

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Gestational diabetic mellitus (GDM) is a common metabolic complication seen during pregnancy. According to Health Insurance Review and Assessment National Patient Sample data, the prevalence of GDM in Korea has increased over time from 5.7% in 2009 to 14.9% in 2016. Adjusted for age, GDM prevalence has increased by 11% annually from 2012–2016 in Korea.12 Also, the prevalence of GDM is increasing worldwide.34
There are many prior studies reporting the adverse pregnancy outcomes of GDM. Maternal adverse outcomes in GDM patients are increased and include the need for cesarean section due to a large-for-gestational-age (LGA) status, preterm birth, pre-eclampsia, and gestational hypertension. Also, women with GDM have an increased risk of developing type 2 diabetes compared to those who experienced a normoglycemic pregnancy. Neonatal adverse outcomes among GDM patients include macrosomia, shoulder dystocia, neonatal hypoglycemia, major malformation, and neonatal respiratory distress.567 To date, GDM screening tools and management guides have been established worldwide; moreover, most physicians follow screening, diagnosis, and management guidelines,8 and patients adhere to strict glucose control measures under the supervision of GDM education programs.
Another factor that can contribute to maternal and neonatal complications is pre-pregnancy overweightness or obesity. Obesity is increasing worldwide, and obesity in women of childbearing age is also increasing.910 According to national health statistics data from the Korea Centers for Disease Control and Prevention, the proportion of women with body mass index (BMI) values of ≥ 25 kg/m2 in 2010 was 12.1% among those aged 19–29 years and 19.0% among those aged 30–39 years, increasing to 16.5% and 21.6%, respectively, in 2019 (Korea Centers for Disease Control and Prevention, 2019). In a Korean multi-institutional study, it was found that 11.7% and 11.8% of pregnant women were obese (BMI ≥ 25 kg/m2) and overweight (23.0–24.9 kg/m2), respectively.11
It is also well recognized that the risk of perinatal complications increases in women who are overweight or obese pre-pregnancy compared to those with normal weight. The risks of LGA, macrosomia, admission to the neonatal intensive care unit (NICU), stillbirth, neonate low Apgar score, GDM, pre-eclampsia, cesarean delivery, gestational hypertension, and preterm birth are increased when the mother is overweight or obese compared to a normal weight.121314 However, in contrast to the control of GDM during pregnancy, control of maternal obesity or gestational weight gain is frequently overlooked by many patients and physicians alike, and specific supervised education focused on maternal obesity is rarely provided.
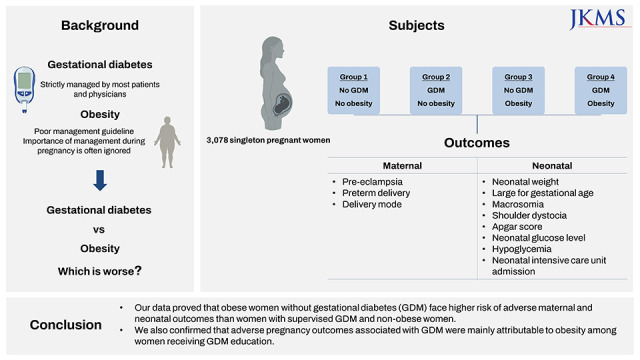
Within this background, we established a pair of hypotheses for this study. First, obese mothers without GDM would experience poorer maternal and neonatal outcomes than non-obese GDM mothers in the current clinical environment. Second, under the current GDM supervision, adverse perinatal outcomes can mainly be attributed to obesity rather than GDM itself. To prove these hypotheses, we categorized our study population into 4 groups according to the presence or absence of both GDM and obesity and examined adverse outcomes through appropriate comparisons.
