

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
South Korea has had the highest suicide mortality rate among the 35 members of the Organization for Economic Cooperation and Development (OECD) since 2003.1 Unfortunately, suicide has been the leading cause of death among adolescents in South Korea for 10 years, with the exception of 2014.2 In addition, in the Korea Youth Risk Behavior Web-based Survey in 2019, 13.1% of students reported having serious thoughts of suicide in the past 12 months.3 To address the serious mental health issue of suicide among youth, an approach that enables the dissemination and understanding of suicide prevention to youths is needed.4
Based on World Health Organization (WHO) statistics, in Europe, where suicide is the number one cause of death among adolescents and young adults aged 15–24, the establishment of a national suicide prevention program was discussed in 2005.5 However, problems have been identified regarding the development of unsystematic and unverified suicide prevention programs.
A warning sign of suicide is an indicator that a person could be in acute danger and requires immediate assistance.6 In the United States, it was reported that more than 80% of adolescents who committed suicide informed others of their plans of suicide attempts one week before death and that more than 90% reported clear warning signs of suicide.7 According to a prior study,8 warning signs may signal an imminent suicide as well as a potential suicide risk over a relatively long period of time.8 In addition, it has been confirmed that warning signs appear more prominently in individuals who commit suicide who had previously received a psychiatric diagnosis. In a previous study, psychological autopsy was performed on parents, friends, and acquaintances of adolescents who committed suicide in Utah, USA.9 As a result of a study on the warning signs and behavioral changes that the deceased adolescents showed before suicide, they reported that parents were more likely to identify emotional problems, friends were more likely to identify behavior and relationship problems, and those around them, such as teachers, were more likely to better identify relationship problems. The common warning signs include self-harm and suicidal thoughts, obsession with death, completion of death-related documents such as wills, sudden changes in behavior or eating and sleep patterns, feelings of guilt, and poor performance at school or work.10 However, warning signs for suicide in children and adolescents include many factors related to depressive symptoms, which are relatively common and nonspecific in general students without suicidal thoughts; therefore, it is not easy to identify direct signs of the suicide risk of students in school.11 In the United Kingdom, approximately 30 percent of 544 young people who committed suicide from 2014 to 2016 had no known history of recent adverse life events, self-harm, or suicidal ideas.12 Particularly, in South Korea, a recent study found that teachers could only notice 20.6% of deceased students’ warning signs, which meant that students’ psychiatric problems were not well recognized before their suicides.13
In addition, little is known about the relationship between a history of psychopathology and suicide among children and adolescents. According to previous research with 101 hospitalized children and adolescents, a history of suicide attempts was directly associated with physical abuse and indirectly related to emotional abuse.14 Internalizing disorders predict suicidal thoughts; however, their co-occurrence with externalizing disorders significantly elevates the probability of eventual suicide.15 Therefore, identifying psychometric profiles and risk factors could help prevent suicidality among youths.14
Until now, no warning signs for suicide have been identified to predict who is at imminent risk for suicide with enough specificity and sensitivity.13 Teachers’ understanding of the warning signs and characteristics of children’s and adolescents’ suicide are necessary for suicide prevention. Therefore, our study aimed to identify the different warning signs among Korean students who committed suicide according to their psychopathology characteristics based on 5 years of retrospective cohort data from student suicide reports written by teachers.
This study aimed to analyze the features of suicidal warning signs of Korean students with different psychometric profiles before their deaths based on teacher reports. The following research questions guided our study:
1) What were the demographics and school-related factors of students who committed suicide? Also, what were the characteristics of students based on the symptomatic versus nonsymptomatic group as defined by the SDQ?
2) Would an LCA (Latent Class Analysis) analysis based on SDQ (Strengths and Difficulties Questionnaire) scores identify the types of students who committed suicide? How would the characteristics of students who committed suicide be classified based on LCA?
3) Were the warning signs that appeared in the students near the time of their death based on the types of students who committed suicide as confirmed by LCA?
METHODS
Participants
The present study was a retrospective cohort study of the Student Suicide Report Form completed to record suicidal deaths of students in Korea from 2017 to 2020. The Ministry of Education in Korea developed the Student Suicide Report Form to evaluate risk factors related to school life among suicide victims. Since 2015, all elementary, middle, and high schools have been required by the Ministry of Education to submit an annual ‘Student Suicide Report’ to the Office of Education and Ministry of Education. When a teacher recognizes that a student’s death was a suicide, he or she submits the student suicide report (including the teachers’ observations in school, parental reports of the death, and information in the official school records) to the Ministry of Education.13 The form includes teacher-reported information on each incident of a child’s or adolescent's suicide death. The prior study showed the detailed survey items.16
The study data were obtained from the Ministry of Education in Korea. Data were collected for each case by reviewing teachers’ forms of suicides in children and adolescents. A total of 546 cases of student suicide were reported from 2017 to 2020. After 18 cases were excluded due to missing data, 528 cases were ultimately included in the analysis.
