

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
In recent decades, screening for fetal aneuploidy using maternal serum markers and ultrasonographic markers has become a part of the antenatal care in many countries.12 In the first trimester, maternal serum markers such as human chorionic gonadotrophin (hCG) or free β-hCG and pregnancy-associated plasma protein A (PAPP-A) in combination with the ultrasound measurement of nuchal translucency (NT) are effective screening methods, with a detection rate of 90% and false-positive rate of 5% or less.34 In the second trimester, maternal serum alpha-fetoprotein (AFP), hCG, unconjugated estriol (uE3), and inhibin A are widely used as markers in the quadruple screening test or in combination with the first screening test (integrated test), with a detection rate of 80% to 96% and false-positive rate of 5% or less.567 In these serum marker tests, several clinical factors are used for adjusting variables, such as gestational age, maternal weight, ethnicity, smoking status, parity, in vitro fertilization mode of conception, overt diabetes, and previous aneuploidy history.891011121314 These are adopted as adjusting factors because these are well-known to affect maternal serum marker concentrations.
The vanishing twin (VT), defined as a spontaneous reduction of one fetus of a twin pregnancy in the first trimester, occurs in approximately 10% to 40% of twin pregnancies.1516 In VT, the demised fetus disappears either partially or completely during gestation. Although the demised fetus may affect the concentrations of serum markers, VT is not considered as an adjustment factor for aneuploidy risk estimation. Moreover, the results of studies on this topic are also conflicting regarding the biochemical changes in serum markers of VT. The purpose of this study was to evaluate the effect of VT on first- and second-trimester maternal serum markers and NT.
METHODS
Study design
This is a secondary analysis of a multicenter prospective cohort study, which was designed to evaluate the cost-effectiveness of various prenatal test strategies for Down syndrome.17 Between December 2016 and February 2018, singleton pregnant women from 12 institutions in South Korea were enrolled in the study. Women were counseled on several options of prenatal test strategies for Down syndrome, including maternal serum screening, noninvasive prenatal test (NIPT), and invasive prenatal test. The final decision on the type of screening or diagnostic tests was made by the patient herself, and this secondary analysis study included only women who underwent serum screening tests. The available serum screening tests in Korea are dual test, triple test, quad test, integrated test, sequential test, and contingent test. Women who selected NIPT and underwent subsequent AFP measurement were also included.
At the time of enrollment, researchers collected baseline clinical characteristics, including the history of VT in the index pregnancy. The study population was divided into two groups: 1) the VT group, in which a twin pregnancy was noted in early pregnancy but was diagnosed as VT during the first trimester, and 2) the normal singleton group, which started as a singleton pregnancy from early pregnancy. The results of serum markers and NT were compared between the VT group and normal singleton group, and the concentration of serum markers was compared with the multiple of the median (MoM) of each marker.
Maternal serum screening test and measurement of NT
In women who adopted the maternal serum screening test, the type of screening test included double marker (PAPP-A and free beta-hCG), triple marker (AFP, total hCG, uE3), quad marker (AFP, total hCG, uE3, inhibin-A), integrated test, sequential test, and contingent test. The integrated test was performed using the combination of the first-trimester markers (PAPP-A and NT) and the second-trimester markers (AFP, total hCG, uE3, inhibin-A). The sequential test was performed by separate calculations of the first trimester test with free-hCG, PAPP-A, and NT and in the second trimester quad test. Each screening test was performed in each hospital or by commercial services. Between 10 and 14 weeks of gestation, NT was measured in each hospital, according to the Fetal Medicine Foundation guideline (www.Fetalmedicine.com).
Statistical analysis
Mann-Whitney U-test was used to assess the differences in the MoM values of serum markers and NT between the VT group and normal singleton group. Categorical data were compared with Fisher exact test. P values < 0.05 were defined as statistically significant. Multiple linear regression analysis was performed to determine the effect of VT after adjustment for confounding variables and significance was calculated using permutation test with 10,000 replicates. Statistical analyses were performed with the SPSS software (version 22.0; IBM Corp., Armonk, NY, USA), MedCalc Statistical Software version 13.3.1 (MedCalc Software bvba, Ostend, Belgium) and R version 3.6.0 (http://www.r-project.org).
RESULTS
Among 6,793 cases, 5,381 cases underwent serum screening tests, and 65 cases (1.21%) had a history of VT in index pregnancy. Table 1 summarizes the demographics and pregnancy outcomes of the study population. The VT group had higher median values of maternal age and pre pregnancy body mass index (BMI) and higher frequency of nulliparity and pregnancy after assisted reproduction technology. However, the pregnancy outcomes in terms of gestational age at delivery, birthweight, and mode of delivery were not different between the two groups.
