

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Over the past a few years, atherosclerotic cardiovascular disease (ASCVD) has become a chronic epidemic worldwide. Despite notable advancements in ASCVD prevention and treatment, it remains the leading cause of death worldwide; and dyslipidemia has been implicated as the most important factor in the development and progression of this disease.1
Hypertriglyceridemia is a highly prevalent lipid disorder clinically associated with populations prone to metabolic syndrome, obesity, and diabetes. For several decades, triglycerides (TGs) and TG-rich lipoproteins (TRLs) have been widely recognized as risk factors for ASCVD, marked by cumulative formation of arterial plaque.2 Although a lowering of low-density lipoprotein cholesterol (LDL-C) remains the chief goal in ASCVD prevention, TRLs and remnant cholesterol have currently gained attention as residual cardiovascular risk factors. Recent clinical trials in users of statin treatments nonetheless seem to expose a failure by TG-lowering agents to significantly reduce ASCVD events. Even with mounting support from epidemiologic and genetic studies, there is thus lingering controversy surrounding the roles of TGs and TRLs in cardiovascular disease pathogenesis.
To settle the matter, deeper research into ramifications and differing aspects of TGs, TRLs, remnant TRLs, and remnant cholesterol is essential, serving to determine how each uniquely affects the atherosclerotic process. Greater appreciation for the pathophysiologic and metabolic intricacies of TGs and TRLs has fortified emerging evidence that cholesterol as part of TRL remnants (vs TGs alone) is actually a more consequential contributor to ASCVD.
The aim of this review is therefore to provide insights into TRL remnants by addressing related concepts, metabolic/functional considerations, atherogenicity potential, and clinical repercussions of TRL remnants for cardiovascular disease prevention.
NOMENCLATURE AND CLINICAL MEANING OF TRLs AND REMNANT CHOLESTEROL
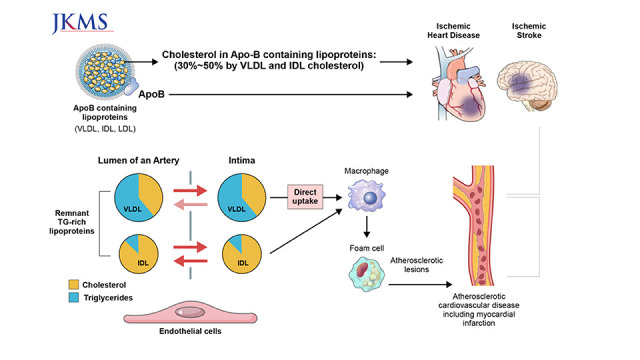
Lipoproteins are large complexes that transport hydrophobic lipids, primarily TGs and cholesteryl esters, through the bloodstream (Fig. 1).3 TRLs are lipoproteins composed primarily of core TGs, including chylomicrons, very-low-density lipoproteins (VLDLs), and intermediate-density lipoproteins (IDLs). There are two primary sources of TRLs: intestine (chylomicrons) and liver (VLDLs). These are the main sources of fatty acids for energy production in peripheral tissues or for lipid storage in adipose tissue. VLDLs produced in the liver undergo hydrolysis by lipoprotein lipase (LPL) enzyme, becoming VLDL remnants, IDL and LDL. Chylomicrons formed in the intestine are also metabolized to remnant particles, although not IDLs or LDLs. If TG levels are elevated (e.g., ≥ 260 mg/dL), there is increased secretion of TRLs and impaired lipolysis, with mostly diminished lipolysis at higher TG concentrations. Hence, circulatory accumulation of chylomicron and VLDL remnants is substantial in hypertriglyceridemic condition.4
Fig. 1
Spectrum of lipoproteins and remnant cholesterol.
HDL = high-density lipoprotein, Lp(a) = lipoprotein a, LDL = low-density lipoprotein, IDL= intermediate-density lipoproteins, VLDL = very-low-density lipoproteins, Apo = apolipoprotein, HDL-C = high-density lipoprotein cholesterol, LDL-C = low-density lipoprotein cholesterol.