Measures
Demographic factors
The report items include the student's gender, type of school (elementary, middle, and high school), and family type (parents, single parents, and others). The socio-economic status (SES) was classified into three groups (high, middle, and low). In addition, emotional behavior problems, physical illness, mental illness, trigger events, self-harm experience, suicide attempts, the record of attendance, conduct problems, depressive symptoms, anxiety, impulsiveness, and social problems were assessed. Two response options were provided: “yes” or “no.”13
Strengths and Difficulties Questionnaire (SDQ)
The report form includes a total of 25 items from the Korean version of the SDQ for teacher reporting developed17 and translated into Korean.18 The SDQ is a scale composed of a total of five subscales, including ‘prosocial behavior,’ which is a strength, and ‘hyperactivity,’ ‘emotional symptoms,’ ‘conduct problems,’ and ‘peer problems,’ which are difficulties. The total score for each subscale ranges from 0 to 10. According to the interpretation guidelines for each subscale for teacher reporting, the total score is calculated by adding up the scores for all five subscales, and then it is interpreted. Based on the total score, a score of 0 to 11 is interpreted as ‘normal,’ a score of 12 to 15 as ‘borderline,’ and a score of 16 to 40 as ‘abnormal.’ In our study, the sample was divided into a normal group, a borderline group, and an abnormal group.18 For analysis, the groups were reclassified as symptomatic and nonsymptomatic groups. In our study, the internal consistency value for the SDQ was 0.761.
Warning signs of suicide
Warning signs for students who died by suicide consisted of three subfactors (verbal, behavioral, and emotional signs).10 The warning signs were reported by the teacher of the deceased student and included any observed changes in the student’s verbal, behavioral, and emotional signs prior to committing suicide.19 According to the previous research, the warning signs were classified into a total of 20 items, including 7 verbal signs, 11 behavioral signs, and 2 emotional signs.2021
The detailed warning signs of suicide were as follows: verbal signs (talking about suicide or death frequently, complaining about physical discomfort, saying they feel worthless or alone, asking questions about how to commit suicide, speaking of longing for the afterlife, talking about people who have committed suicide, and writing down death-related information), behavioral signs (changes to sleeping patterns and eating habits, putting affairs in order, planning for suicide, loss of interest in personal hygiene or appearance, acting differently than usual or not completing a given task, being distracted, difficulty making decisions about trifles, self-harm behavior or substance abuse, and being preoccupied with death-related music, writing, or movies), and emotional signs (displaying extreme mood swings and withdrawing or feeling isolated).10 In our study, the internal consistency value for the warning signs of suicide was 0.753.
Data analysis
We conducted frequency analysis, multiple response analysis, the χ2 test, and the t test to examine the demographic characteristics and school-related factors of students who died by suicide. In addition, LCA was performed to confirm the types of students according to the characteristics of the students who died by suicide. LCA was used to identify subgroups (classes) of respondents and to capture heterogeneity associated with latent or unobserved subpopulations.22 All data analyses were performed using IBM SPSS Statistics 23 (IBM Corp., Armonk, NY, USA) and Mplus ver. 8.6.
RESULTS
Demographic characteristics of the subjects
Based on the SDQ total score, the group was divided into a nonsymptomatic group (n = 411) and a symptomatic group (n = 117), and a cross-analysis and χ2 test were performed. In the nonsymptomatic group, there were 213 (51.8%) boys and 198 (48.2%) girls, with 3.65% more boys than girls in the group. In the symptomatic group, there were 58 (49.6%) boys and 59 (50.4%) girls. In addition, a χ2 test was performed to test whether the observed frequency between the total difficulty group and gender was significantly different. There was no statistically significant difference (χ2 = 0.185, P = 0.667).
Regarding the type of school, the nonsymptomatic group consisted of 19 elementary school students (4.6%), 128 middle school students (31.2%), and 264 high school students (64.2%), and the symptomatic group consisted of 3 elementary school students (2.6%), 46 middle school students (39.3%), and 68 high school students (58.1%). In both the nonsymptomatic group and the symptomatic group, the highest percentage of students were high school students. The association between the total difficulty scale of the SDQ and the type of school showed no statistically significant difference between groups (χ2 = 3.314, P = 0.191).
Regarding family type, the proportion of students living with both parents was more than 70% in both the nonsymptomatic group and the symptomatic group (χ2 = 6.428, P = 0.040). In terms of the difference in SES according to the groups, the symptomatic group had a lower SES level than the nonsymptomatic group, and the difference between the groups was statistically significant (χ2 = 8.981, P = 0.011). Compared to the nonsymptomatic group, the symptomatic group complained of significantly more difficulties with emotional behavior (χ2 = 112.543, P < 0.001).
In addition, the symptomatic group had a significantly higher proportion of reports of physical illness (χ2 = 9.320, P = 0.002). The major physical illnesses that were reported were atopy, epilepsy, rhinitis, asthma, and hypotension. In terms of mental illness, the symptomatic group had a significantly higher percentage of reports of mental illness (χ2 = 100.045, P < 0.001). The detailed reports of mental illness included depression, attention deficit hyperactivity disorder (ADHD), bipolar disorder, schizophrenia, and panic disorder.
