

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cardiovascular disease (CVD) is the number one cause of global mortality and, in particular, premature death throughout the world, accounting for about one third of all global deaths.1 Despite the advances in cardiovascular health promotion over the past several decades, global number of deaths from CVD has increased from 12.6 million deaths in 1990 to 17.9 million deaths in 2015.2 The majority of cardiac arrest caused by CVD are still sudden onset and survival outcomes from sudden cardiac arrest (SCA) remain poor; It is estimated that approximately 40–50% of all CVD related mortalities are sudden cardiac death (SCD). Furthermore, the CVD related mortality is expected to be increasing due to increases in health behavioral risk factors and comorbidities according to aging of populations.3
During the past several decades, numerous studies made a significant contribution in identifying the major risk factors for incidence, complication, and mortality for CVD. There has been also increasing efforts to identify potential novel risk factors and biomarkers for SCD and CVD mortalities, beyond the established traditional risk factors include age, gender, smoking, diabetes mellitus, hypertension, dyslipidemia, physical inactivity, and poor diet.4567 Recently, a rapidly expanding literature has focused on the role of vitamin D in CVD related mortality and SCA,89 as accumulating evidence support crucial role of vitamin D on cardiovascular health.910 Vitamin D may favorably influence cardiovascular health through its pleiotropic effects, including downregulation of the renin-angiotensin system,11 protection against angiogenesis,12 and modulation of inflammatory/immune processes.13 Furthermore, vitamin D has direct effect on cardio-myocytes, endothelial, and vascular smooth muscle cells through its metabolites, such as vitamin D receptor.14
Despite the strong association between vitamin D and risks of CVD incidence and mortality, as well as biological plausibility from basic sciences,15 the causal links between circulating vitamin D status and SCD or CVD related mortality are conflicting and ambiguous. Moreover, it is still unclear whether vitamin D is a potential biomarker for detecting increased risk for SCD and CVD mortality. We therefore conducted this comprehensive meta-analysis of prospective cohort studies to analyze the effect of circulating vitamin D level on the risk of SCD and CVD mortality. In addition, we further examined the dose-response curve between circulating vitamin D level and SCD and CVD mortality through dose-response meta-analysis.
METHODS
This meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) statement.16
Inclusion criteria
Studies were included if they met the following criteria: 1) a prospective cohort study design was employed; 2) the population was adults population; 3) the exposure of interest was circulating vitamin D; 4) the end points were SCA, SCD, or CVD mortality; 5) adjusted hazard ratios (HRs) with corresponding 95% confidence intervals (CIs) were reported; and 6) English language. When more than one study studied the same population, the study reporting the most detailed information for both exposure and outcome was included in this meta-analysis.
Data sources
We searched the PubMed and Embase databases that had evaluated the association between circulating vitamin D and risk of SCD and CVD mortality. No restrictions on publication year were imposed.
Search strategy
In this meta-analysis, we used the following search terms: (“vitamin D” OR, “cholecalciferol” OR “calcidiol” OR “calcitriol” OR “25-hydroxyvitanin D” OR “25-OH-D”) AND (“cardiac arrest” OR “heart arrest” OR “sudden death” OR “cardiovascular death” OR “cardiovascular mortality” OR “cardiac death” OR “cardiac mortality”).
Data extraction
Two reviewers (SYK and EJ) independently screened all citations and consecutively excluded studies using the title and abstract. After initial screening, they reviewed the full manuscripts of eligible studies. Data were extracted in standard data-collection forms. Any disagreement between two reviewers were resolved in consensus meetings. Extracted data included first author’s last name, year of publication, cohort name, country, mean/median age of subjects at baseline, sample size, duration of follow-up (years), adjusted HRs with corresponding 95% CIs for lowest vs. highest circulating vitamin D levels. Measure of effects (HRs) that were adjusted for the largest number of confounding factors were considered in this meta-analysis. Quality of the included studies were assessed using the National Institute of Health “Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies” tool (https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools) (Supplementary Table 1).