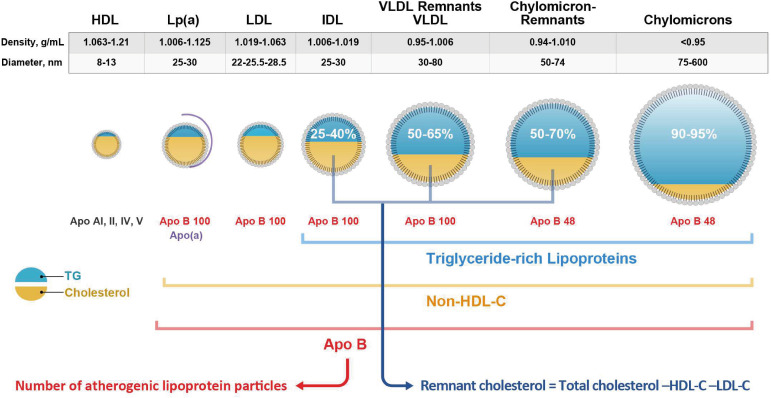
In the course of lipolysis, TRLs shrink in size due to decreasing core TG content, whereas TRL levels of cholesteryl esters increase. This lipid exchange process is facilitated by cholesteryl ester transfer protein, which relocates TGs from TRLs to LDL and high-density lipoprotein (HDL) particles and conversely transports cholesteryl esters from LDLs and HDLs to TRLs. As a result, partially lipolyzed TRLs, known as remnant TRLs, become enriched in both free and esterified cholesterol. The longer remnant TRLs remain in circulation, the more they become enriched with cholesteryl esters, eventually holding four times more cholesterol per particle than LDLs.4 Remnant cholesterol is the cholesterol component of remnant TRLs, consisting of VLDLs and IDLs in fasting states and of chylomicron remnants in nonfasting states. Results of a previous study have suggested that up to 30–50% of the cholesterol load in apolipoprotein B (apo B)-containing lipoproteins may be transported by these remnant particles, calculated as the cholesterol content of VLDL+IDL fractions. Remnant cholesterol is considered the major culprit in atherogenicity, contributing to formation of arterial plaques,5 with less direct arterial injury exerted by TGs of these TRL particles.6
Apo B is the predominant structural protein within TRLs. During lipolysis, intestine-derived chylomicrons and VLDLs of hepatic origin will lose TG content but gain in cholesterol load. However, they still retain apo B-48 and apo B-100 in chylomicron and VLDL remnants, respectively. Apo B-containing lipoproteins are contributors to atheroma formation, so degrees of atherosclerosis reflect cumulative exposures to apo B-containing lipoproteins. Because each particle retains only a single apo B molecule, apo B concentration serves as a reliable index of existing atherogenic lipoprotein particles.
MEASUREMENTS OF TRLs AND REMNANT CHOLESTEROL IN CLINICAL PRACTICE
To date, there are few established measures to precisely capture the atherogenic potential of TRLs and their remnants in a clinical setting.4 Furthermore, the dynamic catabolism that takes place alters lipid and apolipoprotein compositions of chylomicrons and VLDLs, rendering precise measurement of TRLs technically difficult. Remnant cholesterol may nevertheless be directly measured through various analytic methods, including ultracentrifugation,7 nuclear magnetic resonance spectroscopy,8 and direct automated assay (e.g., Denka Seiken Co., Tokyo, Japan).9 However, remnant cholesterol may also be calculated from a conventional lipid profile as follows: Remnant Cholesterol = Total Cholesterol − LDL-C − HDL Cholesterol (HDL-C) (Table 1). This method provides a rough estimate of remnant cholesterol content, as well as TRL-based cholesterol not yet lipolytically released as remnants. A clear advantage of this particular approach is the capacity to measure remnant cholesterol from standard lipid profiles, so there is no additional cost or need for special assay equipment.