The examination of the difference in the presence or absence of trigger events between groups showed that the symptomatic group had trigger events at a 12.1% higher rate than the nonsymptomatic group (χ2 = 3.967, P = 0.046). Furthermore, the symptomatic group had a higher rate of self-harm experiences than the nonsymptomatic group by 27.6%, and the difference was found to be statistically significant (χ2 = 43.294, P < 0.001). Regarding suicide attempt experience, the symptomatic group had an 18.3% higher rate of suicide attempts than the nonsymptomatic group, and there was a statistically significant difference between the groups (χ2 = 26.890, P < 0.001). Furthermore, there were statistically significant differences between the two groups in the record of attendance (χ2 = 78.612, P < 0.001), conduct problems (χ2 = 25.641, P < 0.001), depressive symptoms (χ2 = 71.896, P < 0.001), anxiety (χ2 = 64.935, P < 0.001), impulsiveness (χ2 = 78.347, P < 0.001), and social problems (χ2 = 52.692, P < 0.001) (Table 1).
Table 1
Demographic characteristics of the subjects (N = 528) by SDQ scores
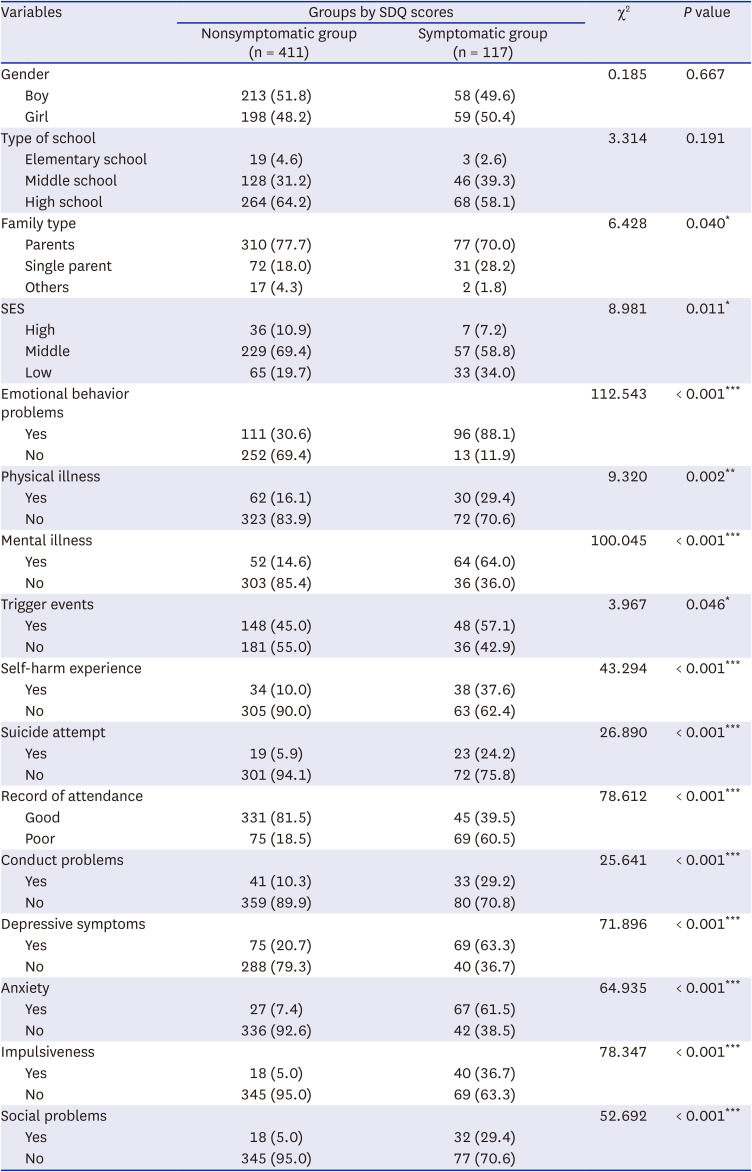
The total number of each variable varies due to missing values; however, the total numbers of members of each group are as follows: nonsymptomatic group = 411, symptomatic group = 117.
SDQ = The Korean version of the Strengths and Difficulties Questionnaire, SES = Socio-economic status.
*P < 0.05, **P < 0.01, ***P < 0.001.
Measures of LCA model fit
To identify the types of student suicide deaths, LCA was performed based on the SDQ scores of students who committed suicide from 2017 to 2020. To establish the optimal latent class model, the analysis was estimated 3- to 5-class models. However, the results of the Lo-Mendell-Rubin Likelihood Ratio Test, which shows whether one latent model (n) is statistically more suitable than another latent model (n-1), were not significant in all layers. Nevertheless, the Akaike information criterion, Bayesian information criterion (BIC), and adjusted BIC showed that the entropy, which refers to the quality of the classification with the lowest information index as the number of latent layers increases, was the best in the 4 latent layer model (entropy value = 0.938). Therefore, in this study, 4 latent hierarchical models were selected and analyzed (Table 2).