Statistical analysis
We derived a pooled estimate of adjusted HRs and 95% CIs using a random-effects model, as the results provided by random effect model were more conservative.17 Heterogeneity across studies were statistically tested using Cochran’s Q statistic and the proportion of total variation was estimated using I2 statistic. I2 < 25% were considered low heterogeneity; 25% < I2
< 75% were considered moderate heterogeneity; and I2 > 75% were considered high heterogeneity.18 Publication bias was evaluated using funnel plots and Egger’s regression model19 with significance level of 10% as suggested previously.20 In the presence of publication bias, the Duval and Tweedie’s trim and fill method was utilized as a sensitivity analysis to determine the effects of missing publications on the overall estimates.
For the primary analysis, we computed a pooled HR with 95% CI for lowest vs. highest circulating vitamin D levels using Comprehensive Meta-Analysis (CMA) software version 3 (Englewood, NJ, USA). We also performed subgroup meta-analyses based on the pre-existing comorbidities (CVD, chronic kidney disease [CKD], or general population) and study endpoints (SCD or CVD mortality).
In order to overcome the limitation of meta-analysis of studies using different exposure categories, we also performed dose-response meta-analyses using the method described by Greenland and Longnecker21 and Orsini et al.22 Based on this method, the exposure distribution of cases and person-year at risk, and adjusted HRs and 95% CIs for at least three quantitative categories for exposure were required from each study. Of total included studies, nine studies had sufficient information to be included in the dose-response analyses. First, we assigned median circulating vitamin D concentration in each category to the corresponding HR for each study. If medians were not reported, we used means (n = 2). If neither the median nor the mean vitamin D concentration per category was reported, the midpoint of the upper and lower boundaries in each category was used to estimate median consumption (n = 5). If the upper boundary for the highest category was open-ended, we assumed the value of the open-ended interval to be 1.5 times that of the closest category.23 If a study used a unit other than nmol/L, the unit of vitamin D was converted to nmol/L. A potential non-linear or linear dose-response relationship between circulating vitamin D level (nmol/L) and SCD and CVD mortality was modelled by using restricted cubic splines with 3 knots at fixed percentiles (20%, 60%, and 80%) using two different reference points of 100 and 50 nmol/L, based on recommendation from the Institute of Medicine Dietary Reference Intakes committee in the United States.24 Dose-response meta-analysis was performed using R packages.
RESULTS
Literature search
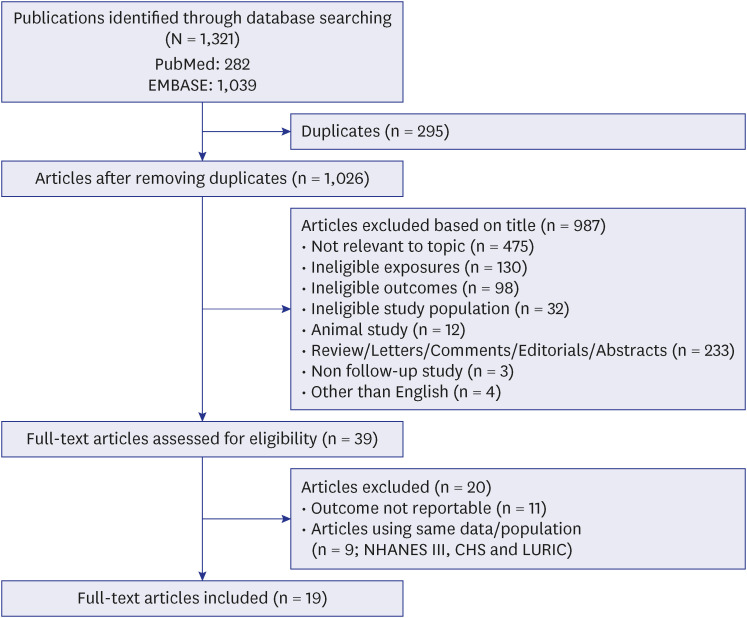
In the initial search, 1,321 publications were identified. We first excluded duplicates (n = 295). After removing duplicates, we assessed 1,026 remaining articles based on the reading of titles and abstracts. A total of 39 eligible articles were selected after screening of titles and abstracts. During the process of full-text evaluation, 20 articles were excluded due to having outcomes in unreportable form (n = 11) or using same population (n = 9). Finally, 19 articles were included for this meta-analysis.9252627282930313233343536373839404142 The flowchart of the study selection is shown in Fig. 1.