Table 1
Methods for evaluating the risk of atherosclerotic cardiovascular disease related to triglyceride-rich lipoproteins and their remnants

| Lipid biomarker | Meaning | Measurement |
|---|---|---|
| TG | TG in all circulating lipoproteins | Directly measured (fasting or non-fasting measurement) |
| Remnant TRL particles | Partially lipolysed TRL particles by lipoprotein lipase | Directly measured: ‘Remnant-like particle’ assay42 |
| TRL cholesterol | Cholesterol carried by TG particle remnants: VLDL, IDL remnants, in non-fasting chylomicron remnants | aCalculated by the formula: total cholesterol minus HDL-C minus LDL-C or directly measured |
| Apolipoprotein B | Number of pro-atherogenic particles containing apoB-100: VLDL and remnants, IDL and remnants, and LDL and Lp(a) | Directly measured |
| Number of particles containing apoB-48: chylomicron and chylomicron remnant numbers |
TG = triglyceride, TRL = TG-rich lipoprotein, VLDL = very-low-density lipoprotein, IDL = intermediate-density lipoprotein, LDL = low-density lipoprotein, Lp(a) = lipoprotein a, HDL-C = high-density lipoprotein cholesterol, LDL-C = low-density lipoprotein cholesterol.
aModifications are available for severe hypertriglyceridaemia or very low LDL-C levels.
A recently conducted study has demonstrated that calculated remnant cholesterol does correlate well with directly measured levels, although directly measured remnant cholesterol concentrations have proven to be much higher by comparison.10 For this reason, calculated remnant cholesterol has been widely used in recent studies, with the European Atherosclerosis Society Consensus Statement endorsing utilization of both directly measured and calculated values in clinical practice. Yet, if LDL-C is calculated by Friedewald formula, where the ratio of TG to VLDL cholesterol (VLDL-C) is fixed at a 5:1, there is an inherent limitation. Such ratios may actually show individual variations, and especially at TG levels ≥ 500 mg/dL, the Friedewald formula becomes completely unreliable. Direct LDL-C measurements or new methods of estimating LDL-C levels through adjusted TG-to-VLDL-C ratios (e.g., Martin-Hopkins equation)11 may alternatively be used to more accurately calculate remnant cholesterol in circumstances of sizeable TG elevations.
It is crucial to adopt a universally accepted standard for defining remnant cholesterol and TRLs. Moreover, practical approaches must be formulated to enable accurate and convenient clinical measurement of remnant cholesterol levels in plasma.
ROLE OF TRLs IN ASCVD
Epidemiologic and genetic evidence
Over several decades, ample epidemiologic evidence has accrued to support the concept that elevated plasma levels of TGs, TRLs, and TRL remnants are causally linked to higher risk of ASCVD.
Castañer et al.12 have investigated the association between calculated remnant cholesterol and major adverse cardiovascular events (MACE) in the high-risk primary prevention Prevención con Dieta Mediterránea (PREDIMED) trial population. This study included 6,901 overweight or obese subjects at high cardiovascular risk. They identified remnant cholesterol of ≥ 30 mg/dL as a threshold for greater risk of MACE, regardless of whether LDL-C levels were on target at ≤ 100 mg/dL.
