

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Coronavirus disease 2019 (COVID-19) is a systemic viral infection characterized by clinical symptoms ranging from self-limiting to life-threatening illnesses. Patients with COVID-19 commonly present with upper respiratory symptoms, such as fever, cough, myalgia, headache, and diarrhea.12 Although COVID-19 is a viral infection, it has been reported that many patients are prescribed antibiotics because of concerns about accompanying bacterial pneumonia. While more than 70% of hospitalized patients with COVID-19 were prescribed antibiotics, only 8–9% had bacterial or fungal co-infection.34 In another single-center study, antibiotics were prescribed to 59% of COVID-19 patients, and 29% of patients with mild symptoms who were not receiving oxygen therapy.5 According to an analysis of 10 studies evaluating at least 100 patients,6 bacterial co-infection occurred in < 4% of patients hospitalized with COVID-19. Nonetheless, most of them were prescribed empirical antibiotics.
Unnecessary antibiotic prescription in COVID-19 patients causes collateral damage.7 Side effects of antibiotics include antibiotic-associated diarrhea and rarely fatal adverse reactions, such as arrhythmias.8 Furthermore antibiotic overuse in hospitalized patients leads to increased antibiotic resistance.9
Therefore, we aimed to analyze the number of patients with COVID-19 who received antibiotic prescriptions, as well as factors that contributed to antibiotic prescription requirement, using the National Health Insurance Service (NHIS) database in Korea. In addition, we compared the data of antibiotic use in patients with COVID-19 with those of patients with influenza, which is another representative respiratory viral infection, using an integrated database from Korea Disease Control and Prevention Agency-COVID19-National Health Insurance Service cohort (K-COV-N cohort).
METHODS
Data source and extraction
Using the NHIS database, claims data of adults aged ≥ 19 years who were hospitalized for COVID-19 from January 2020 were obtained, and their data from December 1, 2019 to December 31, 2020 were retrospectively reviewed. Data were provided in the form of sample data and customized data such as general specification details, in-hospital treatment details, disease details, outpatient prescription details, and healthcare facilities information.10 Approximately 80,000 claims data were extracted after requesting the entire medical insurance use history of the target group mainly diagnosed with COVID-19 according to the International Classification of Diseases, Tenth Revision (ICD-10).11 If the same patient was readmitted, only the data from the first hospitalization were included in the analysis, and only hospitalizations with a total length of stay (LOS) ≥ 1 day were selected, excluding cases with errors in each category.
To evaluate factors that may affect antibiotic prescription, information on age, sex, LOS, and medical institutions was obtained, and underlying disease and severity were defined and analyzed. Underlying disease was defined using the Charlson Comorbidity Index (CCI)12 and classified into four groups using a CCI score of 0, 1, 2, or ≥ 3. According to the National Institutes of Health (NIH) guidelines,13 the severity groups were classified as follows: mild to moderate, except for severe to critical cases; severe, oxygen administration group; and critical, in cases of high flow nasal cannula use, mechanical ventilator requirement, and extracorporeal membrane oxygenation application for sepsis, septic shock, respiratory failure, or acute respiratory distress syndrome during hospitalization in the oxygen administration group. In addition, information on each healthcare facility and region (patient’s residence and location of healthcare facility) was checked.
The types of antibiotics prescribed were as follows: aminoglycosides, beta-lactam/beta-lactamase inhibitors, carbapenems, first to fifth generation cephalosporins, fluoroquinolones, glycopeptides, lincosamides, macrolides, metronidazole, monobactams, oxazolinediones, penicillins, polymyxins, sulfonamides, trimethoprim, and tetracyclines. The amount of antibiotics usage was evaluated as days of therapy (DOTs) per 1,000 patient-days, and the proportion of patients who received antibiotics was also calculated.
In addition, we reviewed the antibiotic use of patients hospitalized from 2018 to 2021 for influenza infection, another representative respiratory viral infection, as well as that of patients with COVID-19 from October 2020 to December 2021, using an integrated database from K-COV-N cohort. Since the timing of provision of patient with COVID-19 was partially adjusted during the database integration process of the two institutions, data from October 2020 to December 2021 were obtained. To compare antibiotic use in patients with COVID-19, DOTs per 1,000 patient-days and the proportion of patients prescribed antibiotics were also analyzed among patients with influenza. During the study period, all patients with domestically confirmed COVID-19 were hospitalized, whereas most patients with influenza were treated at community primary medical institutions, and most cases requiring hospitalization were assumed to be severe. Considering these differences in hospitalization indications, a subgroup analysis was conducted on patients with severe to critical COVID-19 and on total patients with influenza.