Study characteristics
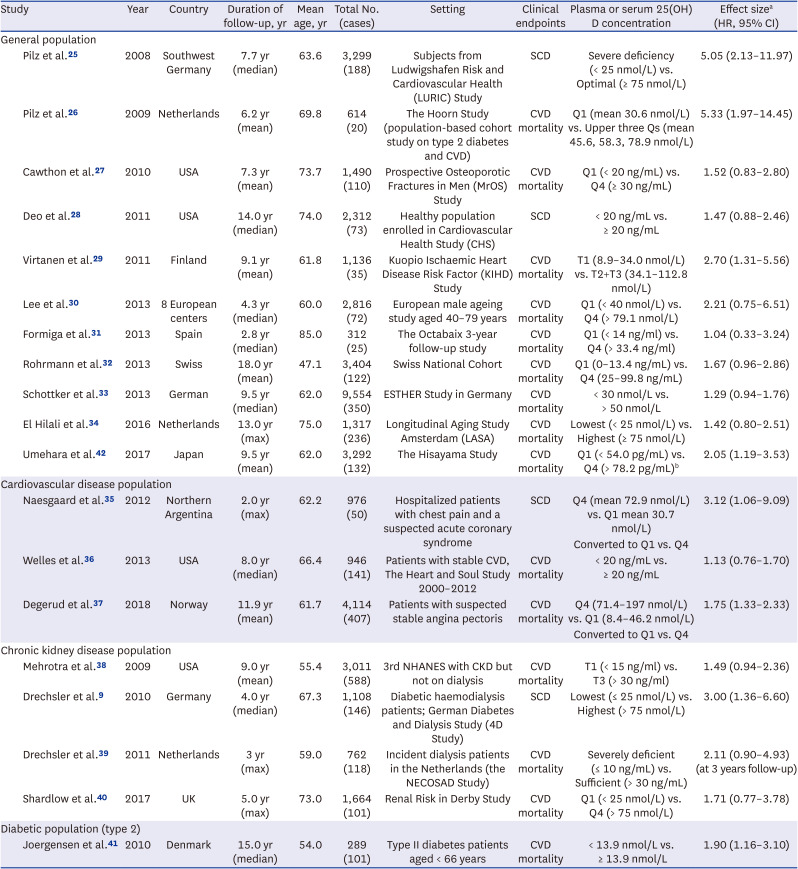
Table 1 shows the main characteristics of the 19 prospective studies on circulating vitamin D. These studies contained a total of 41,916 participants and 3,015 CVD deaths and SCD. Eighteen studies used circulating 25-hydroxyvitamin D (25[OH]D) concentrations and one study used circulating 1,25-dihydoxyvitamin D (1,25[OH]2D) as their main exposure. Thirteen of the studies were from Europe, four were from North America, one from Asia and one from South America. Eleven studies were general population-based studies, 3 studies were based on the population with pre-existing CVD, 4 studies were based on the population with pre-existing CKD, and 1 study was with diabetic population. Of all included studies, 4 studies reported SCD as the end point and the other 15 studies reported mortality from CVD as the end point.