Table 1
Maternalcharacteristics and pregnancy outcomes of study population
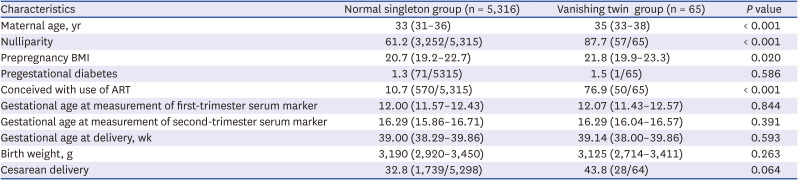
Table 2 and Fig. 1 compare the MoM values of serum markers and NT between the two groups of cases. Compared with cases in the normal singleton group, cases in the VT group had higher median MoM values of AFP (0.984 in normal control vs. 1.314 in the VT group, P < 0.001) and inhibin A (0.990 in the normal singleton group vs. 1.066 in the VT group, P = 0.047). However, there were no significant differences between the two groups in other serum markers, such as PAPP-A in the first trimester and beta-hCG and uE3 in the second trimester (Table 2). The median values of NT were not different between the two groups, either. After Permutation test with adjustment for maternal age, nulliparity, BMI before pregnancy, and pregnancy mode, the difference in the concentrations of AFP, and inhibin A remained significant. The frequency of abnormally increased AFP (> 2.0MoM) was also higher in the VT group (2.4% in the normal singleton group vs. 10.9% in the VT group, P < 0.001).
Table 2
The MoM of the first- and second-trimester serum markers and nuchal translucency in the total study population

Data are presented as median (interquartile range).
MoM = multiple of median, PAPP-A = pregnancy-associated plasma protein A, AFP = alpha-fetoprotein, t-hCG = total human chorionic gonadotropin, uE3 = unconjugated estriol, NT= nuchal translucency.
aMann-Whitney U-test.
bPermutation test with adjustment for maternal age, nulliparity, BMI before pregnancy, and pregnancy mode.
Fig. 1
The MoM of the AFP (A) and inhibin A (B) in the vanishing twin group and normal singleton group.