The Copenhagen City Heart Study (CCHS) and the Copenhagen General Population Study (CGPS), both prospective population cohort studies conducted in Denmark, have provided robust evidence for a correlation between elevated levels of calculated and directly measured remnant cholesterol and ASCVD in cohorts focused on primary prevention. Individuals with calculated remnant cholesterol levels ≥ 58 mg/dL (vs those at levels < 19 mg/dL) exhibited hazard ratios (HRs) of 2.6 (CCHS) and 4.2 (CGPS) for myocardial infarction (MI), 2.1 (CCHS), and 1.8 (CGPS) for ischemic stroke, and 4.9 (CCHS) and 4.8 (CGPS) for peripheral artery disease.13 Analysis of directly measured remnant cholesterol has shown similar results in relation to MI.10
Comparable results have also been reported in Korean populations without prior histories of cardiovascular disease (CVD). According to Huh et al.,14 elevated levels of remnant cholesterol (≥ 30 mg/dL) are associated with CVD incidence in adults with type 2 diabetes, independent of LDL-C levels. Lee et al.15 have likewise demonstrated an association between calculated fasting remnant cholesterol and ischemic heart disease or stroke in previously asymptomatic South Korean subjects.
In secondary prevention settings, 2,973 subjects with histories of MI and/or ischemic stroke in the CGPS cohort display a HR of 1.8 (95% confidence interval [CI], 1.3–2.5) at remnant cholesterol levels of at least 58 mg/dL (vs levels < 19 mg/dL).16 In addition, a recent meta-analysis has suggested that remnant cholesterol is associated with increased long-term risk of MACE in patients with coronary artery disease at baseline.17
Mendelian randomization (MR) studies of genetic variants for specific traits under scrutiny have shown causal associations between high remnant cholesterol levels and increased risk of ASCVD. A composite study of CGPS, CCHS, and Copenhagen Ischemic Heart Study cohorts (N = 73,513) was undertaken to examine variant genes (i.e., Tribbles hololog 1 [TRIB1], glucokinase regulatory protein [GCKR], and apolipoprotein A-V [APOA5]) that raise remnant cholesterol levels while reducing HDL-C. This effort revealed a causal risk estimate of 2.8 (95% CI, 1.9–4.2) for every 1 mmol/L increase in remnant cholesterol levels.18 Recent MR studies focused on other variant genes encoding apolipoprotein C-III (APO-CIII), LPL, and angiopoietin-like proteins 3, 4, and 8 (ANGPTL3, ANGPTL4, and ANGPTL8 have also indicated higher risk of ASCVD in conjunction with elevated TRLs and remnant cholesterol levels.1920 Elevated remnant cholesterol level has been linked to a 2.2-fold increase in risk of MI for the APOA5 gene variant21; and LPL variants showing diminished TG levels have displayed corresponding ASCVD risk reductions, similar to that achieved by lowering LDL-C and apo B.22 However, the risk reduction associated with lower TG levels was directly related to the absolute difference in total apo B levels. Finally, specific single-nucleotide polymorphisms associated exclusively with elevated TG and non-HDL-C levels seem to correlate with increased risk of coronary artery disease.23 Above findings overall signify that cholesterol carried by LDL or TRLs plays an important role in atherogenicity, which related TG content does not accurately portray.
To summarize, there are strong observational and causal relations between elevated levels of remnant cholesterol (whether calculated or directly measured) and increased risk of ASCVD in both primary and secondary prevention settings. Such associations are supported by robust genetic research.
Atherogenic mechanisms
Given their magnitude (> 75-nm diameter), TRLs are incapable of directly penetrating arterial walls. They are subsequently confined to subendothelial spaces to be engulfed by vascular macrophages. However, remnant TRLs produced through partial LPL lipolysis (via hepatic lipase) are sufficiently small (< 70-nm diameter) for active transcytosis across arterial endothelium and subsequent subendothelial retention (Fig. 2).24 Despite slower rates of intimal entry for remnant TRLs than for LDL particles, there is greater likelihood they will be trapped within the intima and thus preferentially retained.25 Accumulation of remnant TRLs contributes to initiation and progression of ASCVD-related events, including deposition of cholesterol, inflammation, and prothrombotic effects. Cholesterol in remnant TRLs accounts for at least 30% of total cholesterol by weight, having up to four times the number of cholesterol molecules per particle (vs LDL particles). TRLs also contain comparatively more apo E and apo-CIII, both associated with binding and retention of particles within arterial walls. These factors contribute to the greater deposition of cholesterol by remnant TRLs in arterial plaques.
