

 PDF
PDF Citation
Citation Print
Print



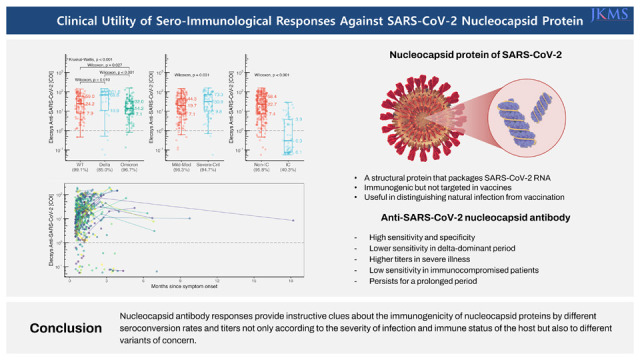
During the coronavirus disease 2019 (COVID-19) pandemic, various serologic assays for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) have been developed and utilized for diagnosis, epidemiologic investigation, and evaluation of immune status.1234567 Although quantitative measurements of spike antibodies have been of major interest, spike antibodies cannot identify natural infections anymore due to widely introduced vaccination.3 Instead, immune responses against the nucleocapsid protein provide useful information about SARS-CoV-2 infection as nucleocapsid protein is immunogenic, but not used as a vaccine target.5 However, immune responses against the nucleocapsid protein according to various clinical settings and different SARS-CoV-2 variants have not been elucidated yet. To investigate the clinical utility of sero-immunological responses against the nucleocapsid protein, we analyzed humoral and cellular responses against nucleocapsid protein during subsequent prevalence of wild-type, delta variant, and omicron variant.
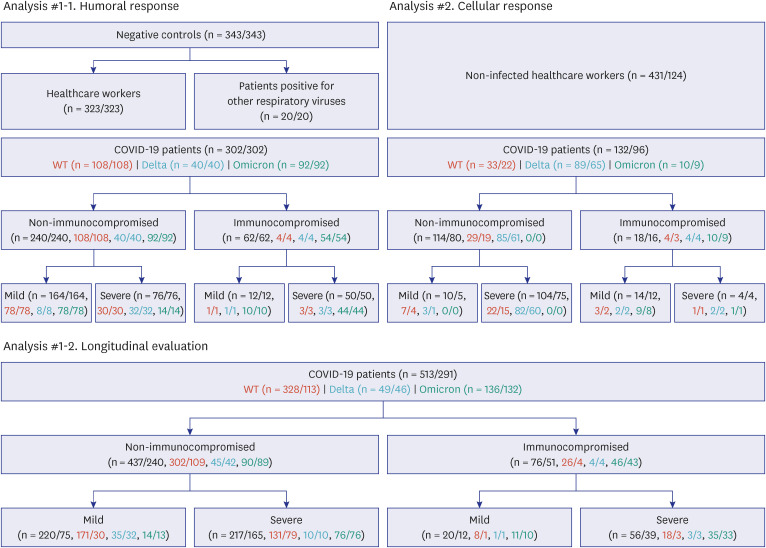
For the analysis of nucleocapsid antibodies, serum specimens collected from 645 subjects (343 negative controls and 302 COVID-19 patients) were evaluated.123467 The negative control group consisted of 323 healthcare workers (HCWs) and 20 patients positive for other respiratory viruses. Samples of the negative control group were obtained from April 2020 to August 2020, which was before the spread of SARS-CoV-2 in Korea. The COVID-19 patient group consisted of 62 immunocompromised and 240 non-immunocompromised patients. Immunocompromised patients were defined as those with solid organ transplant or hematologic malignancy, reflecting markedly impaired T- or B-cell immunity. Those with solid tumors were categorized as non-immunocompromised. There were no patients with human immunodeficiency virus infection or autoimmune diseases taking immunosuppressive agents. Among the immunocompromised patients were 42 outpatients and 20 admitted patients, eight of whom were admitted to the intensive care unit (ICU) and three of whom expired. Among the non-immunocompromised patients, there were 79 patients admitted to the ICU, two of whom expired. Of the non-immunocompromised patients, 76 requiring high-flow oxygen therapy or mechanical ventilation were classified as severe-to-critical, while 164 patients on nasal prongs or no oxygen support were considered mild-to-moderate. Longitudinal analysis for the persistence of nucleocapsid antibody was conducted with 513 samples from 291 COVID-19 patients, which were obtained after at least 14 days from symptom onset. The number of samples collected from each patient ranged from 1 to 33. SARS-CoV-2 infection was confirmed in the COVID-19 patient group with reverse transcriptase polymerase chain reaction (RT-PCR) using PowerChek 2019-nCoV Real-time PCR Kit (KogeneBiotech, Seoul, Korea). Samples of the COVID-19 patient group were collected after at least 14 days from symptom onset. For asymptomatic patients, days of illness were counted from the day of diagnosis by RT-PCR. Nucleocapsid