SDQ detailed scores and content for each class classified based on LCA
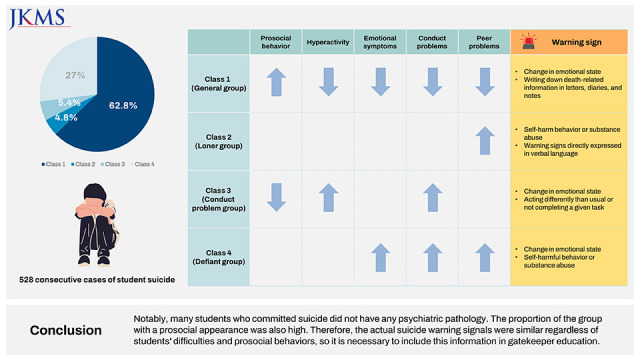
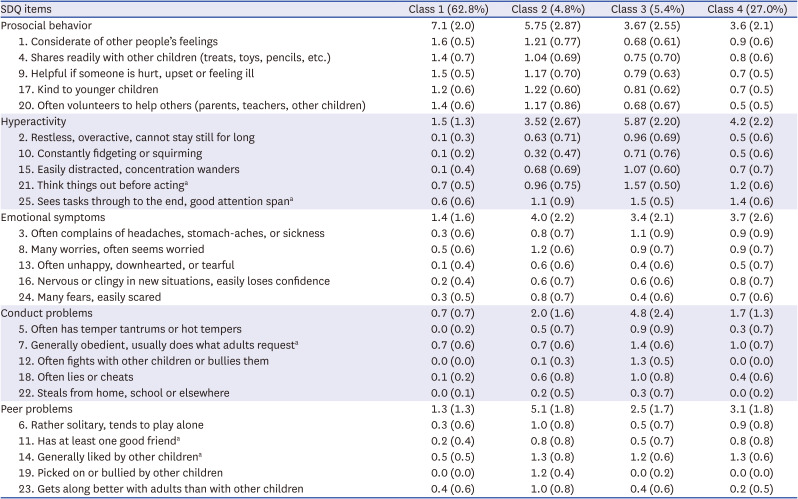
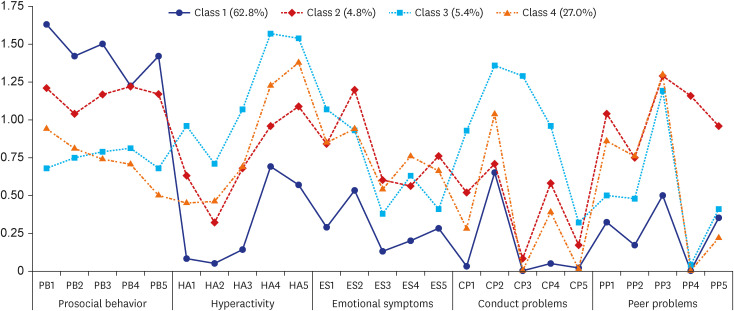
The SDQ detailed scores and questionnaires were presented for each class classified based on LCA. In detail, Class 1 (62.8% of the total) showed a high score for prosocial behavior; however, it had low scores for all four difficulties (hyperactivity, emotional symptoms, conduct problems, peer problems). Class 2 showed moderate strength, especially for peer problems (e.g., picked on or bullied by other children, gets on better with adults than with other children). On the other hand, Class 3 showed overall low prosocial behavior, a high level of hyperactivity (e.g., restless overactive, cannot stay still for long, easily distracted, concentration wanders), and conduct problems (e.g., often fights with other children or bullies them, steals from home, school or elsewhere, often has temper tantrums or hot tempers). Finally, in Class 4, emotional symptoms (e.g., nervous, or clingy in new situations, easily loses confidence), conduct problems (e.g., generally disobedient, not doing what adults normally do), and peer problems (e.g., children usually do not like, rather solitary, tends to play alone) were reported at high levels. Therefore, Class 1 was named the ‘general group,’ Class 2 was named the ‘loner group,’ Class 3 was named the ‘conduct problem group,’ and Class 4 was named the ‘defiant group’ (Table 3, Fig. 1).