AFP = alpha-fetoprotein, MoM = multiple of median.
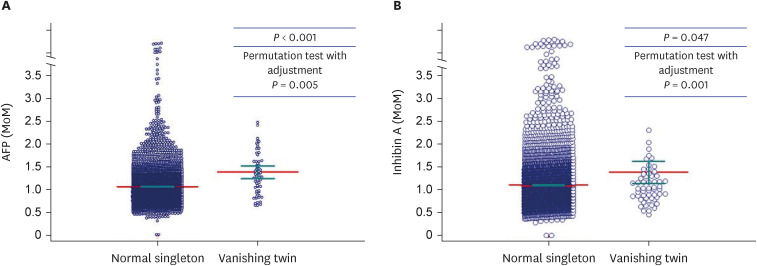
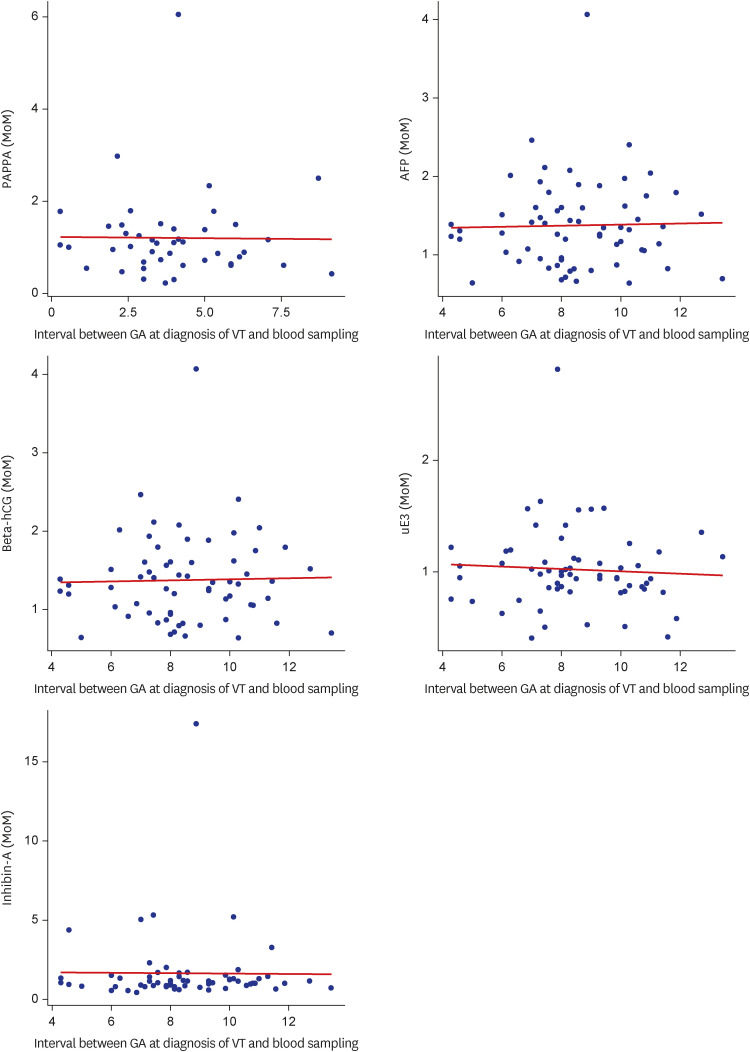
Fig. 2 shows the relationship between gestational age at diagnosis of VT and the MoM values of serum markers. None of the first- or second-trimester serum markers were correlated with the gestational age at diagnosis of VT (Spearman correlation coefficient: –0.049 for PAPP-A, P = not significant [NS]; 0.038 for AFP, P = NS; –0.108 for hCG, P = NS; 0.092 for uE3, P = NS; –0.030 for inhibin A, P = NS). Fig. 3 shows the relationship between the time from diagnosis of the VT to the blood test and the MoM values of serum markers. None of the first- or second-trimester serum markers were correlated with the time from diagnosis of the VT to the blood test (Spearman correlation coefficient: –0.086 for PAPP-A, P = NS; 0.022 for AFP, P = NS; 0.120 for hCG, P = NS; –0.077 for uE3, P = NS; 0.050 for inhibin-A, P = NS).
Fig. 2
The association between MoM of the first- and second-trimester serum markers and gestational age at diagnosis of vanishing twin (PAPP-A, P = 0.745; AFP, P = 0.765; β-hCG, P = 0.402; uE3, P = 0.476; Inhibin-A, P = 0.818).
PAPP-A = pregnancy-associated plasma protein A, MoM = multiple of median, AFP = alpha-fetoprotein, hCG = human chorionic gonadotrophin, uE3 = unconjugated estriol.
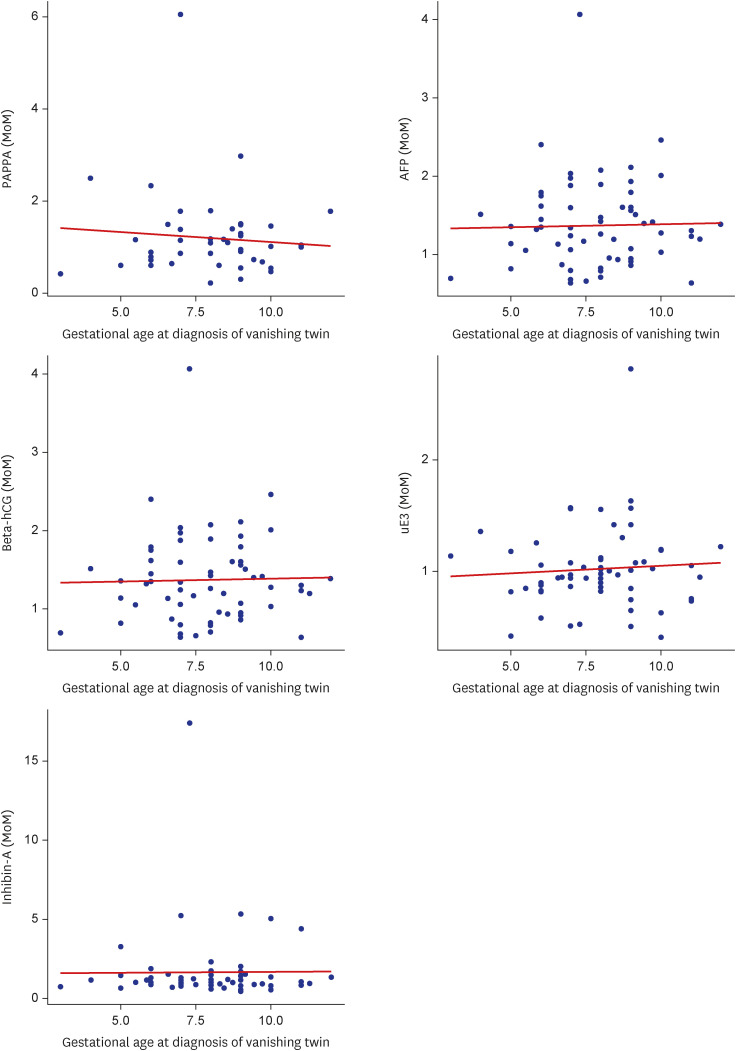
Fig. 3
The association between MoM of the first- and second-trimester serum markers and interval between gestational age at diagnosis of vanishing twin and blood sampling date (PAPP-A, P = 0.578; AFP, P = 0.861; β-hCG, P = 0.352; uE3, P = 0.549; Inhibin-A, P = 0.700).