METHODS
This was a retrospective cohort study performed by reviewing the electronic medical records of women who received prenatal care after a 50- or 100-g oral glucose tolerance test (OGTT) and gave birth at our institution, a tertiary hospital located in Seoul, Korea, between January 2016 and December 2020. During the study period, 3,078 consecutive singleton pregnant women were included in the study cohort. Women with pre-existing diabetes or unknown pre-pregnancy or first trimester BMI values were excluded. Our institution diagnosed GDM using a 2-step method. From 24–28 gestational weeks, all patients were screened with a 1-hour 50-g OGTT and women with a blood glucose level of ≥ 140 mg/dL underwent a 100-g OGTT based on the Carpenter–Coustan threshold for GDM diagnosis.15 The study defined obesity using a pre-pregnancy BMI of ≥ 25 kg/m2 according to criteria for the classification of obesity in Asians from the World Health Organization.16
The study population was categorized into 4 groups, as follows: group 1, no GDM without obesity; group 2, GDM without obesity; group 3, no GDM with obesity; and group 4, GDM with obesity. Women who were diagnosed with GDM participated in specialized GDM education programs offering diet and exercise details and were instructed about self-capillary glucose monitoring. After 1–2 weeks of glucose check, when the blood glucose did not meet the target level (fasting > 95 mg/dL or 2-hour postprandial > 140 mg/dL), insulin treatment was offered under physician supervision. On the contrary, no specific education protocol or supervision was provided to obese mothers.
The relevant baseline characteristics of pregnant women in this study included age, parity, pre-pregnancy BMI, gestational weight gain, chronic hypertension, glucose level after 50-g OGTT, glucose level after 100-g OGTT, glycated hemoglobin (HbA1c) level at diagnosis, and HbA1c level at delivery. For mothers whose pre-pregnancy BMI was not available, the first-trimester BMI was recorded. The perinatal outcomes included pre-eclampsia, preterm delivery (< 37 completed weeks), delivery mode, neonatal weight, LGA status, macrosomia (≥ 4.0 kg), shoulder dystocia, respiratory distress syndrome (RDS), Apgar score (at 1 and 5 minutes), neonatal glucose level, neonatal hypoglycemia (< 40 mg/dL),17 NICU admission, NICU admission days, and neonatal death. An LGA infant was defined by a size in the > 90th percentile based on a nomogram designed using national data from the Korean Health Insurance Review and Assessment Service (2009). Shoulder dystocia was defined by a delivery requiring additional manipulation, such as the McRoberts maneuver. RDS was defined as presence of respiratory grunting and retraction of the chest, an increased oxygen requirement (FiO2 > 0/4) combined with ground-glass appearance and air bronchograms on chest radiographs requiring surfactant treatment.
First, to identify differences among the 4 study groups, we performed an analysis of variance for continuous variables and the χ2 test for categorical variables. We performed an inter-group analysis of group 1 (no GDM, no obesity) versus group 3 (no GDM, obesity) to compare the outcomes according to the presence or absence of obesity in the non-GDN group. We compared group 2 (GDM, no obesity) and group 4 (GDM, obesity) to identify differences in the GDM groups according to the presence or absence of obesity to check our second hypothesis. We performed an inter-group analysis of group 3 (no GDM, obesity) versus group 2 (GDM, no obesity) to check our first hypothesis and a separate inter-group analysis of group 3 (no GDM, obesity) versus group 4 (GDM, obesity). Inter-group differences were assessed using Fisher’s least significant difference test for continuous variables and Fisher’s exact test and the χ2 test for categorical variables. A probability value of < 0.0125 was considered of statistical significance according to Bonferroni’s correction. Multiple logistic regression analysis was used to identify adjusted odds ratios (ORs) and corresponding 95% confidence intervals (CIs) for adverse outcomes while adjusting for maternal age and gestational weight gain. Group 1 was used as the reference to check how the disease groups (groups 2–4) differed from the normal group (group 1), and group 2 was used as the reference to check each hypothesis. Statistical analysis was conducted using SPSS (IBM Corp., Armonk, NY, USA).
RESULTS
Initially, 3,210 consecutive singleton pregnant women were deemed potentially eligible for this study. We excluded 53 women with pre-existing diabetes and 103 women whose pre-pregnancy or first-trimester obesity status was unknown. Finally, 3,078 women were included in the cohort and divided into 4 groups according to their obesity and GDM status (Fig. 1).