Statistical analysis
Differences were analyzed using mean comparison (Student’s t-test), analysis of variance, or χ2 test between groups, and confounding variables, such as age, sex, underlying disease, and severity, were further corrected. In the χ2 test, if the significance probability was < 0.0001, the correlation was evaluated by the Cramer’s V value (> 0.25: very strong; > 0.15: strong; > 0.10: moderate; > 0.05; weak; and > 0; no or very weak).14 For trend analysis of monthly antibiotic usage, two-sided correlated seasonal Mann–Kendall nonparametric tests were performed. If there was a trend, the sign of the tau value was used to evaluate whether the trend was decreasing or increasing (tau > 0: increasing trend). The degree of trend was confirmed using Sen’s slope (lower, upper means 95% confidence interval).15 In addition, we investigated the factors contributing to antibiotic use using linear regression analysis. Statistical analysis was performed using R version 4.1.1 (R Core Team, Vienna, Austria) and Python statistical software (version 3.7.4).
RESULTS
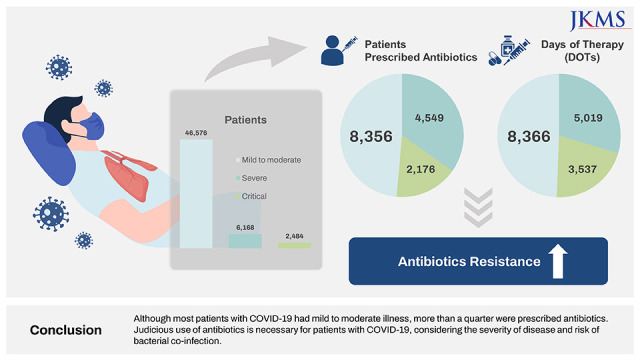
A total of 55,228 hospitalizations were analyzed (Fig. 1). As shown in Table 1, 53.4% of the patients were females, and approximately 90% had no underlying disease (CCI: 0). The median age was 52 (interquartile range [IQR]: 36–64) years, and patients in their 50s or older accounted for approximately 55.9% (n = 30,886) of the study population. Most cases (n = 46,576; 84.3%) were classified as mild-to-moderate. There was no difference in severity according to sex, but severity increased with age. Approximately 90% of patients in their 50s or older accounted for severe and critical cases, with a very strong correlation (Cramer’s V value: 0.30). In mild-to-moderate cases, the proportion of patients with CCI ≥ 3 was only approximately 3.4%; however, the higher the severity, the stronger the correlation (Cramer’s V value: 0.18). There were weak or no correlations between the other variables (Cramer’s V value: < 0.1), except for the relationship between CCI and age (Cramer’s V value: 0.22) and healthcare facilities (Cramer’s V value: 0.12).
Fig. 1
Flow chart of database extraction.
LOS = length of stay, ICD-10 = 10th revision of the International Classification of Diagnoses.
aICD-10: B342, B972, U071, U072.
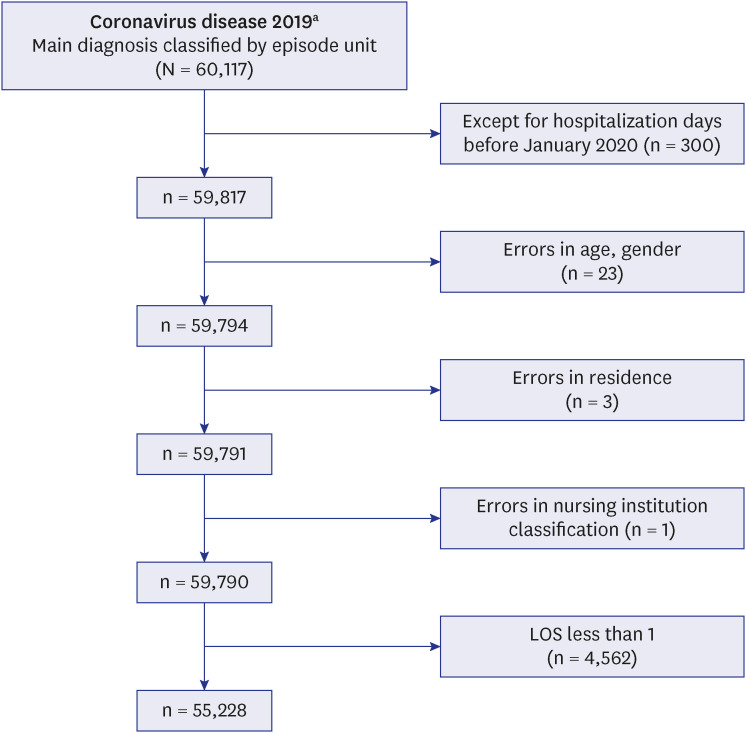
Table 1
Baseline patient characteristics
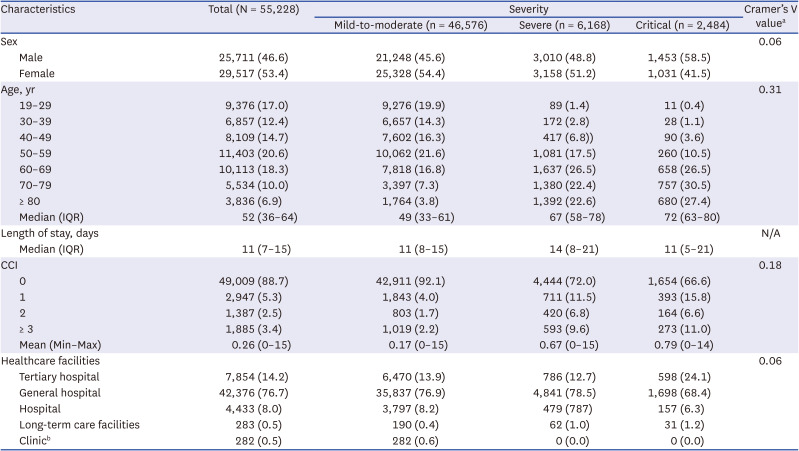
Values are presented as number of patients (%).
