

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Glioma accounts for approximately 30% of all primary brain tumors, caused by the formation of heterogeneous tumor groups of neuroepithelial tissue, and collectively refer to most malignant central nervous system tumors [123]. According to the World Health Organization classification system, since 2007, gliomas have been divided into four histological grades based on differentiation, anaplasia, and malignancy [4]. However, as the classification system was newly established in 2021, it is divided in more detail by isocitrate dehydrogenases (IDH) status, 1p/19q codeletion status, and molecular profile [5]. Although glioma is generally found in adults over the age of 50, it is also one of the most common solid tumors in children and adolescents under the age of 19 years [36]. To date, the effective treatment of gliomas remains a challenge. Surgical resection can reduce the size of the tumor, but complete resection is impossible due to its invasiveness. Extensive resection can remove more tumor cells, but damage to neuronal function is inevitable, which can adversely affect the patient’s quality of life [78]. To overcome the limitations of surgical resection, adjuvant treatments, such as radiation therapy and chemotherapy, have been studied; however, many cases lead to death due to resistance and recurrence [9]. The survival period varies considerably between patients, but for patients with glioblastoma (GBM) classified as grade IV, the average survival period is approximately one year [4]. Despite this, there are currently no approved targeted therapies for GBM, which is largely attributed to the lack of reliable glioma biomarkers [1011]. Therefore, to develop effective treatments and improve prognosis, a more detailed understanding of glioma is required, and research from various perspectives is necessary.
The highly immunosuppressive microenvironment of gliomas is associated with a lack of antitumor immune response and inhibits the efficacy of immunotherapy [12]. Tumor microenvironmental factors cause glioma cells to evade the immune system, and these factors are not only the result of the tumor but also chronic inflammation [12]. Inflammation is a complex immune response to stimulants, such as pathogens and damaged cells. Innate immune responses are involved in various inflammatory processes and play an important role in maintaining tissue homeostasis against infection or damage caused by bacteria and viruses [1314]. However, chronic inflammation can contribute to a wide range of diseases, including heart disease, stroke, multiple sclerosis, neuropathic pain, and cancer, due to overproduction of inflammatory cytokines and subsequent tissue damage [151617181920]. Indeed, about 15% of all cancer-related deaths appear to be related to inflammation, and chronic inflammation within the tumor microenvironment is thought to occur as a result of oncogene expression, leading to genetic mutations [21].
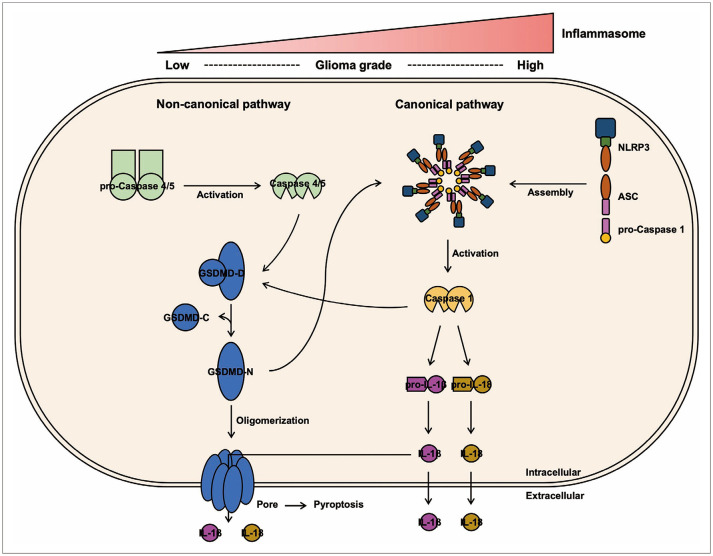
The inflammatory response comprises an inflammatory trigger, a sensor that detects an inflammatory mediator induced by the sensor, and a target tissue affected by the inflammatory mediator [1322]. The key to the inflammatory response is inflammasome activation, which is a cytoplasmic multiprotein complex composed of NOD-like receptors (NLRs), apoptosis-associated speck-like proteins, including caspase recruitment domains (CARDs) acting as adapters, and pro-caspase-1 [1623]. It serves to mediate stimulation of inflammatory caspases, resulting in rapid release of proinflammatory cytokines [24], and as research has progressed, inflammasomes containing components other than NLRs have been identified [25]. Currently, seven forms are widely accepted, including the NLR protein 1 (NLRP1), NLRP3, NLRC4, AIM2, IFI16, and pyrin inflammasomes and the non-canonical inflammasome [252627]. Inflammasomes are classified as either “canonical” or “non-canonical,” depending on the pathway of activation [28]. The canonical inflammasome pathway involves the assembly of related components to form the inflammasome, which then activates pro-caspase-1 