antibodies were measured with the Elecsys® Anti-SARS-CoV-2 assay (Roche Diagnostics, Basel, Switzerland); results of at least 1.0 cut-off index (COI) were considered positive.35 Since patients with re-infection were not included in the analysis, seroconversion was defined as positive nucleocapsid antibody response (COI ≥ 1.0). As the COI reflects signal intensity of antibody response and exhibited linear correlation with neutralizing antibody titers, higher COI values were interpreted as higher antibody titer.3
To evaluate cellular immune responses against nucleocapsid protein, 563 specimens from 220 subjects (431 specimens of 124 non-infected HCWs from a COVID-19 vaccinee cohort8 and 132 specimens of 96 COVID-19 patients) were investigated. Cell-mediated immune response against the nucleocapsid protein was estimated using an interferon gamma release assay (IGRA) kit (Covi-FERON ELISA, SD Biosensor, Suwon, Korea)5 which consisted of four Covi-FERON tubes (Nil tube, Original spike protein (S) antigen tube, Nucleocapsid protein (N) antigen tube, and Mitogen tube). The S antigen tube included spike protein antigens derived from the original Wuhan-Hu-1 and B.1.1.7 variants. Details of the procedure were previously described.5
COVID-19 patients with symptom onset during January 2020 to June 2021 were considered infected with wild-type (WT) SARS-CoV-2, those during July 2021 to January 2022 with the delta variant, and those during February 2022 to December 2022 with the omicron variant based on the outbreak situation in Korea.910 The numbers of samples and individuals used in each step of the analysis are summarized in Fig. 1. Clinical characteristics were compared with Fisher’s exact test for categorical variables, Kruskal–Wallis test for continuous variables of more than two groups, and Wilcoxon test for continuous variables of two groups. Odds ratio of each characteristic was obtained with logistic regression. Assay results were compared with Kruskal–Wallis test for more than two groups and Wilcoxon test for two groups. All statistical tests were two-sided. P values of less than 0.05 were considered statistically significant. Multiple tests were adjusted with Holm’s method. Statistical analysis was conducted with R 4.3.0 (R Foundation for Statistical Computing, Vienna, Austria). Plots were depicted using ggplot2 3.4.2 on R 4.3.0.
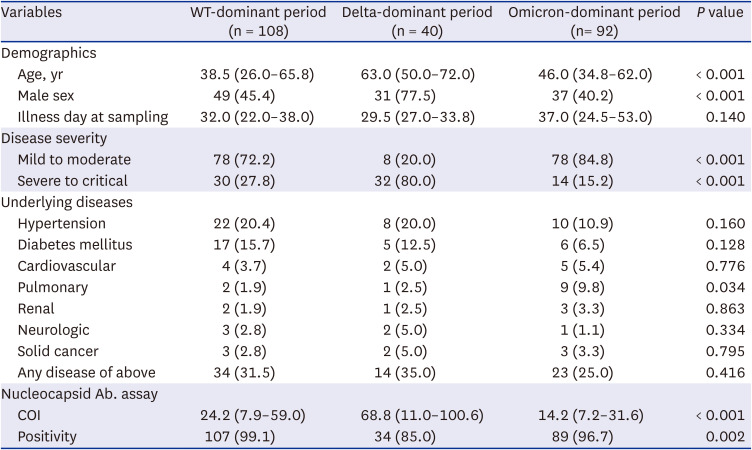
The age of the negative control group (median 31.0 years, interquartile range [IQR] 26.0–39.8 years) was significantly lower than the COVID-19 patient group (median 48.0 years, IQR 32.0–65.0 years, P < 0.001). Male consisted of 18.9% in the negative control group, whereas 52.0% in the COVID-19 patient group (P < 0.001). While information regarding the underlying diseases were not collected for the 20 patients positive for other respiratory viruses, there were only three patients with hypertension and one patient with asthma among the 323 HCWs, which was significantly lower compared to the COVID-19 patient group (P < 0.001). Refer to Table 1 and Supplementary Table 1 for the detailed characteristics of the non-immunocompromised and immunocompromised COVID-19 patients, respectively.
