

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Q fever is an important zoonotic disease caused by Coxiella burnetii. C. burnetii is a Gram-negative and highly pleomorphic coccobacillus. Common reservoirs are livestock such as cattle, sheep, and goats, even though wildlife, pets, birds, and ticks can be infected and shed the microorganism.12345 Human infection by C. burnetii is primarily transmitted through inhalation of aerosolized bacteria from the environment that has been contaminated by birth products or body fluids of infected animals, and infected aerosols can be dispersed up to 5–15 km from the source of infection.67 Person-to-person transmission of Q fever is possible, but seems rare. There was a case of transmission through bone marrow transplantation from an infected donor and a case of nosocomial transmission after delivery in an infected pregnant woman.89 Approximately half of individuals infected with C. burnetii can develop to symptomatic infection.1011 However, Q fever remains as an under-recognized disease because it is usually associated with non-specific symptom such as fever, myalgia, and chills, and has a wide variety of clinical manifestations ranging from an influenza-like febrile illness, to hepatitis, pneumonia, and endocarditis. The most prominent feature distinguishing Q fever from other bacterial infections is that less than 5% of patients with acute C. burnetii infection progress to chronic infection, which manifests as endocarditis or vascular infection.12 Although chronic infection is generally called chronic Q fever, some experts prefer the term persistent localized C. burnetii infection to chronic Q fever.13 In contrast, Q fever in animals, referred to coxiellosis, is usually asymptomatic, but infected female animals can abort in late pregnancy or have stillbirths.14 Infected animals can also shed bacteria through birthing fluids, milk, urine, and feces.
CHANGING EPIDEMIOLOGY OF HUMAN AND ANIMAL Q FEVER IN KOREA
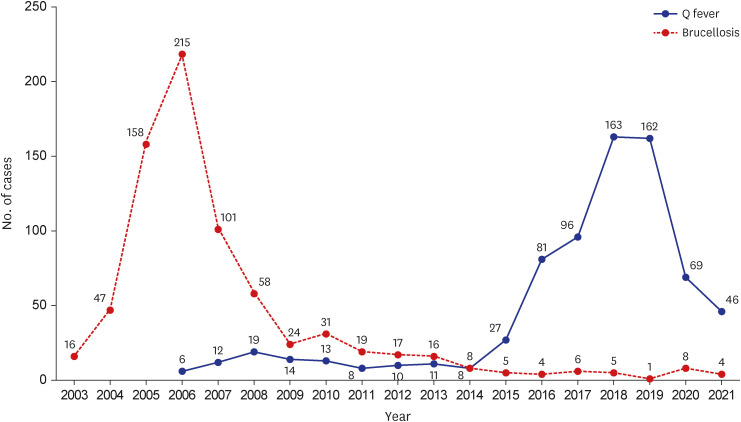
Since human Q fever was designated as the group IV legal infectious disease in 2006, approximately 10 cases per year were reported for several years.15 However, the number of Q fever cases started to increase steeply in 2015, and up to 163 cases were notified in 2018 (Fig. 1). Although the number of notifications has decreased since 2020, it is likely due to the coronavirus disease 2019 pandemic and modification of diagnostic criteria in 2020, rather than to a lower risk of Q fever. In an epidemiological study of Q fever in South Korea, the average incidence rate was as low as 0.07 cases per 100,000 persons per year all across the country from 2011 to 2017, which increased sharply to 0.19 cases per 100,000 persons in 2017.16 Especially, Midwestern areas such as Chungbuk (0.53 cases per 100,000 persons per year) and Chungnam (0.27 cases per 100,000 persons per year) showed a much higher incidence than other areas. One of the epidemiological characteristics of patients with Q fever is that 24% of all reported cases were related to occupational contact with animals or animal products. Among the cases who were not related with occupation exposure, only 18.5% had a history of animal contact.17 This suggests that in most cases, the risk factors associated with Q fever cannot be identified by epidemiological investigation despite it being a zoonosis. In cases of Q fever with a history of animal contact, the common sources of C. burnetii exposure are goats (60.0%) and dairy cattle (32.0%).
Among workers in high-risk occupations with increased animal contact, slaughterhouse workers had a seroprevalence of 1.2% in 2007 and 1.4% in 2012 against C. burnetii.