PAPP-A = pregnancy-associated plasma protein A, MoM = multiple of median, AFP = alpha-fetoprotein, hCG = human chorionic gonadotrophin, uE3 = unconjugated estriol.
DISCUSSION
Principal findings of the study are the following: 1) Compared with cases in the normal singleton group, cases in the VT group had higher median MoM values of AFP and inhibin A, and this difference remained significant even after permutation test with adjustment for confounding variables. 2) The median MoM values of PAPP-A, β-hCG, and uE3 were not different between the two groups. 3) The frequency of abnormally increased AFP (> 2.0MoM) was also higher in the VT group than in the normal singleton group.
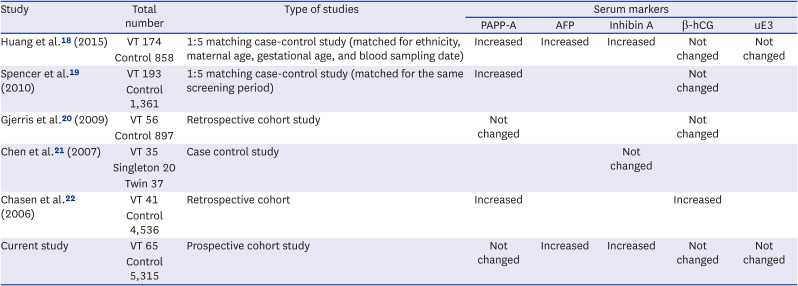
Although the demised fetus may affect the concentrations of serum markers, VT is not considered as an adjustment factor for aneuploidy risk estimation in clinical practice. Indeed, the results are conflicting with regard to the effect of VT on serum markers in previous studies (Table 3).1819202122 The current study shows that AFP and inhibin A were elevated in the VT group, whereas other markers were not different between the two groups. And after permutation test with adjustment for maternal age, nulliparity, BMI before pregnancy, and pregnancy mode, the difference in the concentrations of AFP, and inhibin A remained significant.
Table 3
Comparison with results of a previous studies about vanishing twin and maternal serum markers
| Study | Total number | Type of studies | Serum markers | ||||
|---|---|---|---|---|---|---|---|
| PAPP-A | AFP | Inhibin A | β-hCG | uE3 | |||
| Huang et al.18 (2015) | VT 174 | 1:5 matching case-control study (matched for ethnicity, maternal age, gestational age, and blood sampling date) | Increased | Increased | Increased | Not changed | Not changed |
| Control 858 | |||||||
| Spencer et al.19 (2010) | VT 193 | 1:5 matching case-control study (matched for the same screening period) | Increased | Not changed | |||
| Control 1,361 | |||||||
| Gjerris et al.20 (2009) | VT 56 | Retrospective cohort study | Not changed | Not changed | |||
| Control 897 | |||||||
| Chen et al.21 (2007) | VT 35 | Case control study | Not changed | ||||
| Singleton 20 | |||||||
| Twin 37 | |||||||
| Chasen et al.22 (2006) | VT 41 | Retrospective cohort | Increased | Increased | |||
| Control 4,536 | |||||||
| Current study | VT 65 | Prospective cohort study | Not changed | Increased | Increased | Not changed | Not changed |
| Control 5,315 | |||||||
Compared with the previous studies in Table 3, the current study has several strengths. First, we showed that AFP and inhibin A were elevated in the VT group as compared with the normal singleton group, even after permutation test with adjustment for confounding variables. Maternal age, nulliparity, BMI before pregnancy, and pregnancy mode were selected as confounding variables, as they were different between the VT group and normal singleton group and were correlated to concentrations of serum markers. Previous studies analyzed serum marker concentrations in VT, but they did not adjust for confounding factors,181921 and we also use the permutation test with adjustment for confounding variables. We used the permutation method because we need to identify the differences between the groups adjusting for the other variables. This is one of the nonparametric methods to test for the variance or relevance of variables of interest in the context of adjustment of variables. In other words, this is a type of statistical significance test in which the distribution of the test statistic under the null hypothesis is obtained by calculating all possible values of the test statistic under rearrangements of the labels on the observed data points.23
Second, the current study is a large multicenter prospective cohort study, including cases of both natural pregnancy and pregnancy conceived after assisted reproductive technology. In the current cohort, the frequency of VT was 1.21% among total singleton pregnancies, and this frequency may reflect the actual frequency in the real clinical situation, considering the frequency of twins is about 3% to 4% and the risk of VT is 10% to 40% in twin pregnancies.24
Third, to our knowledge, this is the first study to evaluate the effect of VT on serum markers in an Asian population. Most previous studies were performed in European or North American countries,181921 although the concentrations of serum markers may be different among races or ethnicities.81025 The results of our study show that VT itself can also be confounding factor in pregnant Asian women.