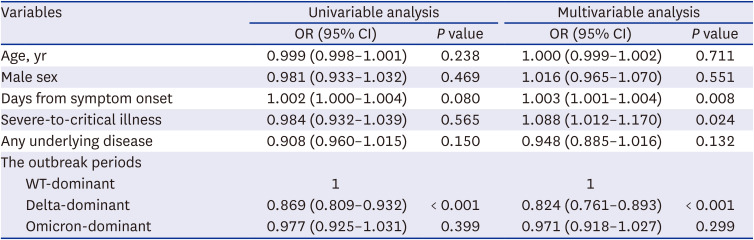
Overall, 230 of 240 sera of non-immunocompromised COVID-19 patients were positive for nucleocapsid antibody, and all specimens of negative controls were negative, showing a sensitivity of 95.8% and a specificity of 100%. A significantly lower sensitivity was noted during the delta-dominant period (n = 40, 85.0%) compared to the WT-dominant period (n = 108, 99.1%; P = 0.005) or the omicron-dominant period (n = 92, 96.7%; P = 0.045) (Table 1). The positive rate between WT-dominant and omicron-dominant periods did not differ significantly (P = 0.336). As clinical variables of each period were different, a multivariable logistic regression analysis was conducted. It revealed that the delta-dominant period was the only significant factor associated with nucleocapsid antibody positivity (odds ratio [OR], 0.869; 95% confidence interval [CI], 0.809–0.932; P < 0.001) in the univariable analysis, whereas days from symptom onset (OR, 1.003; 95% CI, 1.001–1.004; P = 0.008), severe-to-critical illness (OR, 1.088; 95% CI, 1.012–1.170; P = 0.024), and delta-dominant period (OR, 0.824; 95% CI, 0.761–0.893; P < 0.001) were significant in the multivariable analysis (Table 2).
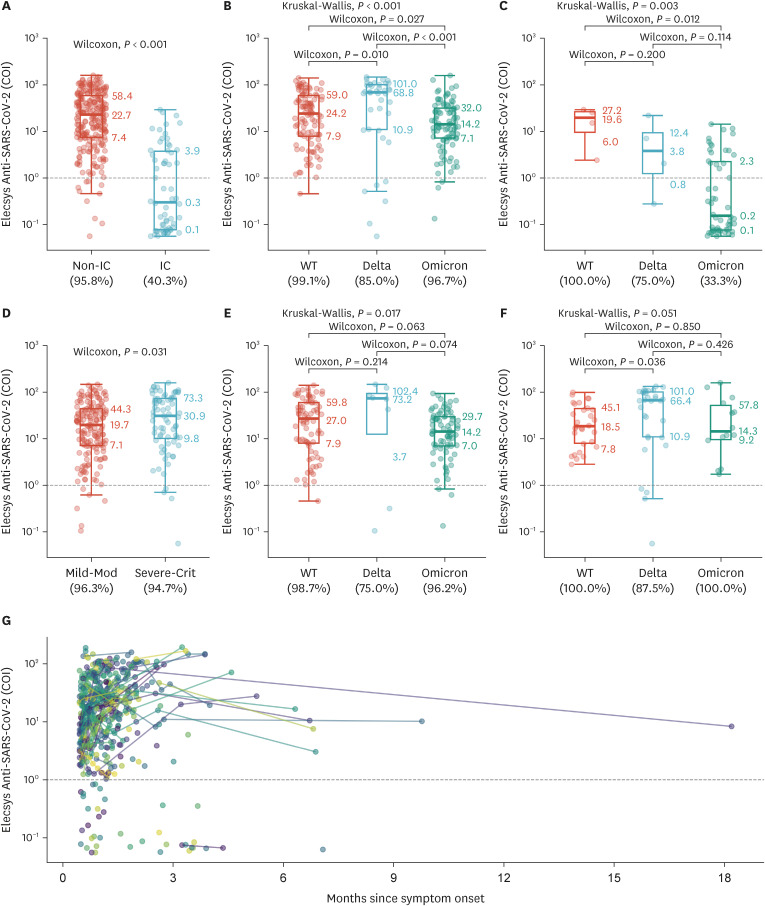
Between immunocompromised and non-immunocompromised hosts, statistically significant differences were noted both in sensitivity (40.3% and 95.8%, respectively; P < 0.001) and COI values (Fig. 2A; P < 0.001). Among the non-immunocompromised patients, COI values of the delta-dominant period were significantly higher than those of the WT-dominant and omicron-dominant periods (Fig. 2B). Although the samples of omicron-dominant period showed the lowest titer and positive rate in immunocompromised patients (Fig. 2C), there were only 4 samples obtained during both wild-type and delta-dominant periods.