1819 However, the seroprevalence of C. burnetii in veterinarians working at the Institute of Veterinary Service and Research has risen continuously from 1.0% in 2009 to 4.0% in 2014 and 7.9% in 2019.20 In 2020, another study reported that the seroprevalence of C. burnetii among goat farm workers reached up to 50.8%, based on a phase II IgG antibody titer of ≥ 1:128 measured by indirect immunofluorescence assay (IFA).21
The incidence of animal Q fever based on data from the Korean Animal Health Integrated System, also recently displayed an increasing trend from 14 cases in 2015 to 170 cases in 2021.22 In studies of the seroprevalence of C. burnetii using enzyme-linked immunosorbent assay, the seroprevalence was 7.1–24.2% in dairy cattle and 8.6–19.1% in goats.23242526
Human Q fever is likely to be an underdiagnosed disease because of its non-specific symptoms and diagnostic difficulty that requires tests on paired serum samples collected 4–6 weeks apart.27 Hence, the recent increase in patients with Q fever may be attributed to increased awareness among clinicians and increased number of requests for diagnostic testing. However, it is more likely that the changing incidence of human Q fever is associated with increasing exposure from animal sources, given the increasing trend of animal Q fever and the high seroprevalence of C. burnetii in high-risk occupations.
LARGE-SCALE OUTBREAK OF Q FEVER IN THE NETHERLANDS
In the Netherlands, approximately 4,100 cases of acute or chronic Q fever were diagnosed in southeastern regions between 2007 and 2010, resulting in 19 deaths.28 Before that time, Q fever was a neglected infectious disease that was usually reported as sporadic cases or occasional small outbreaks in most of European countries. To date, the outbreak of Q fever in the Netherlands is the largest on record. In the early stage of the outbreak, the Dutch government took passive actions, such as hygiene measures and voluntary vaccination on farms.29 However, the size of the epidemic continued to grow despite various control measures. After culling all pregnant goats and sheep on infected farms, corresponding to more than 50,000 goats and sheep, the outbreak of Q fever ended. The economic damage related to this outbreak in the Netherlands is estimated to be between €161 million and €336 million.30
Q fever is usually a self-limiting febrile illness of mild or moderate severity. Nonetheless, large-scale outbreaks have led to unprecedented public health issues because approximately 12% of the total population in the Netherlands was found to be residing in areas at risk of C. burnetii exposure during the outbreak of Q fever.6
First, there was an issue concerning the safety of blood and organ donation. The seroprevalence of C. burnetii in outbreak areas was 12.2%, and the true incidence of C. burnetii infection was estimated to be 12.6 times higher than the estimated incidence based on reported cases.31 As C. burnetii can be transmitted via blood, this raised concern about the potential for spread of Q fever through blood donated by individuals with asymptomatic infection.32 Second, diagnosis of chronic Q fever is difficult. In contrast to acute Q fever, the mortality in patients with chronic Q fever is up to 20%, despite appropriate treatment.33
C. burnetii infection can progress to chronic infection within several months or up to 2 years after symptomatic or asymptomatic primary infection.11 Thus, clinical and serological follow-up is required for a certain period even after recovery from acute illness. Chronic Q fever manifests as serious conditions such as endocarditis or vascular infection, that require surgical treatment and long-term therapy for approximately 2 years.3435 Q fever in pregnant women is one of the most critical concerns in outbreak settings.36373839 Women infected during early pregnancy are at risk of developing chronic Q fever. Moreover, C. burnetii infection during pregnancy can lead to abortion, intrauterine growth restriction, or vertical transmission to the fetus.
LESSONS FROM THE EPIDEMIC OF BRUCELLOSIS
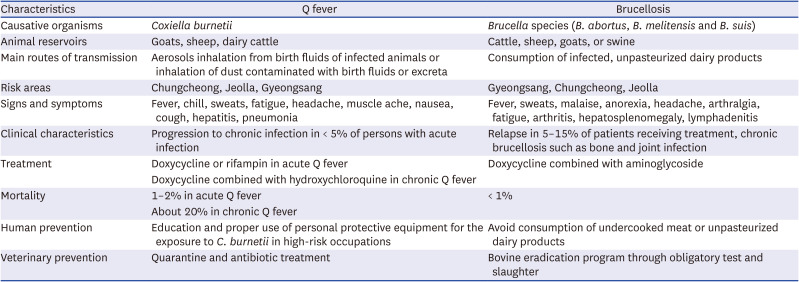
In the early 2000s, South Korea experienced the brucellosis, a zoonotic disease like Q fever, epidemic in humans corresponding to the epidemic in cattle.40 Brucellosis has some features in common with Q fever. The characteristics of human brucellosis and Q fever were presented in Table 1. However, currently bovine brucellosis has almost been eradicated, and consequently, the incidence of human brucellosis has also rapidly decreased.4142 To control bovine brucellosis, compulsory testing for brucellosis has been conducted in Korean native cattle at least once a year, and raw milk and milk bulk tanks on dairy farms are regularly tested for Brucella.43 In addition, it is obligatory to present a Brucella-free certificate whenever trading or slaughtering live cattle. The culling of animals that test positive is economically compensated by the Korean government. This made the policy of compulsory test and slaughter sustainable and effective in controlling bovine brucellosis for a long time in Korea. With the decline in bovine brucellosis, the incidence of human brucellosis could remain to be low in high-risk groups such as livestock workers, veterinarians, ranchers, and abattoir workers.44 This success story in controlling brucellosis suggests that controlling zoonotic diseases in animals serving as sources of infection is key to minimizing transmission to humans.