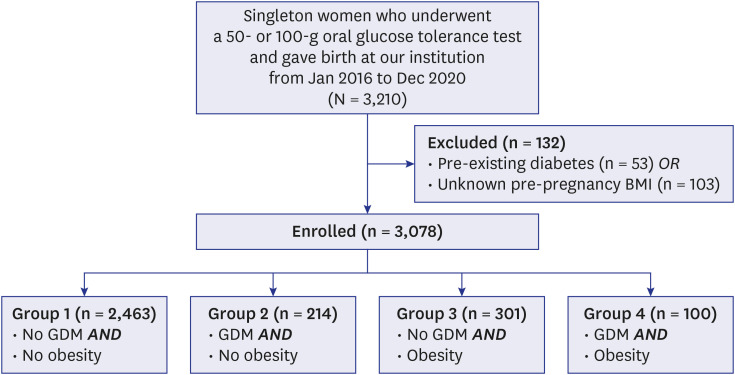
Table 1 summarizes the maternal baseline characteristics. Overall, there were significant differences in maternal age, parity, pre-pregnancy BMI, gestational weight gain, chronic hypertension, glucose level after 50-g OGTT, glucose level after 100-g OGTT, HbA1c at diagnosis, and HbA1c at delivery among the 4 groups. In a comparison of group 3 and group 4, the maternal age was higher in group 4. Of note, in non-GDM groups, group 3 showed less gestational weight gain than group 1. And in GDM groups, group 4 also showed less gestational weight gain than group 2. In a comparison of group 3 and group 2, the gestational weight gain was greater in group 3. Of note, the pre-pregnancy BMI was higher in group 4 than in group 3, but group 4 mothers gained less weight during pregnancy. The chronic hypertension rate among the 4 groups were 1.8%, 2.8%, 8.6%, and 15.0%, respectively. As shown in table 1, obese mothers had high pre-pregnancy BMI, tended to gain less weight during pregnancy, and had higher rates of chronic hypertension.
Table 1
Maternal baseline characteristics by pre-pregnancy obesity and GDM status
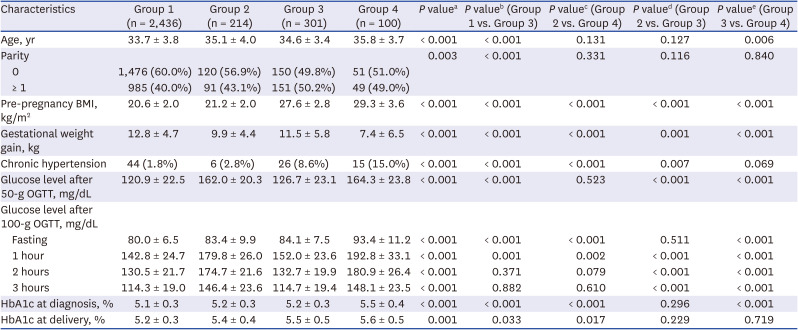
Study participants were categorized into 4 groups, as follows: no GDM, no obesity (group 1); GDM, no obesity (group 2); no GDM, obesity (group 3); and GDM, obesity (group 4).
GDM = gestational diabetes mellitus, BMI = body mass index, OGTT = oral glucose tolerance test, HbA1c = glycated hemoglobin.
aDifferences among four groups; significance was set at P < 0.0125. bInter-group difference between the “No GDM, no obesity” and the “No GDM, obesity” groups. cInter-group difference between the “GDM, no obesity” and the “GDM, obesity” groups. dInter-group difference between the “GDM, no obesity” and the “No GDM, obesity” groups. eInter-group difference between the “No GDM, obesity” and the “GDM, obesity” groups. Inter-group differences were assessed using Fisher least significant difference test for continuous variables and by Fisher’s exact test and the χ2 test for categorical variables; significance was set at P < 0.0125 with appropriate Bonferroni’s correction.
Table 2 summarizes the maternal and neonatal outcomes according to pre-pregnancy obesity and GDM status. As expected, there were significant differences in maternal and neonatal outcomes, including pre-eclampsia, preterm delivery, cesarean section, emergency cesarean section, neonatal weight, LGA infant status, macrosomia, neonatal glucose level, and NICU admission among the 4 groups. Among the non-GDM groups, group 3 had higher risk for adverse maternal outcomes including pre-eclampsia, cesarean section, and emergency cesarean section compared to group 1. In regard to neonatal outcomes, group 3 had higher rates of LGA infants, macrosomia, and NICU admission than group 1. Among the GDM groups, group 4 had higher rates of pre-eclampsia, and tended to have higher risks of cesarean section and emergency cesarean section compared to group 2. Neonates in group 4 also tended to have higher rates of LGA infants and had lower glucose levels than those in group 2. Intriguingly, group 3 had higher rates of pre-eclampsia, cesarean section, and emergency cesarean section compared to group 2. Neonates in group 3 were heavier and had lower glucose levels than those in group 2. Similarly, the rate of neonatal hypoglycemia in group 3 was higher than that in group 2. Also, group 3 tended to have higher rate of LGA infants than group 2. Among the obese groups, there were no significant differences in maternal and neonatal outcomes between non-GDM (group 3) and GDM mothers (group 4), including pre-eclampsia, cesarean section, emergency cesarean section, LGA infant status, macrosomia, neonatal glucose level, shoulder dystocia, RDS, low Apgar score, neonatal hypoglycemia, and NICU admission. Rather, neonates in group 3 were heavier than in those in group 4. As shown in Table 2, obese mothers were more associated with poor prognosis than non-obese mother with or without GDM. Also, in obese mothers, there were no significant differences of outcomes between GDM and non-GDM mothers.