Table 1
Characteristics of included prospective studies of circulating vitamin D concentration and risk of sudden cardiac death and cardiovascular disease mortality
| Study | Year | Country | Duration of follow-up, yr | Mean age, yr | Total No. (cases) | Setting | Clinical endpoints | Plasma or serum 25(OH)D concentration | Effect sizea (HR, 95% CI) | |
|---|---|---|---|---|---|---|---|---|---|---|
| General population | ||||||||||
| Pilz et al.25 | 2008 | Southwest Germany | 7.7 yr (median) | 63.6 | 3,299 (188) | Subjects from Ludwigshafen Risk and Cardiovascular Health (LURIC) Study | SCD | Severe deficiency (< 25 nmol/L) vs. Optimal (≥ 75 nmol/L) | 5.05 (2.13–11.97) | |
| Pilz et al.26 | 2009 | Netherlands | 6.2 yr (mean) | 69.8 | 614 (20) | The Hoorn Study (population-based cohort study on type 2 diabetes and CVD) | CVD mortality | Q1 (mean 30.6 nmol/L) vs. Upper three Qs (mean 45.6, 58.3, 78.9 nmol/L) | 5.33 (1.97–14.45) | |
| Cawthon et al.27 | 2010 | USA | 7.3 yr (mean) | 73.7 | 1,490 (110) | Prospective Osteoporotic Fractures in Men (MrOS) Study | CVD mortality | Q1 (< 20 ng/mL) vs. Q4 (≥ 30 ng/mL) | 1.52 (0.83–2.80) | |
| Deo et al.28 | 2011 | USA | 14.0 yr (median) | 74.0 | 2,312 (73) | Healthy population enrolled in Cardiovascular Health Study (CHS) | SCD | < 20 ng/mL vs. ≥ 20 ng/mL | 1.47 (0.88–2.46) | |
| Virtanen et al.29 | 2011 | Finland | 9.1 yr (mean) | 61.8 | 1,136 (35) | Kuopio Ischaemic Heart Disease Risk Factor (KIHD) Study | CVD mortality | T1 (8.9–34.0 nmol/L) vs. T2+T3 (34.1–112.8 nmol/L) | 2.70 (1.31–5.56) | |
| Lee et al.30 | 2013 | 8 European centers | 4.3 yr (median) | 60.0 | 2,816 (72) | European male ageing study aged 40–79 years | CVD mortality | Q1 (< 40 nmol/L) vs. Q4 (> 79.1 nmol/L) | 2.21 (0.75–6.51) | |
| Formiga et al.31 | 2013 | Spain | 2.8 yr (median) | 85.0 | 312 (25) | The Octabaix 3-year follow-up study | CVD mortality | Q1 (< 14 ng/ml) vs. Q4 (> 33.4 ng/ml) | 1.04 (0.33–3.24) | |
| Rohrmann et al.32 | 2013 | Swiss | 18.0 yr (mean) | 47.1 | 3,404 (122) | Swiss National Cohort | CVD mortality | Q1 (0–13.4 ng/mL) vs. Q4 (25–99.8 ng/mL) | 1.67 (0.96–2.86) | |
| Schottker et al.33 | 2013 | German | 9.5 yr (median) | 62.0 | 9,554 (350) | ESTHER Study in Germany | CVD mortality | < 30 nmol/L vs. > 50 nmol/L | 1.29 (0.94–1.76) | |
| El Hilali et al.34 | 2016 | Netherlands | 13.0 yr (max) | 75.0 | 1,317 (236) | Longitudinal Aging Study Amsterdam (LASA) | CVD mortality | Lowest (< 25 nmol/L) vs. Highest (≥ 75 nmol/L) | 1.42 (0.80–2.51) | |