Table 1
Comparison of clinical characteristics and preventive measures between human Q fever and brucellosis
CHALLENGES TO CONTROL ANIMAL Q FEVER
Currently, the primary way to control animal Q fever in South Korea is quarantine and antibiotic treatment using tetracycline after the diagnosis via an antigen or molecular test, if an animal displays reproductive system symptoms such as abortion or stillbirth.45 Culling can be recommended if an animal has tested positive for Q fever. However, this is not compulsory. In contrast to bovine brucellosis, testing for Q fever in animals is voluntary for farm owners. A symptomatic C. burnetii infection in animals leads to extensive contamination in the farm environments through body secretions or birth products such as placenta, and it can easily spread to other uninfected animals in a herd.46
C. burnetii is highly resistant to external stimuli and common disinfectants.47 Thus, it is possible for it to survive on wool at ambient temperature for 7–10 months.4849 In addition, C. burnetii infection can occur in a broad range of vertebrate and invertebrate hosts including birds, reptiles and ticks, in addition to primary reservoirs such as goats.12450 As an easily spread, highly infectious and ubiquitous organism, C. burnetii has been classified as a category B bioterrorism agent by the US Centers for Disease Control and Prevention.51
To protect humans from C. burnetii, the World Organization for Animal Health (WOAH) emphasizes the need for better surveillance in humans and preventive measures in animals.14 Measures for the control of animal Q fever are preventive vaccination, manure management, segregation of kidding areas, removal of potentially contaminated material, banning visitors, and control of other animal reservoirs and ticks. WOAH anticipates that control of animal Q fever could be effective when different preventive measures are applied using a combined approach. Culling of pregnant animals or shedding herds, and a temporary ban on breeding or animal movement may be an alternative in human Q fever epidemic situations.
THE DIFFERENCE IN THE CONTROL MEASURES BETWEEN BRUCELLOSIS AND Q FEVER
Mandatory testing and slaughter have played a key role in the success of the brucellosis eradication program in South Korea.43 However, it is difficult to apply this policy to other zoonotic diseases. Because human and financial resources for livestock disease control are limited, it is necessary to prioritize zoonotic diseases that require urgent and active control, based on their public health and socioeconomic impact. Although brucellosis and Q fever in humans can have a similar impact on public health, zoonotic diseases between cattle and sheep or goats may have a significantly different socioeconomic impact on the livestock industry. The brucellosis eradication program could be implemented because the brucellosis epidemic had caused major socioeconomic damage to the livestock industry and a major public health impact.5253 Thus, to introduce a mandatory test and slaughter together with economic compensation in Q fever control, such as the countermeasures introduced for brucellosis control, a risk assessment for Q fever is required to assess the national economic and public health impact that could result from an outbreak of Q fever.
Another challenge in controlling Q fever is the diagnosis of Q fever in livestock. WOAH recommends that test results of Q fever should be interpreted at the population level in the context of herd history rather than at the individual level.14 Shedding of C. burnetii in infected animals is usually irregular, and test results can be inconsistent within and between laboratories.545556 Compared to brucellosis, Q fever in livestock shows far higher seroprevalence. Moreover, Q fever diagnosis in an individual animal of a farm can leads to the diagnosis of Q fever at the herd level and not at the individual level. Therefore, it is difficult to introduce proactive countermeasures such as a test and slaughter policy in the management of animal Q fever.