In the non-immunocompromised group, the COI values of severe-to-critical illness were significantly higher than those of mild-to-moderate illness (Fig. 2D; P = 0.031). Regarding the high COI values and low sensitivity in delta-dominant period, similar trends were observed when the data were dissected according to disease severity (Fig. 2E and F). Longitudinal evaluation of 291 COVID-19 patients revealed that nucleocapsid antibody waned slowly and was persistently positive up to 556 days from symptom onset (Fig. 2G).
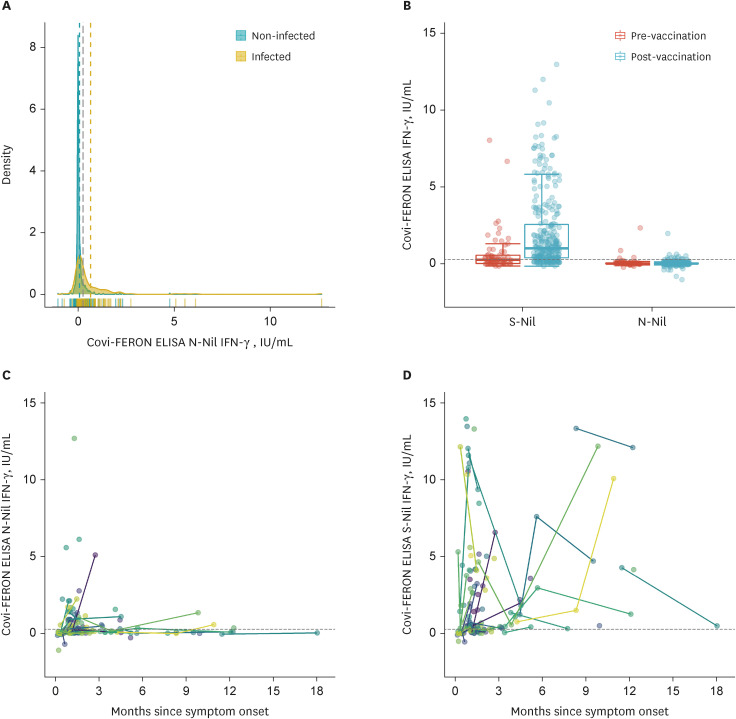
Interferon (IFN)-γ [N-Nil] concentrations of COVID-19 patients (median 0.13 IU/mL, IQR 0.03–0.70 IU/mL, range −0.72 to 12.68 IU/mL) were significantly higher than those of non-infected HCWs (median 0.01 IU/mL, IQR −0.01 to 0.07 IU/mL, range −1.04 to 4.77 IU/mL; P < 0.001). As the distribution of IFN-γ [N-Nil] between infected and non-infected individuals greatly overlapped (75 percentile value of non-infected HCWs was higher than 25 percentile value of infected patients), no suitable cut-off value of IFN-γ [N-Nil] could be determined (Fig. 3A). Among infected patients, cell-mediated immune response against the nucleocapsid protein was significantly weaker than that against the spike protein (IFN-γ [S-Nil], 1.07 IU/mL, IQR: 0.29–4.10 IU/mL; P < 0.001). As expected, IFN-γ [N-Nil] of non-infected HCWs did not increase after COVID-19 vaccination (Fig. 3B). To investigate the longevity of cellular response against nucleocapsid protein, IFN-γ [N-Nil] and IFN-γ [S-Nil] were arranged longitudinally along days from symptom onset. The sustainability of cellular response against the nucleocapsid protein was not revealed due to a low response (Fig. 3C), whereas the response against the spike protein lasted for more than a year (Fig. 3D).