Table 2
Maternal and neonatal outcomes by pre-pregnancy obesity and GDM status
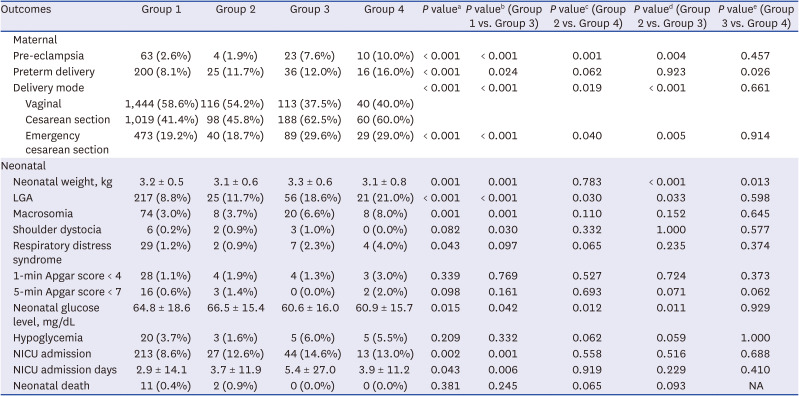
Data are presented as mean ± standard deviation or number (%). Study participants were categorized into 4 groups, as follows: no GDM, no obesity (group 1); GDM, no obesity (group 2); no GDM, obesity (group 3); and GDM, obesity (group 4).
GDM = gestational diabetes mellitus, LGA = large for gestational age, NICU = neonatal intensive care unit, NA = not available.
aDifference analysis performed according to the GDM/obesity state; significance was set at P < 0.0125. bInter-group difference between the “No GDM, no obesity” and the “No GDM, obesity” groups. cInter-group difference between the “GDM, no obesity” and the “GDM, obesity” groups. dInter-group difference between the “GDM, no obesity” and the “No GDM, obesity” groups. eInter-group difference between the “No GDM, obesity” and the “GDM, obesity” groups. Inter-group differences were assessed by Fisher’s least significant difference test for continuous variables and Fisher’s exact test and the χ2 test for categorical variables; significance was set at P < 0.0125 with appropriate Bonferroni’s correction.
Since there were significant differences in maternal age and gestational weight gain among the 4 groups, we calculated adjusted ORs for adverse outcomes after adjusting for maternal age and gestational weight gain. Groups 1 and 2 were used as references as shown in Table 3. Groups 3 and 4 had higher risks for pre-eclampsia, cesarean section, emergency cesarean section, LGA infant status, and macrosomia compared to group 1. Group 3 also had a higher risk for NICU admission than group 1. Of note, there was no significant difference in maternal and neonatal outcomes between groups 1 and 2, except for when considering LGA infant rate.
Table 3
Multivariate analysis for adverse pregnancy outcomes
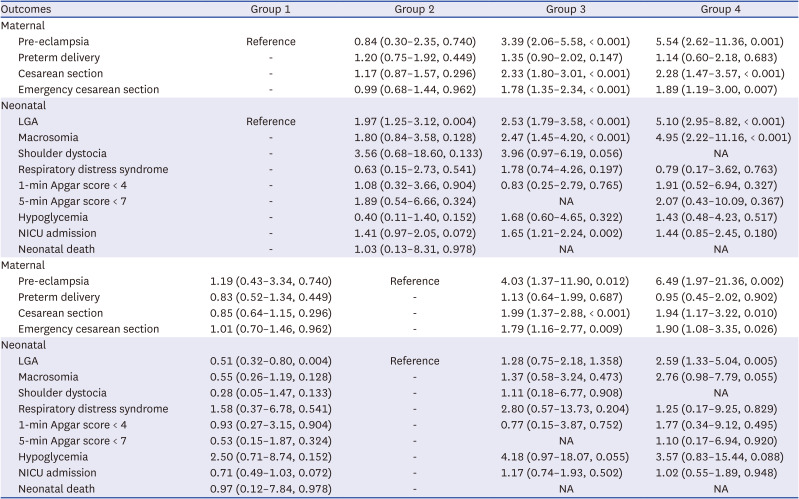
Data are presented as OR adjusted for age and gestational weight gain (95% CI, P value) values; adjusted ORs were assessed by multiple logistic regression analysis. Study participants were categorized into 4 groups, as follows: no GDM, no obesity (group 1); GDM, no obesity (group 2); no GDM, obesity (group 3); and GDM, obesity (group 4).