IQR = interquartile range, CCI = Charlson Comorbidity Index, Min = minimum, Max = maximum.
aIn the χ2 test, if the significance probability was < 0.0001, the correlation was evaluated by the Cramer’s V value (> 0.25: very strong; > 0.15: strong; > 0.10: moderate; > 0.05; weak; and > 0; no or very weak).
bPrimary health care facilities operating fewer than 30 beds.
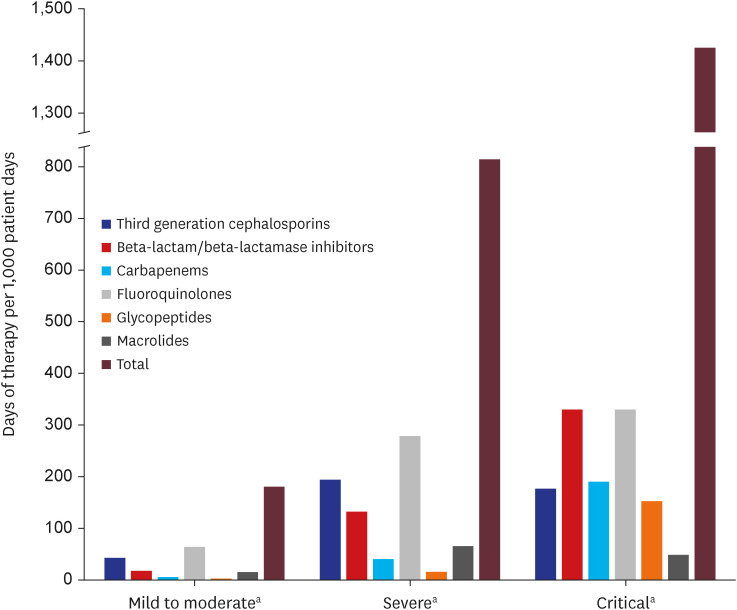
Antibiotics were prescribed to 27.3% (n = 15,081) of the total patients, and to 73.8%, 87.6%, and 17.9% of patients with severe, critical, and mild-to-moderate cases, respectively. Fluoroquinolones (n = 8,348) were the most commonly prescribed antibiotics, followed by third-generation cephalosporins (n = 5,729) and beta-lactam/beta-lactamase inhibitors (n = 3,822) (Supplementary Table 1). Total antibiotic use increased with severity, and fluoroquinolones were the most frequently prescribed antibiotics in all cases. In critical cases, the use of beta-lactam/beta-lactamase inhibitors exceeded that of third-generation cephalosporins, and the prescription of carbapenems and glycopeptides increased (Fig. 2). When at least one antibiotic was administered (15,081/55,228; 27.3%), the total number of antibiotic prescription days increased significantly according to age, severity, and CCI (β coefficients: 0.127, 0.135, and 0.087, respectively; adjusted R2 = 0.06) (Supplementary Table 2). There was no significant increasing or decreasing trend for either antibiotic or total antibiotic use based on hospitalization date during the study period (P ≥ 0.05) (Supplementary Fig. 1).
Fig. 2
Antibiotic prescription according to the severity of COVID-19.
COVID-19 = coronavirus disease 2019.
aCOVID-19 severity classification according to the National Institutes of Health guidelines: 1) Mild to moderate: Except for severe to critical cases; 2) Severe: Oxygen administration group; 3) Critical: high-flow nasal cannula, mechanical ventilator, extracorporeal membrane oxygenation application or sepsis, septic shock, respiratory failure, or acute respiratory distress syndrome during hospitalization among the oxygen administration groups.