through cleavage to secrete interleukin (IL)-1β and IL-18 [29]. In the non-canonical inflammasome pathway, activated caspase-4 and caspase-5 cleave gasdermin-D (GSDMD), an effector protein, into its N- and C-forms [3031]. The N-form GSDMD oligomerizes to form pores in cell membranes, leading to inflammation-programmed cell death called pyroptosis, which results in release of cytoplasmic contents into the extracellular space, accompanied by cell swelling and membrane rupture [32]. Previous studies have shown that caspase-1 also cleaves GSDMD to promote the release of IL-1β and IL-18 and that non-canonical inflammasomes activate the canonical NLRP3 inflammasome [2531]. Inflammasome dysregulation has been shown to be associated with tumor development, autoimmune diseases and neurodegenerative diseases [333435]. The most studied NLRP3 inflammasome is known to induce angiogenesis and confer a mesenchymal phenotype by upregulating the production of IL-1β in GBM [36]. Among these, we investigated the expression patterns in glioma patient tissues, focusing on non-canonical inflammasomes, including the most representative canonical NLRP3 inflammasome, to ensure whether the non-canonical inflammasome is associated with the glioma malignancy and to evaluate its potential as a biomarker.
Pyroptosis, a proinflammatory cell death mediated by GSDMD, was first described in 1992 in myeloid cells infected by pathogens or bacteria. Although pyroptosis plays an important role in clearing bacterial and viral infections by enhancing the host’s defense response, its dysregulation can cause tissue damage as it amplifies local or systemic inflammatory effects [373839]. A recent study showed that pyroptosis in cells in hypoxic regions within tumors contributed to chronic tumor necrosis, suppressing anti-tumor immunity and promoting tumor progression [40]. Thus, sustained activation of non-canonical inflammasomes in tumors can trigger pyroptosis to secrete proinflammatory cytokines, thereby creating an inflammatory tumor microenvironment and contributing to tumor progression.
In this study, we aimed to confirm the presence of a non-canonical inflammasome pathway in gliomas, subsequently investigating its correlation with malignancy and evaluating its potential as an aggressiveness marker for inflammation-related molecules. Our results indicate that the expression levels of non-canonical inflammasome-related molecules are upregulated as the grade increases in glioma patient samples. In addition, we confirmed the tendency of the number of apoptotic cells to increase according to grade. This establishes the importance of the non-canonical inflammasome in glioma malignancy and suggests its potential as an aggressiveness for gliomas.
MATERIALS AND METHODS
Computational analysis
All bioinformatic analyses including survival analysis, gene expression analysis, and correlation analysis were conducted using GlioVis (http://gliovis.bioinfo.cnio.es/) and GEPIA 2 (http://gepia2.cancer-pku.cn/). Kaplan-Meier survival analysis was conducted, and hazard ratio were calculated by coxph function. In the GBMLGG dataset from The Cancer Genome Atlas (TCGA; https://www.cancer.gov/ccg/research/genome-sequencing/tcga), data from at least 330 patients in both the high and low groups were used for survival analysis, and data from a total of 620 patients were used for mRNA expression analysis, including grades II, III, and IV. Comparing gene expression between normal brain tissue from GTEX dataset (https://gtexportal.org) and glioma samples from GBMLGG dataset was conducted in GEPIA 2.
Patient samples
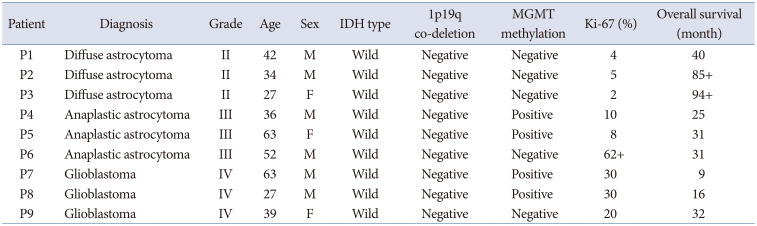
IDH mutation status of all patients was wild type. According to the recently updated WHO 2021 classification, all patients were diagnosed with GBM, IDH-wild type. But these patients were diagnosed before 2020. So, according to WHO 2016 criteria, 3 patients were diagnosed with GBM (WHO grade IV), three anaplastic astrocytomas (WHO grade III), and three diffuse midline gliomas (WHO grade II). The median age of the patients was 39 years (range, 27–63 years). The detailed clinical information on the patient tissue is shown in Table 1.