PREPAREDNESS AND RESPONSE TO OUTBREAK OF Q FEVER IN SOUTH KOREA
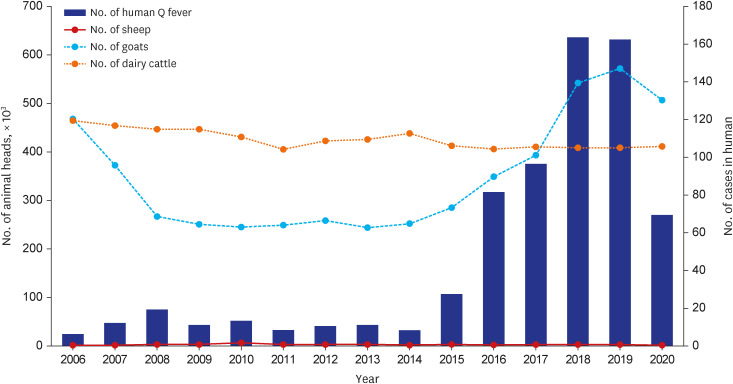
The outbreak of Q fever in the Netherlands was closely associated with a high density of breeding in goat and sheep farms.5758 In the province of Noord-Brabant, which is the center of the dairy goat industry and the focus of the Q fever epidemic in Netherlands, the average number of breeding goats or sheep was more than 600 animals per farm.29 After the epidemics of classic swine fever in 1997 and foot-and-mouth disease in 2001, the total number of goats bred throughout the Netherlands increased to approximately 370,000 in 2009 from approximately 170,000 in early 2000.29 Given the magnitude and major types of livestock on Korean farms, a large epidemic of Q fever, such as the one that occurred in the Netherlands, is less likely in South Korea. However, the number of goats on Korean farms was maintained at around 250,000 until 2015, which increased to more than 350,000 after 2016. The number of goats on the farm was highly correlated with the incidence of human Q fever between 2012 and 2021 (Spearman correlation coefficient [rs] = 0.685, P = 0.029) (Fig. 2). Therefore, it is more likely that small-sized epidemics can occur in suburban areas with high population density, particularly in mid-western Korea, where Q fever is more prevalent.
Fig. 2
Annual number of human Q fever cases, and number of goats, dairy cattle and sheep head in Korea. The incidence of human Q fever is significantly correlated with the number of goats head between 2012 and 2021 (Spearman correlation coefficient [rs] = 0.685, P = 0.029).
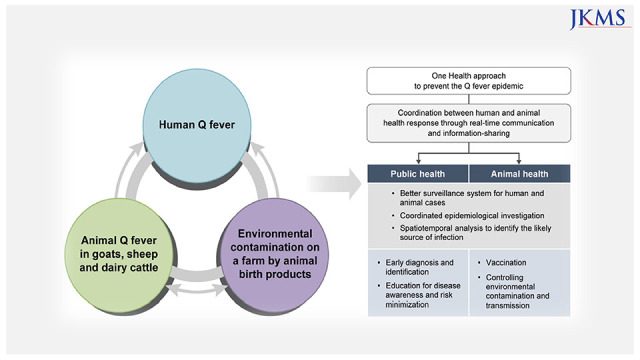
Q fever can be identified in various species of livestock, and the seroprevalence is relatively high at approximately 0.5–25% in dairy cattle and approximately 20% in goats, which implies that the best control strategy is to prevent the progression to a large-scale outbreak of Q fever through early identification, rather than disease eradication. What should be done to prevent Q fever outbreaks in South Korea? Most importantly, to control Q fever outbreaks, a comprehensive and multisectoral One Health approach through a coordinated human and animal response is required.5960 Concurrent human and animal epidemiological investigations are required for human cases to identify the likely source of infection. In outbreaks of human Q fever, epidemiologists can easily access information on livestock farms and animal Q fever that is associated with the cases of human Q fever. Spatiotemporal analysis should be performed in the epidemic area of Q fever to define the transmission route of infection. In addition, information on Q fever on livestock farms needs to be shared with public health officials, physicians, and veterinarians. It is necessary for public health officials to allow real-time communication and information-sharing with animal health officials during the investigation. If an animal source of infection is identified during an outbreak of Q fever, culling of the animals should be considered. In 2022, Korea Disease Control and Prevention Agency (KDCA) had developed the guidance for interdepartmental collaboration in epidemiological investigation of Q fever together with Animal and Plant Quarantine Agency (APQA). KDCA and APQA expect to be able to identify an outbreak of human Q fever earlier and its source of infection in livestock through this collaboration.