In this study, we evaluated the clinical significance and utility of humoral and cellular immune responses against nucleocapsid protein of SARS-CoV-2 using nucleocapsid antibody assay and IGRA, respectively. Our study implies that the nucleocapsid antibody could serve as an indicator of both recent and remote SARS-CoV-2 infections, whereas IGRA using the nucleocapsid protein was incapable of distinguishing SARS-CoV-2 infection. Although spike antibody assays could exhibit false positivity occasionally,2 there were no false positive nucleocapsid antibody results in our negative control group. This underscores the discriminative power of nucleocapsid antibodies in determining prior and/or current SARS-CoV-2 infection. Results stratified by dominant variants showed lower sensitivity for samples obtained during the delta-dominant period compared to those obtained during the WT-dominant and omicron-dominant periods regardless of disease severity. Antibody assay might have rendered different results according to different variants possessing different mutations in the nucleocapsid gene. While the delta variant harbors the R203M variant in the nucleocapsid region, the WT and the omicron variant do not carry such mutation.11 Meanwhile, omicron variant carries R203K+G204R mutation like alpha and gamma variants,11 and the sensitivity of nucleocapsid antibody during the omicron-dominant period was not decreased compared to the WT-dominant period. Therefore, the clinical utility of nucleocapsid antibody assays should be validated with the appearance of new variants. Antigen composition in IGRA may be updated in response to variants affecting immune cell responses, although we did not observe a significant difference between WT and delta variant in our subjects (data not shown). The positive rate of nucleocapsid antibodies did not significantly differ depending on disease severity, although COI values were higher for severe-to-critical patients than for mild-to-moderate patients. Regarding the disease severity, the severe-to-critical group showing higher nucleocapsid antibody titer was in line with previous literature conducted before the omicron-dominance.1213 However, it was evident that the nucleocapsid antibody seroconversion rate was significantly lower in the immunocompromised group. The primary cause of this phenomenon would be impaired helper T-cell function of solid organ transplant recipients (positive rate 13/29, 44.8%) and decreased B-cell count and/or function among patients with hematologic malignancies (positive rate 5/25, 20.0%). While previous studies regarding the Korean population mostly focused on poor COVID-19 vaccination response in solid organ transplant recipients,1415 our study demonstrated poor nucleocapsid antibody response upon natural infection as well. IGRA showed poor sensitivity due to overlapping distribution between COVID-19 patients and non-infected individuals as well as declining T-cell response to nucleocapsid protein upon time. As cross-reactivity to the SARS-CoV-2 nucleocapsid protein has been described in the literature,16 the positive IGRA in the non-infected HCWs might have resulted from infection caused by other endemic coronaviruses. In short, the clinical utility of cell-mediated response to the nucleocapsid protein would be limited compared to nucleocapsid antibody immunoassays.
Although nucleocapsid antibody cannot distinguish remote and recent infections due to its prolonged persistence,31718 especially in severe COVID-19 patients,19 it provides instructive clues about the immunogenicity of nucleocapsid proteins by different seroconversion rates and titers not only according to the severity of infection and immune status of the host but also to different variants of concern. Nucleocapsid antibodies could serve as an indicator of prior infection distinguished from vaccine-induced immunity, and their titers could represent the disease severity. Particularly, results of nucleocapsid antibody assay in immunocompromised individuals should be interpreted with caution due to low seroconversion rates. In summary, the results of our study would aid the interpretation of nucleocapsid antibody results in various clinical settings.
 XML Download
XML Download