All glioma patient tissues were obtained surgically from Bundang CHA Medical Center, Republic of Korea, under Institutional Review Board approval (No. CHAMC2021-01-024-001) and all patients signed informed consent forms. Tissues were stored at -80℃.
Immunohistochemistry
Formalin-fixed, paraffin-embedded glioma blocks were serially sectioned at 4-µm thickness and deparaffinized in xylene (Thermo Fisher Scientific, Waltham, MA, USA). The sections were immersed in ethanol, rehydrated, and incubated with goat serum to block nonspecific binding. They were then incubated overnight at 4℃ with the primary antibodies and subsequently incubated with secondary antibodies for 1 h at room temperature. Images were acquired using a confocal laser scanning microscope (Zeiss LSM; Carl Zeiss AG, Jena, Germany) and quantified using ImageJ v1.52a (National Institutes of Health, Bethesda, MD, USA).
Hematoxylin and eosin staining
Human glioma brain tissues were harvested and fixed in 4% formaldehyde. Paraffin-embedded glioma blocks were prepared and serially sectioned to a thickness of 4 µm. For the hematoxylin and eosin (H&E) histological study, the sections were stained with H&E and examined under a confocal laser scanning microscope (Zeiss LSM).
Terminal deoxynucleotidyl transferase dUTP nick-end labeling assay
To evaluate in situ glioma cell death, 4-µm sections of formalin-fixed, paraffin-embedded blocks of glioma tissue samples were prepared. The sections were permeabilized with 0.1% (w/v) Triton X-100 and incubated with terminal deoxynucleotidyl transferase dUTP nick-end labeling (TUNEL) reagent (Merck GmbH, Darmstadt, Germany). The stained 9 samples were then treated with 4′,6-diamidino-2-phenylindole for 30 min. The apoptosis of single cells was examined using a confocal laser scanning microscope (Zeiss LSM).
Statistical analysis
Survival rates were analyzed using Kaplan–Meier analysis with a log-rank test. Gene expression at different malignancy grades was compared using Tukey’s honest significant difference and a paired t-test. The p-values of all results were adjusted using the false discovery rate (FDR), and an FDR <0.05 was considered statistically significant.
RESULTS
High expression of non-canonical inflammasome-related molecules correlates to the poor prognosis of glioma patients
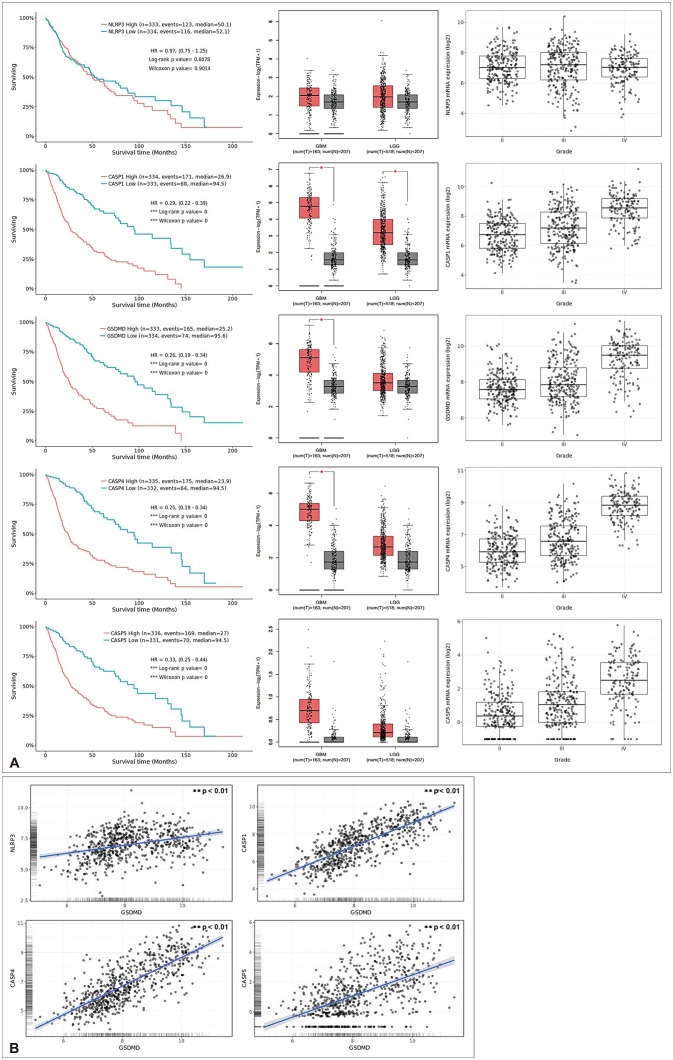