| Umehara et al.42 | 2017 | Japan | 9.5 yr (mean) | 62.0 | 3,292 (132) | The Hisayama Study | CVD mortality | Q1 (< 54.0 pg/mL) vs. Q4 (> 78.2 pg/mL)b | 2.05 (1.19–3.53) | |
| Cardiovascular disease population | ||||||||||
| Naesgaard et al.35 | 2012 | Northern Argentina | 2.0 yr (max) | 62.2 | 976 (50) | Hospitalized patients with chest pain and a suspected acute coronary syndrome | SCD | Q4 (mean 72.9 nmol/L) vs. Q1 mean 30.7 nmol/L) | 3.12 (1.06–9.09) | |
| Converted to Q1 vs. Q4 | ||||||||||
| Welles et al.36 | 2013 | USA | 8.0 yr (median) | 66.4 | 946 (141) | Patients with stable CVD, The Heart and Soul Study 2000–2012 | CVD mortality | < 20 ng/mL vs. ≥ 20 ng/mL | 1.13 (0.76–1.70) | |
| Degerud et al.37 | 2018 | Norway | 11.9 yr (mean) | 61.7 | 4,114 (407) | Patients with suspected stable angina pectoris | CVD mortality | Q4 (71.4–197 nmol/L) vs Q1 (8.4–46.2 nmol/L) | 1.75 (1.33–2.33) | |
| Converted to Q1 vs. Q4 | ||||||||||
| Chronic kidney disease population | ||||||||||
| Mehrotra et al.38 | 2009 | USA | 9.0 yr (mean) | 55.4 | 3,011 (588) | 3rd NHANES with CKD but not on dialysis | CVD mortality | T1 (< 15 ng/ml) vs. T3 (> 30 ng/ml) | 1.49 (0.94–2.36) | |
| Drechsler et al.9 | 2010 | Germany | 4.0 yr (median) | 67.3 | 1,108 (146) | Diabetic haemodialysis patients; German Diabetes and Dialysis Study (4D Study) | SCD | Lowest (≤ 25 nmol/L) vs. Highest (> 75 nmol/L) | 3.00 (1.36–6.60) | |
| Drechsler et al.39 | 2011 | Netherlands | 3 yr (max) | 59.0 | 762 (118) | Incident dialysis patients in the Netherlands (the NECOSAD Study) | CVD mortality | Severely deficient (≤ 10 ng/mL) vs. Sufficient (> 30 ng/mL) | 2.11 (0.90–4.93) (at 3 years follow-up) | |
| Shardlow et al.40 | 2017 | UK | 5.0 yr (max) | 73.0 | 1,664 (101) | Renal Risk in Derby Study | CVD mortality | Q1 (< 25 nmol/L) vs. Q4 (> 75 nmol/L) | 1.71 (0.77–3.78) | |
| Diabetic population (type 2) | ||||||||||
| Joergensen et al.41 | 2010 | Denmark | 15.0 yr (median) | 54.0 | 289 (101) | Type II diabetes patients aged < 66 years | CVD mortality | < 13.9 nmol/L vs. ≥ 13.9 nmol/L | 1.90 (1.16–3.10) | |
25(OH)D = 25 hydroxyvitamin D, SCD = sudden cardiac death, CVD = cardiovascular disease, HR = hazard ratio, CI = confidence interval, T = tertile, Q = quartile, NHANES = National Health and Nutrition Examination Survey, CKD = chronic kidney disease.