Table 3
SDQ items for each class classified based on Latent Class Analysis
The characteristics of students who died due to suicide for each class classified based on LCA
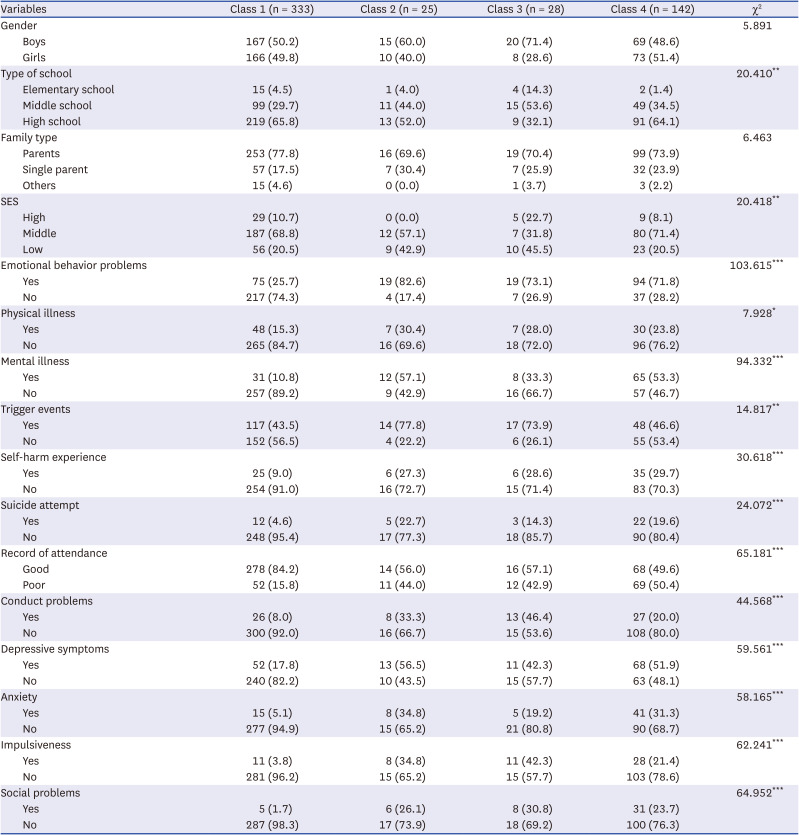
The characteristics of students who committed suicide were divided into individual and relational dimensions, and the four classes were compared through cross-analysis. Differences between the four classes and individual characteristics of the deceased showed statistically significant differences in school type (χ2 = 20.410, P < 0.01), SES (χ2 = 20.418, P < 0.01), emotional behavior problems (χ2 = 103.615, P < 0.001), physical illness (χ2 = 7.928, P < 0.05), mental illness (χ2 = 94.332, P < 0.001), trigger events (χ2 = 14.817, P < 0.01), self-harm experience (χ2 = 30.618, P < 0.001), suicide attempt experience (χ2 = 24.072, P < 0.001), record of attendance (χ2 = 65.181, P < 0.001), behavioral problems (χ2 = 44.568, P < 0.001), depressive symptoms (χ2 = 59.561, P < 0.001), anxiety (χ2 = 58.165, P < 0.001), impulsivity (χ2 = 62.241, P < 0.001), and social problems (χ2 = 64.952, P < 0.001) (Table 4).
Table 4
The characteristics of students who committed suicide for each class classified based on Latent Class Analysis
The characteristics of Class 1
In the case of Class 1, the majority of deceased students, 65.8%, were found to be high school students, with this group showing the highest percentage of high school students compared to the other three groups. In terms of gender, there were similar proportions of boys and girls, with 50.2% and 49.8%, respectively, and the middle level of SES had the highest proportion of students, at 68.8%. Most of the students showed good attendance at school before death (84.2%), and there were no conduct problems (92.0%). In Class 1, emotional and behavioral characteristics such as depressive symptoms, anxiety, impulsivity, and social problems were also confirmed to have not been observed in the majority of students, ranging from 82.2% to 98.3%. Overall, the students belonging to Class 1 did not show any particular school maladjustment or emotional behavior problems during their lifetime.
The characteristics of Class 2
In Class 2, boys accounted for 60%, which was higher than girls, and high school and middle school students accounted for 52% and 44%, respectively. Additionally, 57.1% of students were in the middle SES level. It was confirmed that more than half of students in this class did not show any problems with attendance during their lifetimes, but 44% of students did have problems with attendance, such as absenteeism and early departure. In addition, 33.3% of students had conduct problems. Furthermore, the number of students who showed depressive symptoms during their lifetimes reached 56.5%, which was the highest level among the remaining three classes. On the other hand, anxiety, impulsivity, and social problems were to be present in 26.1% to 34.8% of students, which was relatively lower than the rate of depressive symptoms, but it was confirmed that the students still had psychiatric problems.
The characteristics of Class 3
In Class 3, boys accounted for 71.4%, which was more than twice the proportion of girls, and it was found that the proportion of boys was the highest compared to the other three classes. Regarding the type of school, middle school students accounted for more than the majority at 53.6%, and the lowest level of SES had the highest proportion of students, at 45.5%. In particular, 42.9% and 46.4% of students had problems with attendance and conduct during their lifetimes, respectively. For emotional-behavioral problems, only 19.2% of students had anxiety-related problems. On the other hand, depressive symptoms and impulsivity were observed in 42.3% of students each, nearly half of the students had mental illness problems, and social problems were also observed in 30.8% of students.