Bioinformatic analysis was performed to compare the results according to the expression patterns of inflammasome-related molecules in gliomas. In the case of NLRP3, a component of the canonical inflammasome, the median survival rate was similar at approximately 50 months, regardless of the expression pattern, and there was no significant difference in the expression level according to the tumor grade (Fig. 1A). However, the high expression of caspase-1, which is involved in both the canonical and non-canonical inflammasome pathways, and GSDMD, caspase-4, and caspase-5, which are non-canonical inflammasome-related molecules, had a median rate much lower than 50 months. In addition, as the tumor grade increased, the expression levels were upregulated. Upon comparison of the gene expression levels between gliomas and normal tissues, NLRP3 and caspase-5 were slightly higher in gliomas, although not significantly different. The expression levels of GSDMD and caspase-4 were significantly higher in GBM tissues, and caspase-1 was higher in both GBM and low-grade glioma.
Pyroptosis triggered by GSDMD is a form of programmed cell death characterized by the release of many proinflammatory factors [4142]. The release of various inflammatory mediators, including IL-18 and IL-1β, is closely related to tumorigenesis and anticancer drug resistance [43]. Therefore, we performed a correlation analysis between GSDMD, a molecular effector of pyroptosis, and canonical and non-canonical inflammasome-related molecules in gliomas. As shown in Fig. 1B, positive correlations were observed for NLRP3, casapse-1, caspase-4, and caspase-5, and particularly high correlations were observed with caspase-1/4/5.
In summary, bioinformatic analysis showed that canonical and non-canonical inflammasome-related molecules contribute to poor prognosis in gliomas and that the expression levels of non-canonical inflammasome-related molecules were upregulated according to glioma grade.
The NLRP3 inflammasome contributes to glioma progression
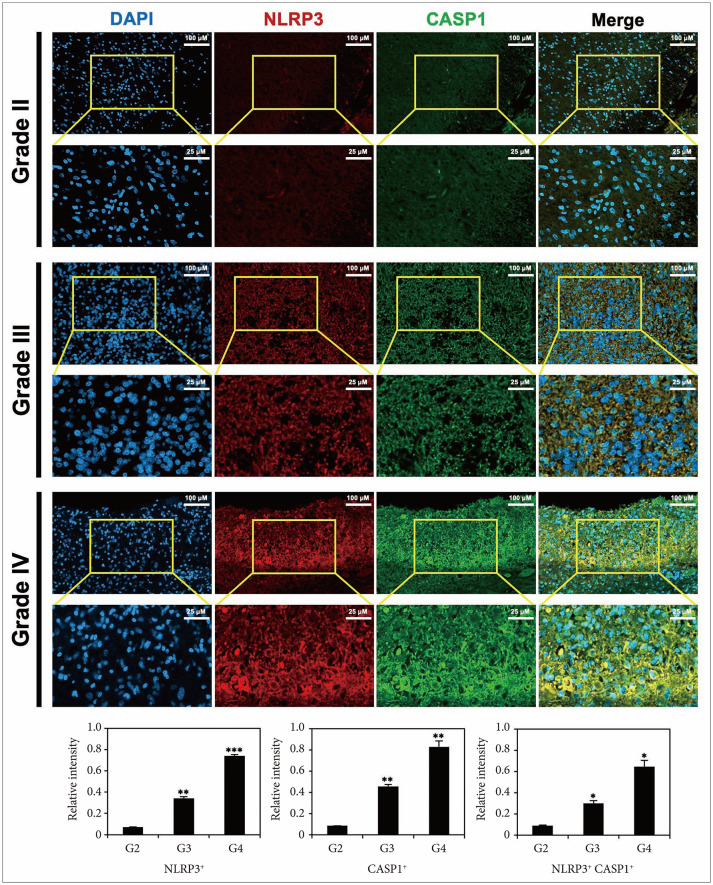
Based on the results of bioinformatics analysis and previous studies, we first performed an immunohistochemical examination, focusing on the canonical NLRP3 inflammasome. Since the tissues used in this study were diagnosed and obtained before the glioma classification criteria were newly established in 2021, the experiment was conducted by dividing tumor grades according to the previous criteria. After classifying tissues from glioma patients into grades II–IV, we compared the expression levels of NLRP3 and caspase-1, which were significantly increased 5-fold in grade III and 10-fold in grade IV, respectively, compared to those in grade II (Fig. 2). The co-expression of these molecules was also upregulated from 0.09±0.003 (grade II) to 0.3±0.026 (grade III) and 0.65±0.059 (grade IV). This result is consistent with a previous study showing that the NLRP3 inflammasome is involved in the malignancy of glioma [29].