Fig. 2
The proposed pathophysiological mechanisms from remnant lipoproteins to atherosclerosis.
VLDL = very low-density lipoprotein, IDL = intermediate-density lipoprotein, TG = triglycerides, CE = cholesteryl ester.
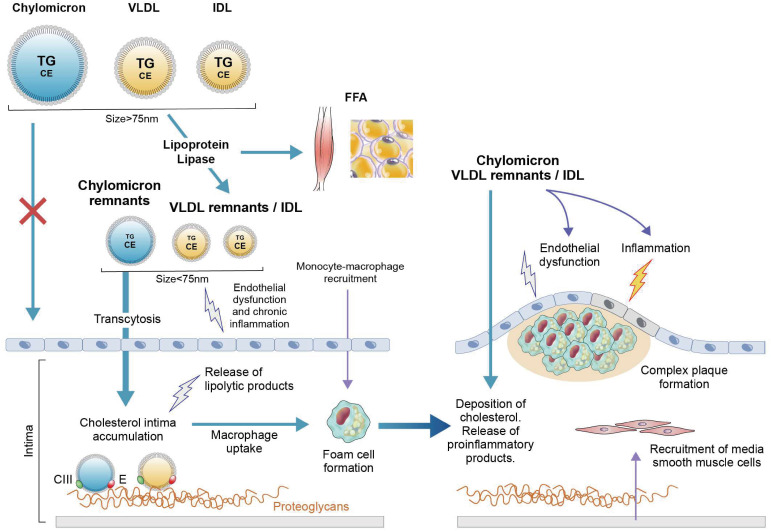
At the endothelial surface or within arterial intima, the TG component in remnant lipoproteins can be degraded into free fatty acids and glycerols by LPL and be released. Such free substances promote endothelial dysfunction and inflammation. Stimulated monocytes then migrate into arterial intima, induced by inflammatory cytokine release under low-grade inflammatory conditions, ultimately compelling uptake of lipoprotein particles and transition to foamy macrophages.2627 Migration of medial smooth muscle cells to these sites is another related alteration. Eventually, an unstable complex plaque develops, which in the event of mechanical or surface erosive failure may trigger thrombus development, luminal obstruction, and a clinical event.2829 Rather than TG directly instigating atherosclerosis, toxic elements released through lipolysis of TG in TRLs may instead be contributors to atherogenesis by inciting production of proinflammatory intermediaries (cytokines, interleukins, and adhesion molecules) that accelerate inflammation.30
MANAGEMENT OF TRLs AND REMNANT CHOLESTEROL FOR CARDIOVASCULAR DISEASE PREVENTION
Of course, the primary focus for those at high risk of ASCVD is still achieving LDL-C target goals; but to further reduce residual ASCVD risk while on maximal LDL-C lowering therapy, one must consider other therapeutic interventions that concurrently lower circulating remnant TRLs and remnant cholesterol levels. Initial steps for TRL-related disorders entail lifestyle modifications such as weight loss, emphasis on physical activity, limited alcohol intake, and avoidance of fructose-containing or high-carbohydrate foods.4 Although recognized experts have not stipulated measures for lowering plasma levels of remnant cholesterol levels, the 2019 European Society of Cardiology and European Atherosclerosis Society guidelines for managing dyslipidemia allow for pharmacotherapy in high-risk patients at TG levels > 2.3 mmol/L (or 200 mg/dL).31 Unfortunately, there is limited evidence to support pharmacologic interventions that specifically target elevated levels of TRLs to prevent ASCVD.