The characteristics of Class 4
Class 4 included 51.4% girls and 48.6% boys. Regarding SES, the majority of students were in the middle level, at 71.4%. In addition, high school students were the most common, representing 64.1% of the group. In particular, in this group, 80% of the students did not show any behavioral problems during their lifetime. On the other hand, with regard to attendance, 50.4% of students showed problems such as early departure or absenteeism. Additionally, in terms of emotional and behavioral problems, 51.9% of students complained of depressive symptoms during their lifetimes, followed by anxiety symptoms, at 31.3%; social problems, at 23.7%; and impulsivity, at 21.4%.
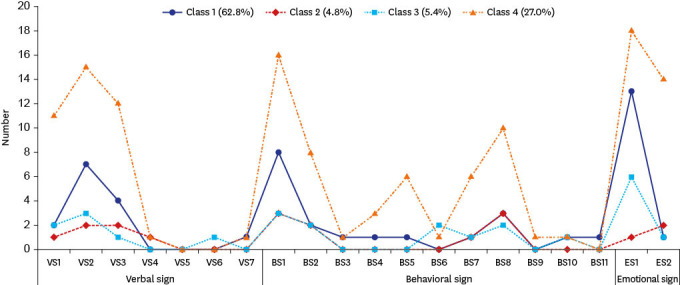
Warning signs by type of student who committed suicide
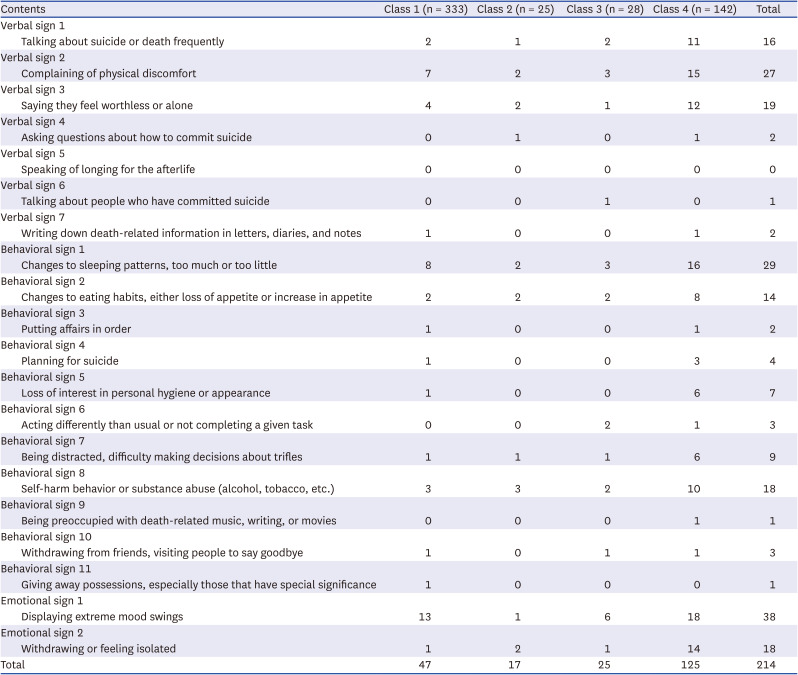
Based on the 4-class model of students who committed suicide confirmed through LCA, the verbal, behavioral, and emotional signs that appeared in the students near the time of their death by suicide are presented by class (Table 5, Fig. 2).
Table 5
Warning signs by type of student who committed suicide
Warning signs of Class 1
In Class 1, ‘Emotional sign 1: Change in emotional state’ was found in a total of 13 students, indicating that it was the warning sign most frequently identified by teachers. In addition, ‘Behavioral sign 7: Writing down death-related information in letters, diaries, and notes’, a sign that was not observed in other classes, was observed in Class 1.
Warning signs of Class 2
The most observed behavioral change near death in Class 2 was 'Behavioral sign 8: Self-harm behavior or substance abuse (alcohol, tobacco, etc.)’, which was observed by a total of 3 students, showing that it was identified as a key warning sign. In addition, warning signs directly expressed in language such as ‘Verbal sign 1: Frequently speaking about suicide, murder, or death’ and ‘Verbal sign 4: Asking questions about how to commit suicide’ were observed.
Warning signs of Class 3
In Class 3, ‘Emotional sign 1: Change in emotional state’ was observed in 6 students and was found to be the most frequently reported warning sign of suicide by teachers. In addition, ‘Behavioral sign 6: Acting differently than usual or not completing a given task,’ which was very rare or not observed in other classes, was found to be a highly possible suicide risk index for class 3 students.
Warning signs of Class 4
In Class 4, ‘Emotional sign 1: Change in emotional state’ was the suicide risk index most frequently identified by teachers, with a total of 18 students showing this change during their lifetimes. In addition, ‘Behavioral sign 8: Self-harmful behavior or substance abuse (alcohol, tobacco, etc.)’ was confirmed to be a particularly prominent warning sign in class 3 compared to the other classes. There was a rare case when ‘Verbal sign 7: Writing about death in letters, diaries, notes, etc.’ was observed.