Why are AFP and inhibin A elevated in VT AFP is a glycoprotein produced during pregnancy. It is produced by the fetal yolk sac, fetal liver, and choroid plexus, and it crosses the placental barrier, fetal membrane, and decidua to reach the maternal blood.262728 Therefore, AFP levels are known to be elevated in both neural tube defect and fetal demise.232930 The most likely explanation for elevated AFP in VTs is tissue breakdown from the vanished twin, resulting in an increased concentration of AFP in the amniotic fluid of the remaining normal fetus. Previous studies have reported that AFP was increased in the amniotic fluid of VT3132 and in multifetal pregnancies after reduction.33
Inhibin A is produced by the human placenta and fetal membranes. Florio et al.34 reported that inhibin A is a marker of trophoblast viability, and it has also been associated with placental insufficiency in the second trimester.1834 Inhibin A is produced in considerable amounts, resulting in increasing levels in maternal serum and amniotic fluid in the presence of gestational diseases, such as preeclampsia.34 Therefore, inhibin-A may be a sign of some underlying changes of the pregnancy resulting in VT, rather than an influence of the demised twin.34
The biological half-life of AFP is about 4 to 6 days,3536 and a previous report showed that almost 50% of inhibin A disappeared from the maternal blood within the first hour after removal of the feto-placental units.37 However, in the current study, the concentrations of AFP and inhibin-A in cases of VT were not correlated to the gestational age at diagnosis of VT, suggesting that the effect of VT on elevated AFP and inhibin A is much longer than half of both markers. This is consistent with previous reports. Grau et al. showed that increased AFP lasted as long as 7 weeks in VT or selective fetal reduction,33 and Abbas et al.34 reported that elevated concentrations of maternal serum AFP persisted for at least 8 weeks in cases with selective reduction in multifetal pregnancies. Therefore, elevated AFP seems to continue at least 8 to 12 weeks after the reduction, and a longer time period seems to be needed for complete resorption of the dead fetus.
In the case of VT, elevation of MSAFP at 16–18 weeks of gestation is a well-known fact, most obstetricians ask about existence of VT when the Triple test or the Quadruple test is abnormal. Despite of this fact, VT is not included as a confounding factor in maternal serum screening tests for fetal aneuploidy. Our study showed that the concentrations of AFP and inhibin A were higher in the VT group than in the normal singleton group, and this difference remained significant even after adjustment for confounding factors. Therefore, VT may be considered an adjustment factor for risk assessment in maternal serum screening tests. However, accurate numerical correction values have not yet been presented. This study also tried to see the numerical relationship between the gestational age of missing twins and the degree of MSAFP elevation. The analysis result for this is Fig. 3. None of the first- or second-trimester serum markers were correlated with the time from diagnosis of the VT to the blood test. Further studies are needed for adequate adjustment of AFP and inhibin A in VT.
In additional, in the results of this study, the NT values of fetuses that survived VT don’t affect maternal blood like serum markers. This is because structural abnormalities on ultrasound of one fetus don’t affect twins. Chang et al.38 reported that chromosomal anomaly was diagnosed in 7.4% of fetuses with esophageal atrasia in 27 Korean pregnant women. In 2022 Ko et al.39 published a study on aneuploidy screening for second trimester soft markers in Korean women. As a prospective study in the future, if major and soft markers are included as structural markers on second trimester ultrasound with serum markers in VT, it will be more helpful in diagnosing aneuploidy.
The VT may be considered an adjustment factor for risk assessment in maternal serum screening tests.
 XML Download
XML Download