It is also necessary to introduce an active surveillance system that can trace the incidence and spread of Q fever in animals. Q fever in animals is generally asymptomatic. Goats and sheep are relatively common livestock, and abortion, stillbirth, and infertility have been reported to be associated with Q fever. Birth products excreted from livestock with symptomatic Q fever can lead to extensive contamination of C. burnetii in farm environments, and can consequently cause the spread of C. burnetii to humans or other livestock in a herd. It is necessary to establish a surveillance system for events such as abortion and stillbirth in goats and sheep.61
As with other communicable diseases, early diagnosis and identification of a suspected case is one of the key components to avoid a large-scale outbreak of Q fever in humans. However, early identification of individuals with Q fever is challenging because of the diagnostic difficulty and the non-specific symptoms and signs. Serologic testing by IFA is most commonly used for diagnosing Q fever in humans. This assay allows a seroconversion rate of less than 50% within 2 weeks after symptom onset.62 To confirm acute Q fever, a fourfold increase in phase II IgG antibody needs to be detected by IFA in paired samples from the acute and convalescent phases, obtained 3–6 weeks apart.63 A negative result in the acute phase cannot rule out acute Q fever because it is not uncommon for the IFA test result to be negative during the early stage of acute infection. Thus, it is crucial for clinicians and public health officials to raise awareness of disease characteristics and to be trained in proper diagnosis in areas endemic for Q fever. There is also an urgent need to introduce a new diagnostic tool, such as real-time polymerase chain reaction, that is more sensitive to enhance diagnostic yield in patients with acute illness and a negative antibody test result.6465
Veterinary vaccines for Q fever should be considered as a preventive measure. Q fever vaccines have been developed for humans and animals. Coxevac®, a non-adjuvanted whole-cell formalin-inactivated veterinary vaccine against the phase I antigen of C. burnetii (Ceva Santé Animale, Libourne, France), is used to lower the spread of C. burnetii infection and reduce the incidence of abortions caused by Q fever in cattle and goats.66 A field study in cattle and goats showed that veterinary vaccine lowered bacterial shedding in infected animals.6768 Currently, the primary control measures against animal Q fever are antibiotic treatment and separating infected livestock in a herd. However, antibiotic treatment for animals with C. burnetii infection is labor-intensive, and veterinarians are at risk of exposure to C. burnetii during antibiotic injection, despite wearing personal protective equipment.46 Therefore, control measures for animal Q fever need to switch from quarantine and antibiotic treatment to the use of preventive vaccines, at least in high-risk areas, taking into account the seroprevalence of C. burnetii in animals.
Despite the surge in human and animal Q fever since 2015, there is a lack of epidemiological data to determine which control measures should be prioritized to prevent outbreaks of Q fever in South Korea. To establish policies regarding Q fever, it is essential to understand the disease burden of Q fever. Specifically, the incidence of chronic Q fever and the seroprevalence of C. burnetii in high-risk groups should be evaluated. It is necessary to determine the prevalence of C. burnetii infection in individuals with culture-negative endocarditis or vascular infection.336970 It is also necessary to monitor trends in antibody titers in the Korean population and to conduct prospective cohort studies to determine the proportion of individuals that progress to chronic Q fever after primary C. burnetii infection.717273
Recently, Q fever has increased among meat processing workers, who are at an increased risk of occupational exposure (KDCA, personal communication, September 30, 2019). It is recommended that samples positive for C. burnetii should be handled in a biosafety level 3 laboratory, and the risk of C. burnetii transmission can be lowered by wearing personal protective equipment such as N-95 masks and goggles when infectious materials or aerosols may be generated in the process of work. Thus, workers in high-risk occupations should be educated about the risk of C. burnetii exposure and the clinical presentation of Q fever. Standard precautions regarding personal protective equipment should be established and non-medical professionals and workers in high-risk occupations should be trained in their use.74
CONCLUSION
While the seroprevalence of C. burnetii has increased in high-risk occupations since the late 2010s, the incidence of human Q fever has increased since 2015, especially in the mid-western area of South Korea. Q fever in livestock has shown an increasing trend since 2016. The Dutch Q fever epidemic highlights the risk of Q fever outbreaks in Korea. Given the potential impact of a Q fever epidemic on public health and socioeconomic loss, enhanced epidemiological investigation and surveillance systems and proactive preventive measures through comprehensive and multisectoral one-health approaches are required to minimize the risk of Q fever epidemic in South Korea. Therefore, a well-coordinated response between public health and animal health officials is critical to prepare for future Q fever outbreaks. It is also necessary to raise disease awareness among clinicians and veterinarians, and to educate workers in high-risk occupations.
 XML Download
XML Download