Expression of non-canonical inflammasome-related molecules is upregulated with increasing glioma malignancy
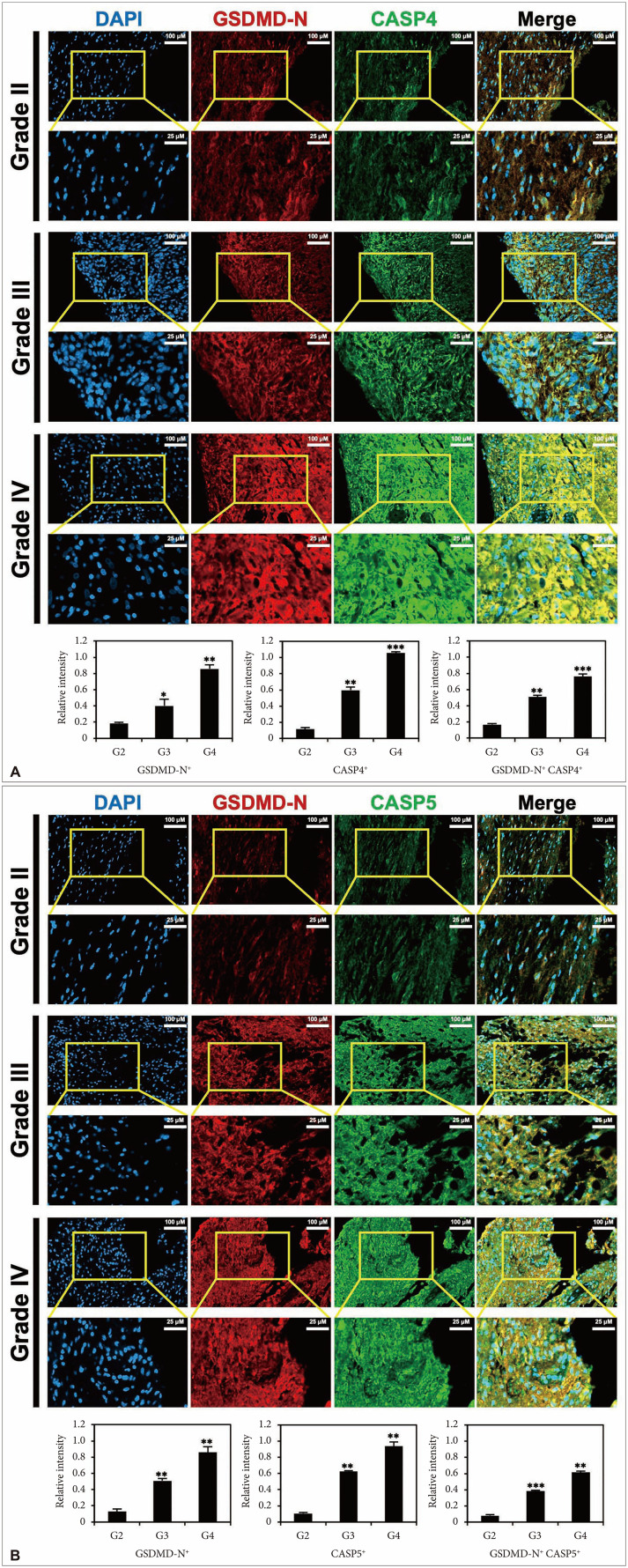
In humans, caspase-4 and caspase-5 are involved in GSDMD cleavage via the non-canonical inflammasome pathway [3031]. Therefore, we confirmed the expression patterns of N-form GSDMD, caspase-4, and caspase-5, which are key non-canonical inflammasome molecules, in glioma tissues by grade.