DISCUSSION
We analyzed teachers’ reports on suicide completers in school from 2017 to 2020. In this study, 528 students who committed suicide were classified into four groups based on the SDQ through LCA analysis, for which the psychopathological characteristics and the differences among warning signs were analyzed. As a result of SDQ items for each grade classified according to LCA, 62.8% were in class 1, 4.8% in class 2, 5.4% in class 3, and 27.0% in class 4. This analysis was intended to give teachers additional information in recognizing suicide warning signs.
According to our findings, among students who committed suicide, warning signs were reported for only 40.5% (214 out of 546 cases, including duplicate responses). According to the reports completed by the teachers at school, approximately 60% of the students did not seem to have a ‘problem,’ which shows a limitation in that the explanatory power of warning signs is low. In addition, these results indicate that it is very difficult to identify the suicidal warning signs of students in schools. Warning signs are the first signs that can be seen in a person likely to harm themselves within a short period of time (e.g., within minutes, hours, days, or months) and are distinct from risk factors that predict suicide over relatively long periods of time (e.g., one year). In other words, if a risk factor is comparable to a ‘clue,’ a warning signal is considered to be similar to a ‘red flag.’23 The present study’s findings are similar to previous results indicating that suicides are preceded by warning signs.23 Prior study also showed that we need to be on alert for warning signs that suggest suicidal risk. On the other hand, our findings contrast those of a prior study24 in which warning signs were observed in 93.0% of suicide decedents. A previous study24 was conducted based on the Korea-Psychological Autopsy Checklist for Police Records (K-PAC-PR) for adults. However, since the present study used data for adolescents observed by teachers in the school, there may be differences from other studies. In particular, regarding suicidal warning signs in children and adolescents, there have been very few reports. Above all, the first warning sign might predict suicidal behavior; therefore, identifying the factors that protect against these warning signs are essential.25 Based on this, it could be expected that the findings will increase the understanding of obvious warning signs that are not easy to observe at school.
More importantly, in our study, we clearly showed that there were many cases in which students were observed as normally active students in the school, despite being a student who later committed suicide. According to the SDQ, the nonsymptomatic group of deceased students showed relatively high strengths and low difficulties, and they accounted for approximately 62.8% of the total. In other words, based on teachers’ observations of students at school, approximately 60% of students did not show significant ‘problems or difficulties,’ which overlapped significantly with the approximately 60% of students who did not show warning signs before suicide. This is contrary to the existing literature from the United States that suggests 80% of adolescents at risk of suicide commonly showed warning signs in advance26; therefore, warnings signs should be detectable.27 However, the results can be explained by other possibilities. First, evidence also exists indicating that suicidal students largely go unnoticed and rarely receive formal assistance from schools, mainly due to teachers’ apparent deficit in knowledge of suicide warning signs.28 Second, one of students’ reported barriers to help-seeking behaviors in schools was found to be difficulties in discussing mental health-related concerns with school staff as well as a lack of closeness to school staff.28 Thus, detecting suicidal students by identifying warning signs may involve endogenous limitations in school settings. In particular, the home-based distance learning model has been prevalent due to coronavirus disease 2019, and barriers to identifying at-risk students may be stronger, as the traditional school-based mental health delivery system is based on the in-person system. Therefore, attention to the detection of such signs through the improvement of mental health literacy is needed in school settings to ensure careful observation of at-risk students.
In addition, our study showed that participants who were categorized into the nonsymptomatic and symptomatic groups according to the SDQ showed multidimensional vulnerability in family, school, psychological and social factors. Our finding is consistent with previous research showing that students experiencing school maladjustment (e.g., irregular attendance/truancy, poor academic performance, peer conflict, behavior problems) are known to be at increased risk for suicide.29 Additionally, the present study showed similar results to a prior study that found that suicide among youths was associated with recent stressful events.12133031 As mentioned above, deceased students for whom no warning signs were identified accounted for 60%. However, according to the results of the psychological autopsy of children and adolescents conducted by the authors’ research team, 96.7% of students showed at least one warning sign.10 Based on this, the reasons for the low rate of identifying suicide warning signs observed by teachers in school settings may be explained as follows. First, students may not have shown warning signs at school. Especially, the masked depression of adolescents may often be not recognized because it may be hidden by symptoms not readily identified. Second, a few kinds of warning signs that are difficult to identify in school environments, such as changes in sleep patterns, may exist. As such, some behavioral signs could only be observed in the home or community rather than the school system.16 Third, the warning signs may not have been included in the 20 warning signs we assessed. It should be noted that, in practice, the dynamics through which students fulfill their assigned roles within the school and the processes they perform in the home and social system operate differently.32 Therefore, schools still function as a frontline of defense in mental health crises among students, although not all warning signs can be detected.