GDM = gestational diabetes mellitus, LGA = large for gestational age, NICU = neonatal intensive care unit, NA = not available, OR = odds ratio, CI = confidence interval.
Group 3 mothers had higher risks for pre-eclampsia (OR, 4.03; 95% CI, 1.37–11.90; P = 0.012), cesarean section (OR, 1.99; 95% CI, 1.37–2.88; P < 0.001), and emergency cesarean section (OR, 1.79; 95% CI, 1.16–2.77; P = 0.009) than group 2. Also, neonates of group 3 tended to have higher risk of hypoglycemia (OR, 4.18; 95% CI, 0.97–18.07; P = 0.055) than group 2. Among all the GDM groups, group 4 mothers were at significantly greater risk for pre-eclampsia (OR, 6.49; 95% CI, 1.97–21.36; P = 0.002), cesarean section (OR, 1.94; 95% CI, 1.17–3.22; P = 0.010), and emergency cesarean section (OR, 1.90; 95% CI, 1.08–3.35; P = 0.026) than group 2 mothers. Neonates of group 4 had higher risks of LGA infant status (OR, 2.59; 95% CI, 1.33–5.04; P = 0.005) than those in group 2. As shown in table 3, obese mothers were at greater risks of adverse perinatal outcomes than non-obese mother with or without GDM, after adjusting for maternal age and gestational weigh gain.
DISCUSSION
Our data proved that obese women without GDM have higher risks for adverse outcomes, including pre-eclampsia, cesarean section, and LGA infant status than those with supervised GDM or non-obese women. Among the GDM groups, obese GDM women more frequently experienced pre-eclampsia, cesarean section, and LGA infants than non-obese GDM women as expected. Within the obese groups, similar adverse outcomes were observed regardless of the presence of GDM. Of note, within the non-obese groups, the presence of GDM did not confer adverse outcomes. Collectively, our data indicate that obesity is a more important factor associated with adverse outcomes than GDM among Korean pregnant women receiving GDM education.
Our study falls in line with previous studies reporting that obesity is associated with adverse pregnancy outcomes. In a retrospective study of 2,454 women from Korea, obese women had higher risks for GDM, hypertensive disorder, incompetence of the internal os of the cervix, LGA infant status, and low Apgar scores than normal-weight mothers.18 According to a recent prospective cohort study of 3,454 singleton pregnant women from Korea, obesity before pregnancy also significantly increases the risk of adverse perinatal outcomes, including hypertensive disorders, GDM, and cesarean section by > 2.5 times (OR, 2.512; 95% CI, 1.817–3.473).19 In fact, the data of the present study manifested quite a similar OR for adverse pregnancy outcomes. In the earlier study, the OR for hypertensive disorders of pregnancy was 5.510 (95% CI, 2.634–11.525) in obese mothers, and, in this study, the OR for pre-eclampsia in obese GDM mothers compared to non-obese GDM mothers was 5.743 (95% CI, 1.754–18.805). Therefore, our results align with those of previous studies from Ireland and Denmark showing that obesity is an independent risk factor for adverse pregnancy outcomes in glucose-tolerant women.2021 Also, similar with our study, study from Vietnam22 showed that there were no significant differences of cesarean section and LGA infant rate between non-obese GDM mothers and non-obese non-GDM mothers. Whereas, obese but non-GDM mothers had significantly higher risks of cesarean section (OR, 1.80; 95% CI, 1.33–2.44) and LGA infant (OR, 2.75; 95% CI, 1.88–4.03) than non-obese non-GDM mothers. Also, obese mothers with GDM were at significantly higher risks of cesarean section (OR, 2.43; 95% CI, 1.49–3.96) and LGA infants (OR, 3.36; 95% CI, 1.94–5.80) than non-obese non-GDM mothers. Another study done in Finland,23 there were no significant differences of macrosomia and acute cesarean section rates between non-obese GDM mothers and normal mother. Whereas, overweight (BMI 25–29.9 kg/m2) non-GDM mothers and obese (BMI ≥ 30 kg/m2) non-GDM mothers were at significantly higher risks of macrosomia and acute cesarean section than normal mother. Also, obese GDM mothers had higher risks of macrosomia and acute cesarean section than normal mother. GDM women received dietary and lifestyle counselling and begun self-monitoring of glucose concentration according to the Finnish national guidelines. Another study from Saudi Arabia24 showed that maternal obesity influences neonatal birth weight more than gestational diabetes. These studies support our point that obese women without GDM face higher risk of adverse maternal and neonatal outcomes than women with supervised GDM and non-obese women.