Recent randomized trials of omega-3 fatty acids and fibrate
Randomized controlled trials of TG-lowering treatments have produced conflicting results (Table 2). The REDUCE-IT trial evaluating icosapent ethyl, a purified form of eicosapentaenoic acid (EPA), has boasted an impressive 25% reduction in primary ASCVD outcomes, to include MACE and secondary cardiovascular events. Cardiovascular deaths fell 34%, accompanied by significant reductions in TG levels (20%), LDL-C (6.6%), and apo B (9.7%), although the impact on remnant cholesterol was not specified. These effects on LDL-C and apo-B are noteworthy and have not been observed in past trials of fibrate or of various omega-3 fatty acids. The positive outcomes here were also largely independent of the changes in TG levels. The STRENGTH trial has been the only study of omega-3 fatty acids similar to REDUCE-IT (i.e., long-term, randomized, controlled), testing a combination of EPA and docosahexaenoic acid (DHA). In this instance, there was a comparable decline in TG levels, but no significant changes in LDL-C and apo B were observed. Although reasons for these disparities remain unclear, one possibility is that EPA alone may uniquely affect atherosclerosis through its anti-inflammatory properties and other assets, including plaque stabilization and membrane fluidity. It is feasible that such features are neutralized upon addition of DHA.
Table 2
Summary of recent randomized clinical trial results with omega-3 fatty acids or fibrate
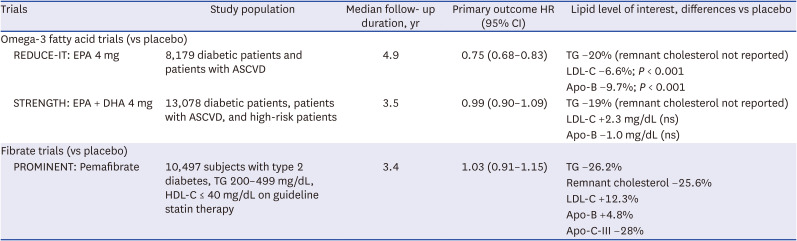
HR = hazard ratio, CI = confidence interval, TG = triglyceride, HDL-C = high-density lipoprotein cholesterol, LDL-C = low-density lipoprotein cholesterol, EPA = eicosapentaenoic acid, DHA = docosahexaenoic acid, ASCVD = atherosclerotic cardiovascular disease, Apo-B = apolipoprotein B, Apo-C-III = apolipoprotein C-III.
Clinical trials investigating the effectiveness of fibrates and peroxisome proliferator-activated receptor α (PPAR-α) agonists in lowering TG levels and reducing MACE have also yielded inconsistent findings.323334 However, subgroup analyses of participants with dyslipidemia, specifically those with TG levels ≥ 200 mg/dL and HDL-C ≤ 40 mg/dL, have shown significant benefits in terms of vascular events.35 The Pemafibrate to Reduce Cardiovascular Outcomes by Reducing Triglycerides in Patients with Diabetes (PROMINENT) trial has explored this hypothesis using the novel selective PPAR-α modulator pemafibrate.36 This particular trial logged a 26.2% reduction in TG levels and a 25.6% reduction in remnant cholesterol, but it also resulted in a 12.3% increase in LDL-C and a 4.8% increase in apo B levels. In assessing absolute changes during follow-up, a reduction (10 mg/dL) in remnant cholesterol was apparent, accompanied by an increase in LDL-C (10 mg/dL). Pemafibrate subsequently failed to reduce absolute numbers of proatherogenic apo B-containing lipoprotein particles. These outcomes imply a higher conversion of remnant cholesterol to LDL-C, rather than its effective removal from circulation. They may also explain why pemafibrate did not significantly reduce the incidence of ASCVD (vs placebo), despite substantial decline (40–50 mg/dL) in TG levels.