The expression level of both the N-form GSDMD and caspase-4 increased by at least 2-fold and up to 10-fold in grades III and IV, respectively, based on grade II (Fig. 3A). In addition, the co-expression of the N-form of GSDMD and caspase-4 significantly increased from 0.17±0.012 (grade II) to 0.51±0.022 (grade III) and 0.76±0.029 (grade IV). Additionally, as shown in Fig. 3B, the expression level of caspase-5 also increased by 6–9 times as the grade of glioma increased. Moreover, the co-expression of the N-form of GSDMD and caspase-5 was upregulated from 0.13±0.03 (grade II) to 0.51±0.029 (grade III) and 0.86±0.069 (grade IV).
These results suggest that non-canonical inflammasomes are associated with glioma malignancy (Fig. 1).
The features of pyroptosis associated with inflammasome expression increase with glioma malignancy
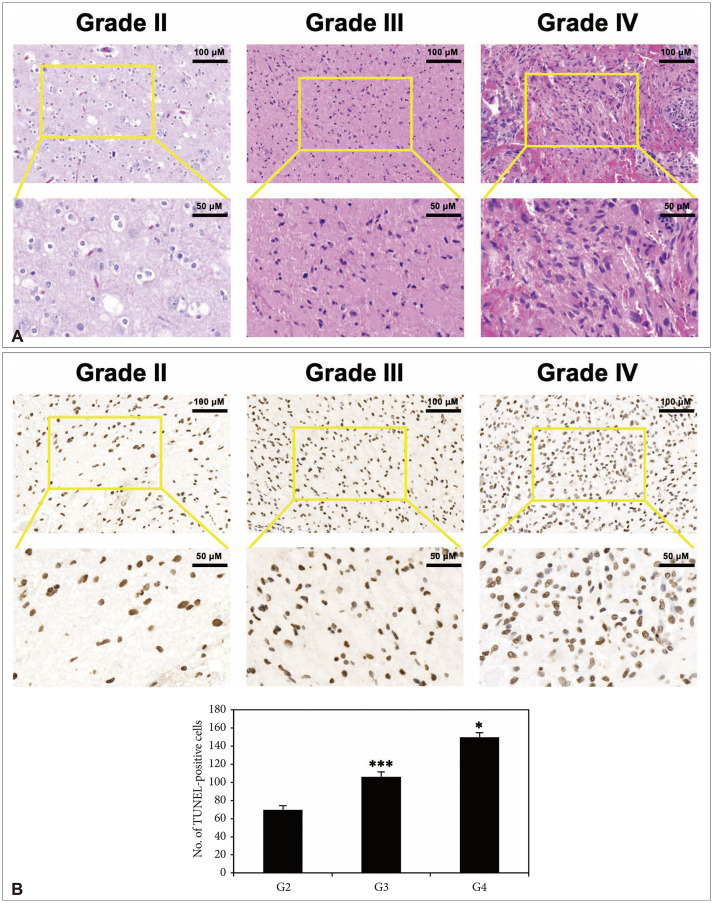
Previous studies have shown that oligomerization of N-form GSDMD causes pyroptosis by forming pores in the cell membrane [32], and the features of pyroptosis are identified by grade in glioma tissues.
H&E staining was performed for each grade of glioma tissue. We confirmed that cell density increases with malignancy, especially in grade IV, and we observed features of an inflammatory tumor microenvironment, such as vascular formation, irregular mitosis, and spindle-shaped cells with anaplasia (Fig. 4A). Next, apoptotic cells were measured using the TUNEL assay, and the frequency markedly increased according to malignancy (Fig. 4B).