aBased on the fully adjusted models; b1,25-dihydroxyvitamin D measurement.
Circulating vitamin D and SCD and CVD mortality
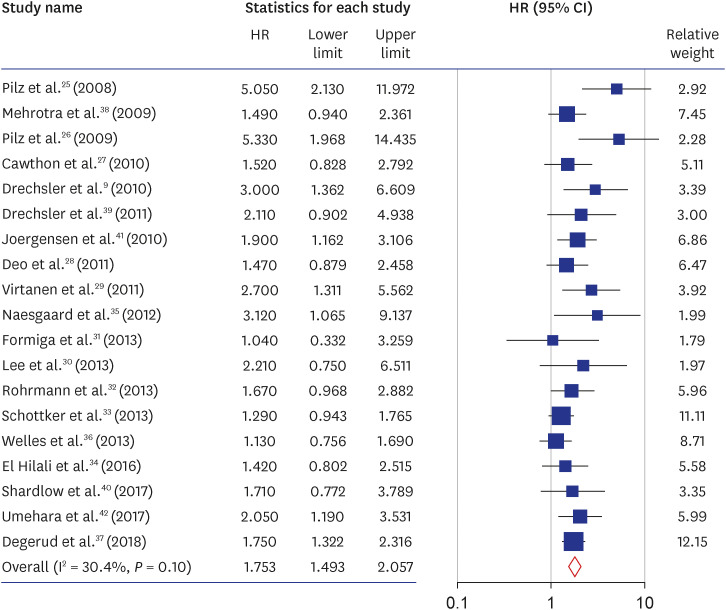
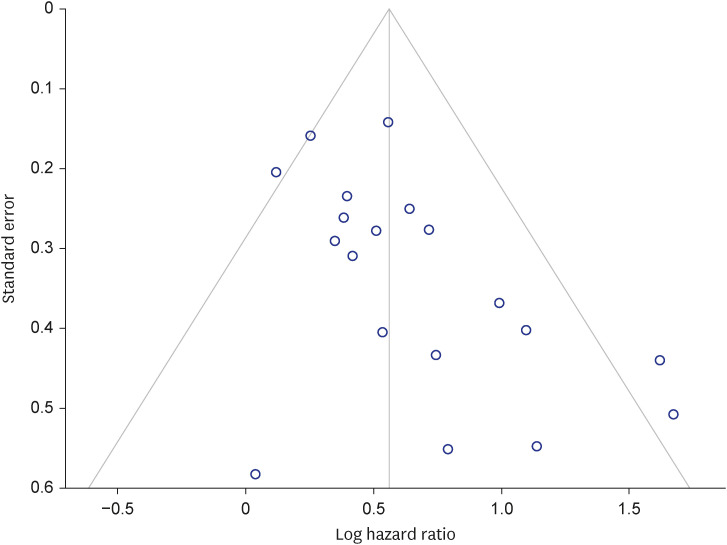
Study-specific multivariable-adjusted HRs with 95% CIs for the lowest versus highest categories of circulating vitamin D levels are shown in Fig. 2. The pooled result demonstrated a trend toward a significantly higher risk of SCD and CVD mortality associated with lower circulating vitamin D levels. The summary HR and 95% CI were 1.75 (1.49–2.06) with I2 value of 30.4% (P = 0.103), which indicates moderate heterogeneity between studies. As shown in Fig. 3, the funnel plot showed evidence of lack of symmetry. The further analysis of publication bias with the Egger’s regression also showed evidence of publication bias with P value of 0.01, which indicates the presence of significant asymmetry. However, further examination of presence of publication bias using Duval and Tweedie’s trim and fill method showed similar results (summary HR, 1.54; 95% CI, 1.28–1.85).
Fig. 2
Forest plot for study-specific and pooled hazard ratios and 95% confidence intervals of risk of sudden cardiac death and cardiovascular disease mortality for lowest versus highest categories of circulating vitamin D levels. The overall effect was obtained from a random-effect model.
HR = hazard ratio, CI = confidence interval.
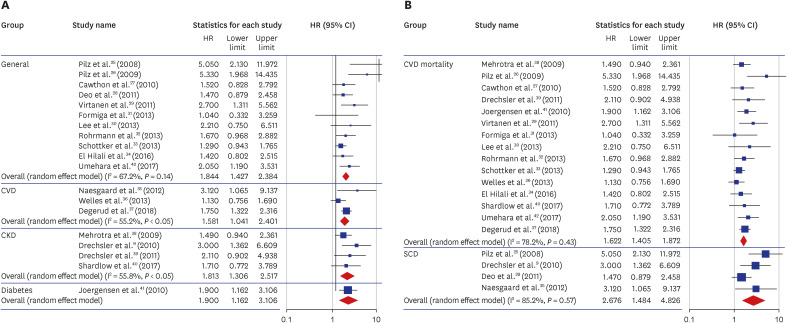
Subgroup meta-analysis
In order to investigate the impacts of pre-existing comorbidities on the results, stratified meta-analyses were performed. Fig. 4 shows stratified analyses of the associations between circulating vitamin D level and risk of SCD and CVD mortality by studies with pre-existing comorbidity status (A) and by study endpoints (B). The pooled HR (95% CI) for the 11 studies2526272829303132333442 with general population was 1.84 (1.43–2.38). The pooled HRs (95% CIs) for the studies with populations with pre-existing CVD (3 studies),353637 CKD (4 studies),9383940 and diabetes (1 study)41 were 1.58 (1.04–2.40), 1.81 (1.31–2.52), and 1.90 (1.16–3.11), respectively. We further performed stratified meta-analysis based on the study endpoints. The pooled HRs (95% CIs) for the 15 studies262729303132333436373839404142 with CVD mortality as study endpoint was 1.62 (1.41–1.87) and for the 4 studies9252835 with SCD endpoint was 2.68 (1.48–4.83).
