor of mortality after major cancer surgery. Although BMI has been traditionally used to measure body size and nutritional status, WC, which reflects central obesity, has been suggested to be superior than BMI in predicting risk for cardiovascular disease.29 WC is strongly correlated with abdominal obesity and is the most commonly used clinical measure for body fat distribution.30 A previous pooled analysis of 650,000 adults showed that a higher WC was positively associated with higher mortality at all levels of BMI.31 However, no study has reported the effect of preoperative WC on mortality after cancer surgery, and our results suggest that preoperative WC should not be considered in predicting mortality after cancer surgery.
Our study has several limitations. First, the stages of tumors among patients with major cancers were not evaluated, which could affect mortality after cancer surgery. Moreover, the prevalence of malnutrition in patients with advanced stage tumor is high and may affect the preoperative BMI of patients who undergo cancer surgery.32 Second, there might be some residual confounders in this study, which might have affected the results. Third, the generalizability of the results may be limited because the environment or health policies for patients with cancer differ in each country. Fourth, information on the duration of cancer surgery or anesthetic technique was not included in this study because such information was not present in the NHIS database. Lastly, since we measured the BMI and WC a year prior to the surgery, there may have been changes in the measurement prior to the date of the actual surgery.
In conclusion, in South Korea, preoperative BMI < 18.5 kg/m2 and > 35 kg/m2 are associated with an elevated risk of 90-day mortality after major cancer surgery. However, preoperative WC was not significantly associated with 90-day mortality after cancer surgery. This association was more evident in patients who underwent lung, gastric, colorectal, and liver cancer surgery. Our results suggest that preoperative BMI must be optimized for better survival outcomes in major cancer surgery, whereas preoperative WC does not require optimization.
 XML Download
XML Download