Moreover, the antibiotic use rate was higher in the influenza group (107,642/188,483; 57.1%) than in the total COVID-19 patient group (66,225/312,082; 21.2%), and higher in severe-to-critical COVID-19 cases (29,072/43,675; 66.6%) than in influenza cases (Supplementary Fig. 2). In cases of patients with influenza, third-generation cephalosporins (52,764/188,483; 28.0%) were most frequently administered, followed by beta-lactam/beta-lactamase inhibitors (33,073/188,483; 17.5%) and fluoroquinolones (25,257/188,483; 13.4%).
DISCUSSION
In the present study, antibiotics were prescribed to not a few patients with COVID-19, and some of these cases were not severe. According to several studies, co- or secondary infections do not commonly occur in COVID-19; therefore, antibiotic prescription may be inappropriate in mild-to-moderate cases. In severe or critical COVID-19 cases, even if antibiotics are unavoidably administered because of concerns regarding co-infection or secondary infection, it is necessary to determine the appropriate agent and duration of antibiotic treatment based on the risk and possibility of bacterial infection. Recently, intestinal colonization by carbapenem-resistant Enterobacterales, invasive mechanical ventilation, administration of immunomodulators (i.e., tocilizumab and barictinib), and high levels of inflammatory markers, such as C-reactive protein on admission, have been identified as risk factors for bacterial co-infection.16
As the treatment guidelines for COVID-19 have been revised and several treatment options, including antiviral agents, immunomodulatory agents, and anticoagulants, have been well established,17181920 it was expected that the use of antibiotics would decrease over time. However, there were no significant changes in antibiotic use over the study period.
According to a previous systemic review,5 the proportion of patients in the antibiotic-treated group increased with age. As our study also revealed that age or underlying disease had a significant effect on antibiotic prescription rate, it is thought that concerns regarding bacterial infection may have contributed to antibiotic prescription requirement. This is consistent with other studies showing that old age is one of the risk factors for severe progression of COVID-1921 and one of the predictors of bacterial co-infection occurrence.22
Recent studies have shown that critical COVID-19 infection may be accompanied by bacterial infection,523 and is frequently complicated by secondary bacterial infection. In the case of critical COVID-19 infection, broad-spectrum antibiotics were often administered against multidrug-resistant organisms, including Pseudomonas aeruginosa or methicillin-resistant Staphylococcus aureus when the patient’s vital signs were unstable and mechanical ventilation was applied.24 However, routine administration of empirical antibiotics did not improve clinical outcomes in patients with moderate-to-severe illness requiring oxygen therapy.25 On the other hand, procalcitonin (PCT) level could be an indicator of disease severity in COVID-19 and can contribute to determining the severity of COVID-19,26 which may be one of the factors driving the use of antibiotics in severe COVID-19. Regardless of severity, an increase in the PCT level alone is insufficient to directly determine whether a patient has a co- or secondary bacterial infection with COVID-19,27 although a threshold of PCT < 0.3 ng/mL helps rule out bacterial co-infection.28 Therefore, it is important to determine the necessity of antibiotic therapy as well as select more appropriate antibiotics, based on the severity in each patient and various biomarkers after appropriate microbiological tests. In our study, the causative agent could not be identified, and the appropriateness of antibiotic prescriptions could not be evaluated owing to the limitations of the NHIS data.
Antibiotic use was higher in influenza patients than in the total patients with COVID-19, which might reflect the differences in indications for hospitalization between the two disease groups. In addition, the high possibility of complications of secondary bacterial pneumonia, including Streptococcus pneumoniae,2930313233 could influence antibiotic prescription in the former group, as previously experienced in pandemic and in patients with seasonal influenza.3435 As most of the patients hospitalized with influenza were presumed to have moderate or high severity, we further compared them with patients with severe-to-critical COVID-19, which revealed that the antibiotic administration rate was somewhat higher in the latter group.
Since this study used claims data, it had a few limitations. First, it was impossible to evaluate individual cases to determine whether antibiotic administration was appropriate because the medical records were not individually reviewed. Second, data analysis was delayed owing to the nature of claims data, and there were difficulties in the real-time evaluation of long-term changes after 2021. Nevertheless, the number of participants in this study was 55,228, accounting for 90% of all 60,726 patients with COVID-19 in Korea identified from the Korea Disease Control and Prevention Agency from December 1, 2019 to December 31, 2020,36 which means that it could be representative of all COVID-19 patients in Korea.
In conclusion, antibiotic stewardship is a necessary practice for reducing antibiotic overuse, considering the spread of multidrug-resistant bacteria worldwide during the COVID-19 pandemic.373839 Moreover, as most COVID-19 cases are mild-to-moderate and bacterial co-infection or secondary infection is not common, it is necessary to determine the appropriate agent and duration of antibiotic treatment.
 XML Download
XML Download