Fig. 4
Forest plot for stratified meta-analysis and their pooled hazard ratios and 95% confidence intervals of the risk of sudden cardiac death and cardiovascular disease mortality for lowest versus highest categories of circulating vitamin D levels by (A) pre-existing comorbidity status and (B) endpoints. The overall effects for each stratified group were obtained from a random-effect model.
HR = hazard ratio, CI = confidence interval, CVD = cardiovascular disease, CKD = chronic kidney disease, SCD = sudden cardiac death.
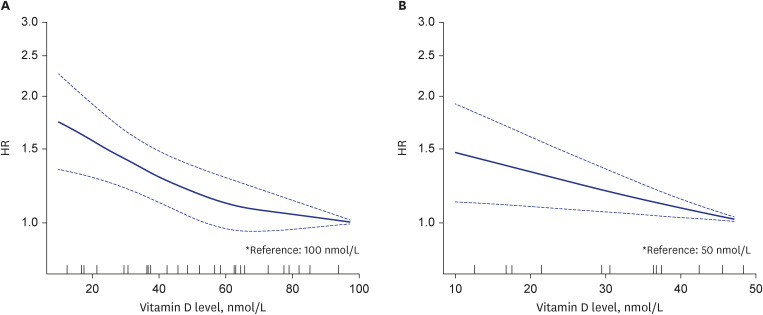
Dose-response meta-analysis
Nine studies252629313233343740 reported sufficient information for inclusion in dose-response analyses. Our dose-response analysis showed a trend of inverse association between circulating 25(OH)D and risk of SCD and CVD mortality (P for nonlinearity < 0.01, reference = 100 nmol/L) (Fig. 5A). In this dose-response analysis, any vitamin D values lower than the reference value of 100 nmol/L consistently showed hazard ratios greater than 1.00. Further analysis of dose-response relationship between circulating 25(OH)D and risk of SCD and CVD mortality with reference value of 50 nmol/L showed significant inverse dose-response relationship with 95% CIs above 1.00 at any level (Fig. 5B).
Fig. 5
Dose-response meta-analysis between circulating vitamin D level and the hazard ratio of sudden cardiac death and cardiovascular disease mortality with reference value of (A) 100 nmol/L and (B) 50 nmol/L, which is the approximate sufficient level of serum 25(OH)D recommended by the Institute of Medicine. The solid line represents point estimates with the use of a restricted cubic splines model, and the dashed lines indicate 95% confidence intervals.
HR = hazard ratio.
DISCUSSION
The findings from this meta-analysis of prospective studies showed that lower circulating vitamin D levels significantly increase the risk of SCD and CVD mortality when compared with higher levels of circulating vitamin D. This significant association was observed in both general healthy population and populations with pre-existing comorbidities, including CVD and CKD. We also observed a significant inverse dose-response relationship between circulating vitamin D levels and the risk of SCD and CVD mortality, using dose-response meta-analysis methods. To our knowledge, this is the first study to give a comprehensive review of the published observational studies on the association between blood vitamin D levels and risk of SCD and CVD mortality.
Low vitamin D levels have been identified as a risk factor for several major CVD, including coronary artery diseases, stroke, atherosclerosis, hypertension, and atrial fibrillation.104344 Several putative mechanisms on the role of vitamin D in cardiovascular health have been proposed. Vitamin D levels affect the extracellular calcium homeostasis, which in turn impact the intracellular calcium, which is a critical regulator of cardio-myocyte function and cardiac cell contractility properties.45 Vitamin D impacts the function of almost all body cell including cardiac cells, endothelial cells, and vascular smooth muscle cells through vitamin D receptor.14 Particularly, they play crucial role in cardiac cells, therefore, the absence of vitamin D receptor leads to many adverse effects on cardiac cells.46
Vitamin D from skin and diet is metabolized in the liver and converted to 25(OH)D, which in turn undergoes a second hydroxylation in the kidney and other tissues, resulting in 1,25(OH)2D, the biologically active metabolite of vitamin D.47 The 25(OH)D is the major form found in the blood and currently it is considered the best marker of vitamin D, because it is robust and reliable marker with fairly long half-life of 15 days, and also it reflects the contributions from both diet and synthesis in the skin.48 In contrast to 25(OH)D, the renal production of 1,25(OH)2D is tightly regulated by plasma parathyroid hormone levels and serum calcium and phosphorus levels and has a short half-life of 15 hours.49 Our meta-analysis included a total of 19 studies, of which 18 studies used 25(OH)D as marker for circulating vitamin D and one study used 1,25(OH)2D.