In the case of Class 1, the majority of deaths, 65.8%, were found to be among high school students. Most of the students showed good attendance at school before death (84.2%), and there were no conduct problems (92.0%). Overall, the students belonging to Class 1 did not show any particular school maladjustment or emotional behavior problems during their lifetimes. However, the identification of the warning signs of suicide should not be prevented for these reasons. In all cases, close attention and observation should be required.33
In Class 2, boys accounted for 60% of the group, which was higher than girls, and 33.3% of students had conduct problems. Additionally, the number of students who showed depressive symptoms during their lifetimes reached 56.5%. The present study is similar to a previous study24 in which 66.9% of females and 46.7% of males were diagnosed with a psychiatric disorder according to the police records of 13,265 suicide decedents. Furthermore, it was reported that among suicide decedents, the diagnosis of depressive disorder was the most common.24 Early detection and effective intervention of mental health problems such as depression provide an opportunity to reduce the frequency of suicide.34 Therefore, particular caution is required when depressive disorders are present in adolescents.
In Class 3, middle school students accounted for more than the majority, at 53.6%, and 42.9% and 46.4% of students had problems with attendance and conduct during their lifetime, respectively. Depressive symptoms and impulsivity were observed in 42.3% of students each, nearly half of the students had mental illness problems, and social problems were also observed in 30.8% of students. Our results were similar to those of a prior study35 that showed that 1,569 high school students in New York State who felt unsafe at school were at high risk of experiencing suicidal or violent behavior. Interestingly, a previous study36 reported that people with conduct problems or dangerous behavior could engage in suicidal behaviors. Thus, we should pay attention to the various warning signs. Furthermore, these findings could be helpful to develop psychological services to improve the mental health conditions of children and adolescents.22 Thus, it is reasonable to understand that these behaviors and warning signs were clustered together.
In Class 4, in terms of emotional and behavioral problems, 51.9% of students complained of depressive symptoms during their lifetimes, followed by anxiety symptoms, at 31.3%; social problems, at 23.7%; and impulsivity, at 21.4%. In summary, using LCA, we identified four classes of students who committed suicide and demonstrated that some classes were associated with suicide risk and warning signs in adolescents. Most studies focusing on suicide in the youth population made no specific reference to their warning signs and types of students.37 Therefore, to prevent suicide, we should understand the underlying problems of the types of students who commit suicide.
South Korea has established a system and services for suicide prevention and mental health intervention.38 In South Korea, the gatekeeper program was included in the 10 tasks of ‘the 2018–2022 National Suicide Prevention Action Plan’, and the ‘Suicide CARE: version 1.6A’ program for adolescents was developed in 2015.39 The key element of gatekeeper education is to recognize the warning signs of adolescents who are at risk of suicide. As an important suicide prevention strategy, gatekeeper training programs have positive effects on youth at risk for suicide.4041 Although not all people at risk for suicide may show warning signs, school staff, and mental health professionals should have a basic concept of warning signs related to suicide in students, which helps to recognize children and adolescents at risk of suicide in schools.
Of note, teachers play an important role in daily contact with students who are at risk for suicide. Teachers’ understanding of warning signs of suicidal behavior could assist in the identification of students at risk.29 Indeed, the school could offer significant intervention in a timely manner to keep children and adolescents safe from suicide. As reported in a previous study,42 an in-depth study of students having difficulty in school is important since suicidal warning signs could be monitored by teachers in school settings. Indeed, the evidence regarding school mental health literature consistently has emphasized that teachers’ ability to identify early warning signs of suicide plays a strategic role in the early identification of at-risk students and the prevention of suicide. Thus, teachers’ active role in identifying warning signs by monitoring student verbal, emotional and behavioral characteristics to prevent suicide needs to be highlighted in school settings. Overall, this approach would allow schools to play a protective role for children and adolescents and build resilience in students by increasing mental health literacy as well as empathy. In South Korea, schools have established and implemented a system that screens high-risk adolescents for mental health and connects them with professional counselors or psychiatrists, if necessary.32 Based on this, it is required to establish more efficient and systematic suicide prevention policies for children and adolescents in the national system.238
The limitations of this study were as follows. First, our data were based on teacher records. The teachers completing these records may not have been able to provide accurate and detailed information of warning signs. Therefore, our findings suggest that it is necessary to supplement teacher reports of suicide decedents in children and adolescents. In addition, to improve the perception of student suicide prevention, it is necessary to continue to provide suicide-related education systems for teachers. Second, our findings indicated that many of the students who committed suicide were in the nonsymptomatic groups. However, it may consider the possibility that the individual's pathological characteristics could not be revealed or were not observed by others due to cultural factors in Korean society. Thus, it needs to be verified in conjunction with more objective data, such as national data of suicide decedents or psychological autopsy. Furthermore, it is necessary to improve our understanding of deceased students based on an in-depth analysis. To this end, various studies and projects should be conducted based on analysis combined with national data. Nevertheless, our data had the advantage of allowing the analysis of the suicide-related characteristics of domestic children and adolescent suicide decedents.
The present findings could contribute to the development of evidence-based interventions that aim to identify warning signs among children and adolescents and contribute to the reduction of suicide among students. In addition, the perspectives of teachers would be significant for future interventions since they could play a key role in suicide prevention. Furthermore, school-based psychosocial interventions and services should be required to address students at risk and prevent suicides.
 XML Download
XML Download