Our data showing that non-obese GDM patients have similar pregnancy outcomes to those of non-obese, non-GDM patients differ from those of a previous study from the United States25 in which normal-weight (BMI < 25 kg/m2) GDM women had a higher risk of LGA infant status than normal-weight, non-GDM women. In our perspective, this difference arises from the fact that the aforementioned American study excluded women who received any form of treatment during pregnancy, which was not the case in our study. In our cohort, GDM patients were educated by a specialized GDM program that offered diet and exercise details and instructed about self-glucose monitoring. According to a Cochrane review,26 lifestyle interventions led to a reduction in the risk of LGA infant status and macrosomia among GDM women. In fact, according to a research study of GDM adverse outcomes at a single tertiary center in Korea, GDM patients experienced fewer adverse pregnancy outcomes than expected. In detail, the incidence rates of shoulder dystocia, macrosomia, neonatal hypoglycemia, respiratory distress syndrome, and admission to the NICU were 0.3%, 4.2%, 1.9%, 0.5%, and 2.9% among term births, respectively.27
It is noteworthy that our data revealed a greater prevalence of neonatal hypoglycemia in obese women without GDM than in normal-weight GDM women (6.0% vs. 1.6%). Although obesity can lead to insulin resistance, it seems unclear that neonatal hypoglycemia is increased without maternal hyperglycemia. According to a previous study of 2,459 glucose-tolerant women, neonatal hypoglycemia (defined as requiring intravenous glucose during the first 48 hours of life) was not more common in association with maternal obesity.20 According to another previous multi-center study, following adjustment of fasting plasma glucose values, ORs of clinical neonatal hypoglycemia (considered present if there was a notation of neonatal hypoglycemia in the medical record and there were symptoms and/or treatment with a glucose infusion or a local laboratory report of a glucose value of 1.7 mmol/L within the first 24 hours and/or ≤ 2.5 mmol/L > 24 hours after birth) were not significantly increased according to maternal BMI.28 On the contrary, a study from Brazil that conducted continuous blood glucose monitoring in obese women with normal glucose tolerance reported that pregnant women who were obese had higher glycemic levels than non-obese mothers,29 in line with our results.
Interestingly, our data showing that obese mothers gained less weight during pregnancy than non-obese mothers and GDM mothers gained less weight than non-GDM mothers is in line with the previous studies. In the research from Korea, diabetic women (GDM and overt diabetes patients) gained less weight than non-diabetic women during pregnancy (10.9 vs. 12.8 kg, P = 0.013).30 Another research from Korea also showed that GDM mothers gained less weight than non-GDM mothers during pregnancy.31 Also, according to another Korean research, in GDM women, gestational weight gain was less in the group with high pre-pregnancy BMI.32 As such, obese women may gain less weigh during pregnancy. Of note, relative weight gain based on the women’s pre-pregnancy BMI is more important than absolute weight gain. According to the Institute of Medicine guidelines for adequate gestational weight gain, 11.5 to 16 kg for normal weight women, 7 to 11.5 kg for overweight women, and 5 to 9 kg total weight gain is recommended for obese women.33 Therefore, group 3 (no GDM, obesity) in our study population is considered to have more weight gain than recommended (11.5 ± 5.8 kg). It is well known that excessive gestational weight gain is associated with an increasing incidence of maternal and neonatal complications.3435 Therefore, it is important to provide personalized counseling to mothers about appropriate gestational weight gain goal.