DISCUSSION
Although numerous studies have been conducted to overcome the poor prognosis of glioma and to develop effective treatments, it is still classified as an intractable cancer owing to its aggressive nature, including its onset location, heterogeneity, and invasiveness [744]. This aggressive nature has been found to be induced by the inflammatory microenvironment [45]. Proinflammatory cytokines, such as IL-6, IL-18, IL-1β, and TNF-α, play a key role in inflammation and are involved in a wide range of inflammatory diseases, particularly in stimulating the growth and proliferation of cancer cells [4647]. Inflammation is initiated by the activation of inflammasomes [48]. Initially, it was assumed that all NLRPs belonging to the host pattern recognition receptor form caspase-1-activating inflammasomes, and this was known as the canonical pathway. However, as research progressed, it was confirmed that only specific NLRPs work, and that other NLRPs and non-NLRPs can also assemble canonical inflammasomes [25]. Currently, it is accepted that inflammasome activation can be achieved in two main ways: 1) by canonical pathways that signal through the formation of caspase-1 activating inflammasomes and 2) by non-canonical pathways that function through inflammasome-independent mechanisms or alternative caspases [49]. To date, a total of seven pathways have been identified, including the canonical NLRP1/NLRP3/NLRC4/AIM2/IFI16/pyrin inflammasomes and the non-canonical inflammasome [2627].
The most studied canonical NLRP3 inflammasome is a multiprotein complex of the innate immune system that is responsible for initiating the inflammatory response by releasing IL-18 and IL-1β [24]. Previous studies have shown that the NLRP3 inflammasome contributes to the progression of malignant central nervous system cancers, such as GBM [36]. In addition, NLRP3 and NLRC4 are highly correlated, and upregulation of the NLRC4 inflammasome has been confirmed to contribute to the poor prognosis of glioma patients [50]. However, more detailed studies are needed on the correlation between the glioma and non-canonical inflammasome, which is different from the canonical manner. Accordingly, this study focused on identifying the role of the non-canonical inflammasome in gliomas.
Bioinformatics analysis revealed that the expression of GSDMD, caspase-4, and caspase-5, which are non-canonical inflammasome-related molecules, and caspase-1, which is involved in both canonical and non-canonical manners, increased with glioma malignancy and negatively affected patient survival. These results were verified in glioma tissues through immunohistochemical examination, and NLRP3, GSDMD, and caspase-1/4/5 were all significantly upregulated with increasing tumor malignancy.
GSDMD is a common substrate for caspase-1/4/5 and, upon cleavage, oligomerizes to form pores in the cell membrane, resulting in pyroptosis [3151]. The initiation of pyroptosis leads to the release of the inflammatory mediators IL-1β and IL-18, which can promote cancer occurrence and growth in various ways [43]. According to the data of this study, the features of pyroptosis, which increased as the grade of glioma increased, were also confirmed through H&E staining and the TUNEL assay. This suggests that the expression of canonical and non-canonical inflammasomes generated in gliomas can contribute to the formation of an inflammatory tumor microenvironment by inducing pyroptosis.
Summarizing the results of this study together with the inflammasome pathways revealed in previous studies [2552], activated caspase-1/4/5 in glioma cells cleaves GSDMD into N- and C-forms, and the N-form GSDMD oligomerizes to create pores in the cell membrane, inducing pyroptosis. Through this process, pro-IL-18 and pro-IL-1β mature and are released extracellularly, thereby contributing to the formation of an inflammatory microenvironment. In addition, the N-form GSDMD may be involved in the activation of the canonical NLRP3 inflammasome, suggesting that canonical and non-canonical inflammasomes complement each other (Fig. 5). Additionally, our previous study revealed that the binding of T cell immunoglobulin and the mucin-domain containing-3 (Tim-3), a representative immune checkpoint molecule in glioma, and its ligand, gal-9, induces the NLRC4 inflammasome [53]. Tim-3/gal-9 showed a positive correlation with NLRC4 and caspase-1, and their expression increased with glioma grade and was associated with poor survival in patients with glioma [53]. The inflammasome is also associated with T cell-related immune responses and can affect the inflammatory tumor microenvironment in various ways, and its control can be used for the treatment of glioma.
This study confirmed that canonical and non-canonical inflammasomes contribute to glioma malignancy and poor patient prognosis. These findings may lead to a more sophisticated understanding of the glioma microenvironment and suggest potential as novel molecular aggressiveness markers. Our study is not without its limitations, so further research is needed. Further studies are needed to determine whether downregulation of the non-canonical inflammasome can inhibit glioma cell activity or cell-to-cell interactions. In addition, the causal relationship between the cofactors involved in the generation of inflammasomes, the effect of inflammasome regulation on normal brain cells, and the side effects of the immune system should be explored to improve the outcomes of chemotherapy.
 XML Download
XML Download