The sub-analysis of studies by population with and without pre-existing comorbidities revealed a strong trend toward a greater risk increase of SCD and CVD mortality among general population compared with populations with pre-existing CVD or CKD with 85%, 75%, and 81% increased risk in each group respectively. We had one study with diabetic population, which showed a hazard ratio of 1.90 (1.16–3.11). Although this 90% increase in the risk of SCD and CVD mortality for those with low circulating vitamin D shows greater risk than the other three populations (general, pre-existing CVD, and CKD), since this is based on only one study, careful interpretation is needed. Moreover, when we stratified studies by their clinical endpoint, the pooled result of four studies with SCD outcome showed strong association with circulating vitamin D than the pooled results of studies with CVD mortality outcome (pooled HRs [95% CIs]: 2.68 [1.48–4.83] vs. 1.62 [1.41–1.87]). This suggests that low circulating vitamin D levels may be a stronger risk factor for SCD than CVD mortality.
Our dose-response analysis further confirmed the significantly negative association between circulating 25(OH)D and SCD and CVD mortality. One of the limitations of meta-analysis of biomarker studies is combining of the results of studies with different cut-points. By conducting dose-response analyses, we could standardize circulating 25(OH)D categories in studies with different cut-points to better extrapolate the results, with two different reference points of 100 nmol/L and 50 nmol/L. The Institute of Medicine Dietary Reference Intakes committee in the United States suggested that people are at risk of deficiency at serum 25(OH)D concentrations < 30 nmol/L; potentially at risk of inadequacy at serum 25(OH)D concentrations from 30–50 nmol/L; and vitamin D sufficient at concentrations > 50 nmol/L.24 While both analyses further confirmed a trend of negative association, the one with 50 nmol/L reference showed stronger and significant inverse dose-response relationship, which suggests that low or insufficient circulating vitamin D levels would be a potential biomarker for detection of risks for SCD and CVD mortality.
Our meta-analysis has several limitations. First, although we performed a comprehensive literature search, publication bias cannot be ruled out, which may have distorted the study results in either direction. Based on the funnel plot and Egger’s regression methods, we observed some evidence of publication bias. Therefore, we further utilized the Duval and Tweedie’s trim and fill method, which allowed us to impute the studies that may actually exist and are missing from our analysis. The trim and fill method showed the similar estimation of the pooled result, supporting the validity of our meta-analysis. Second, circulating vitamin D levels measured in all of our included studies were measured at the baseline. Durations of follow-up of the included studies range from 2 years to 18 years, and circulating vitamin levels measured at the baseline may not reflect changes in vitamin D levels following the date of study initiation. It is possible that those with low vitamin D level individuals change their dietary and/or outdoor activity habits, which are the major sources of vitamin D, after the study initiation, particularly for those with longer follow-up periods. Therefore, an over- or under-estimation of association between SCD and CVD mortality risk and the true level of circulation vitamin D may have resulted. Third, although subgroup analysis was performed according to patients' comorbidities and study outcomes, there are limitations in generalizing and interpreting the results of this study. Fourth, although PubMed and Embase were used as search methods in this study, it is possible that there are studies that were omitted from the analysis, excluding search programs such as CINAHL and the Cochrane Library.
Last, our included studies for the meta-analysis were all published studies.
In conclusion, the present dose-response meta-analysis showed a significant inverse dose-response relationship that lower circulating vitamin D level is a significant predictor of risk of SCD and CVD mortality. These findings provide emphasis on the importance of maintaining sufficient vitamin D level as vitamin D deficiency is a worldwide epidemic.50 Further studies should be clarified the causality of the observed association, as well as the potential underlying mechanisms.
 XML Download
XML Download