Our data support the suggestion that a systemic supervision program targeting maternal obesity is urgently needed. The current guideline of the Korean Society for the Study of Obesity recommends that physicians and patients should set a target together according to the individual’s health status.36 More specifically, the guidelines recommend mothers lose 5–10% of their body weight within 6 months as the primary goal and emphasize that losing even 3–5% of their weight could reduce the risk of cardiovascular disease. The American College of Obstetricians and Gynecologists recommends low- to moderate-intensity exercise for obese pregnant women (≥ 150 min/week) unless there are other contraindications (American College of Obstetricians and Gynecologists [ACOG] 2015). According to a Cochrane review evaluating the effectiveness of diet, exercise, or both, overweight or obese women receiving combined diet and exercise counseling interventions experienced a 15% reduced risk of infant macrosomia.37 In a study from Italy, therapeutic lifestyle changes, including to the diet (1,500 kcal/day) and the addition of mild physical activity (30 min/day, 3 times/week), could significantly reduce the risks of adverse perinatal outcomes such as GDM, gestational hypertension, and preterm delivery in women with BMI > 25 kg/m2.38 Of note, our data showed that gestational weight gain is significantly greater in obese women without GDM than non-obese GDM women, implicating that some factors are modifiable by controlling weight through exercise and diet in these populations. Not only weight control during pregnancy, but also optimizing maternal BMI before pregnancy is important as our research showed. Some research suggested the methods of pre-pregnancy lifestyle intervention. In the research from the USA,39 they suggested diet and exercise intervention started before pregnancy to lose 0.2–0.4 kg per week. Patients were encouraged to organize their diet with Dietary Approaches to Stop Hypertension dietary pattern which is consistent with ACOG nutrition guidelines during pregnancy and set customized caloric target. Women were also encouraged to exercise 60 minutes of moderate intensity physical activity and walk at least 10,000 steps per day. Another research from USA40 suggested pre-pregnancy lifestyle intervention. They suggested to loss 0.5–0.9 kg per week before pregnant. Women were encouraged to restrict dietary calorie and low-fat diet (35% fat, 20% protein, 45% carbohydrate) were suggested. Also, they suggested to increase physical activity from at least 150 minutes per week to 60 minutes per day.
It is noteworthy that only 1/3 of women with GDM were obese (BMI > 25 kg/m2) in our study population. In research from the United States, about 76.3% of GDM mothers were obese.25 In fact, the estimated population-attributable risk associated GDM was only 0.23 (95% CI, 0.20–0.26) in Asians, whereas it was as high as 0.52 (0.48–0.56) in non-Hispanic whites.41 Moreover, recent data from our institute revealed that about 10% of GDM women are underweight (BMI < 18.5 kg/m2), and these women have a rather significantly higher risk of SGA.32 Meanwhile, our data also showed that, incidence-wise, obesity is more prevalent than GDM (13.03% vs. 10.20%). Together with the finding that obese women without GDM have higher risks for adverse maternal and neonatal outcomes than supervised GDM women and non-obese women, our study implicates that we need to develop systematic management protocols targeting maternal obesity to be included in current GDM education, instead of worrying too much about well-supervised non-obese diabetes patients.
There are several limitations to our study. First, our study divided its population into obese and non-obese groups. According to previous studies, risks of adverse pregnancy outcomes such as pre-eclampsia, GDM, cesarean section, LGA infant status, macrosomia, and NICU admission are increased among women who are overweight compared to those with normal BMIs.1142 So, the poor pregnancy prognosis of overweight mothers may have been obscured in our study. Second, our study included mothers from a single tertiary hospital and thus cannot represent the total Korean population nor populations from other countries. Our institution carries out systematic education and supervision of mothers with GDM. In addition, as there are relatively many high-risk mothers in our institution, their motivation is considerable. In this setting, the prevalence of pregnancy complications may have been found to be lower than that of the general Korean population. The results may vary slightly among other hospitals where the management of GDM is insufficient or the mothers are less motivated. Therefore, our findings do not devaluate the importance of GDM management. Despite these limitations, this study has strengths; it included a large sample size and proved the current seriousness of addressing pre-pregnancy obesity.
In conclusion, our findings highlight how important pre-pregnancy obesity affects the outcome of pregnancy, regardless of GDM status. So, our study implicates the importance of weight control in women who are planning to become pregnant.
 XML Download
XML Download