Emerging therapies
Considering the findings from the aforementioned PROMINENT trial, it is evident that future research should focus on investigating methods to enhance the removal of remnant TRLs and their cholesterol contents. This is achievable by targeting apolipoproteins, such as apo-CIII, ANGPTL3, and ANGPTL8, to counter their inhibitory effects on LPL. Various studies involving loss-of-function mutations have provided supportive evidence for this approach. Apo-CIII inhibits LPL and hepatic lipase, both of which degrade TGs and TRLs for removal from the blood. Volanesorsen (Waylivra; Ionis Pharmaceuticals, Carlsbad, CA, USA) is a second-generation antisense oligonucleotide (ASO) that selectively binds APOC3 messenger RNA. In the phase 3 APPROACH trial, addressing patients with severe hypertriglyceridemia, those receiving volanesorsen experienced dramatic (84%) lowering of apo-CIII levels at 3 months and marked (77%) reduction in mean TG levels, compared with increases of 6.1% and 18%, respectively in the placebo group.37
Olezarsen (Ionis Pharmaceuticals) is a N-acetyl-galactosamine (GalNAc)-conjugated ASO targeting hepatic APOC3 mRNA to inhibit apo-CIII protein production. In a phase 2 trial of 114 patients with moderately elevated TG levels (200–500mg/dL), treatment with olezarsen resulted in mean TG reductions of 23% at 10 mg every 4 weeks, 56% at 15 mg every 2 weeks, 60% at 10 mg weekly, and 60% at 50 mg every 4 weeks, compared with a 6% increase in the pooled placebo group.38 Significant decreases in apo-CIII, VLDL, non-HDL-C, and apo B were also observed.
ANGPTL3 (along with ANGPTL8) enhances the suppression of LPL and endothelial lipase (EL), leading to increased TRL levels and reduced TRL clearance efficiency. Evinacumab (Evkeeza; Regeneron Pharmaceuticals, Tarrytown, NY, USA) is a fully humanized anti-ANGPTL3 antibody that binds ANGPTL3 with high affinity. Evinacumab has been assessed in a phase 3 clinical trial for treatment of homozygous familial hypercholesterolemia (HoFH). This trial included 65 HoFH patients already receiving maximum doses of lipid-lowering therapy. Each was randomly assigned to intravenous infusion of either evinacumab (15 mg/kg every 4 weeks) or placebo. After 24 weeks, the evinacumab group exhibited significant (47.1%) reduction in LDL-C levels (vs baseline concentrations), whereas the placebo group showed minor (1.9%) increase.39 Evinacumab serves to enhance an EL-dependent pathway, bringing about reductions in lipid content in VLDL and particle size and generating remnant particles that are efficiently cleared from the circulation.40
Vupanorsen (Pfizer Inc., New York, NY, USA) is another GalNAc-conjugated ASO targeting hepatic ANGPTL3 mRNA. A phase 2 clinical trial was conducted for 6 months, involving 105 patients diagnosed with type 2 diabetes, hepatic steatosis, and hypertriglyceridemia. Administration of vupanorsen led to significant reductions (approximate values) in TGs (24–44%), remnant cholesterol (24–38%), non-HDL-C (10–19%), apo-B (3–9%) and apo-CIII (36–58%). However, LDL-C levels were essentially unchanged.41
CONCLUSION
The prevalence of hypertriglyceridemia is expected to increase, owing to continued pervasiveness of obesity, diabetes, and chronic kidney disease. Preclinical studies, together with epidemiologic and genetic research, have generated an abundance of evidence implicating remnant TRLs and remnant cholesterol in the development of ASCVD. Remnant cholesterol is deemed a valid index of ASCVD risk, particularly if LDL-C is already maintained within the recommended range. Remnant cholesterol and TRLs are thus important therapeutic targets for preventing ASCVD in high-risk individuals. Recent data from fibrate trials suggest that persistently high levels of remnant cholesterol and increased numbers of apo B-containing lipoprotein particles may carry more weight in propagation of atherosclerosis than do TG levels alone. Ultimately, newer medications aimed expressly at efficient clearance of remnant cholesterol and TRLs must be pursued.
 XML Download
XML Download