

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Diabetic foot ulcer (DFU), a complication of diabetes, is economically burdensome and associated with a premature mortality rate of 30%, comparable to the 5-year mortality of all reported cancers.1 The major etiologies of DFU include infection, ischemia, and neuropathy.2 The management of these factors is important for improving DFU outcomes.
In patients with diabetic kidney disease (DKD), the prevalence of DFU is more than twice as high, and the amputation rate is 6.5–10 times higher, than that in the general diabetic population.3 This may be due to another etiology of DFU: vascular calcification.4 Among patients with peripheral arterial occlusive disease, the calcification of the lower extremity arteries increases DFU risk,4 amputation, and all-cause mortality.5 In patients with critical limb ischemia, the ankle–brachial index (ABI) cannot be measured because of the stenosis or calcification of peripheral arteries.6 In such cases, the assessment of medial arterial calcification (MAC) severity using a scoring system might be useful.7 Although MAC is common in patients with diabetes mellitus or chronic kidney disease (CKD), the association between the MAC score and amputation risk of DFU has been less explored.
Thus, we aimed to assess DFU characteristics, including MAC, and analyze its effect on the risk of major amputation in patients with DKD.
METHODS
This cross-sectional study retrospectively enrolled 261 DFU patients with DKD stages 3b–5 (estimated glomerular filtration rate [eGFR] < 45 mL/min/1.73 m2 calculated using the Modification of Diet in Renal Disease formula) treated at Yeungnam University Hospital from 2002 to 2020. CKD stages 3b–5 are associated with increased all-cause and cardiovascular mortality8 and designated as renal outcomes in various clinical trials.9 Patients who had incomplete X-ray images or had undergone amputation before enrollment were excluded (n = 51). Finally, 210 patients were included in the analysis.
Data on patients’ age, sex, duration of diabetes, body mass index, smoking, drinking, and dialysis status, current antiplatelet use, erythrocyte sedimentation rate, hemoglobin A1c and total cholesterol levels, GFR, and presence of hypertension, stroke, and coronary artery disease were collected.
The DFU location was categorized as forefoot, mid-, or hindfoot. The extent of DFU penetration (grades 0–3) and the presence of ischemia or infection (stages A–D) were evaluated using the University of Texas Wound Classification System.10 Ischemia was defined as wounds with claudication, rest pain, absent pulses, dependent rubor, or pallor on elevation. Infection was defined as wounds with purulence and/or local signs (e.g., warmth, erythema, edema, pain, and loss of function). Diabetic neuropathy was diagnosed using a 10-g monofilament11 and clinical scores were assessed using a questionnaire (Michigan Neuropathy Screening Instrument).12 The presence and extent of vascular calcifications were assessed through three-view radiography (anteroposterior, lateral, 45° oblique projection) using the MAC scoring system7 (Fig. 1). The sum of MAC ranged from 0–5 and was divided into three categories: no MAC (0 or 1 positive site), moderate (2 or 3 positive sites), and severe (4 or 5 positive sites).
Fig. 1
Assessment of vascular calcification using MAC. MAC was assessed in five arterial sites. A positive score of 1 was given for ≥ 2 cm calcification in the 1) dorsalis pedis, 2) lateral plantar, and 3) first metatarsal artery, or ≥ 1 cm calcification in the 4) first toe and 5) other toe arteries. (A) The anteroposterior (left) and lateral (right) views of “no MAC.” A total of one positive score was assigned to the lateral plantar artery (5.9 cm). (B) The anteroposterior (left) and lateral (right) views of “moderate MAC.” Two positive scores were assigned to the dorsalis pedis artery (5.4 cm) and first metatarsal artery (2.8 cm). (C) The anteroposterior (left) and lateral (right) views of “severe MAC.” Five positive scores were assigned for the dorsalis pedis artery (8.0 cm), lateral plantar artery (5.6 cm), first metatarsal artery (2.1 cm), first toe artery (3.9 cm), and third toe artery (1.7 cm).
MAC = medial arterial calcification.

The extent of amputation was categorized as minor and major according to the International Working Group on the Diabetic Foot guidelines.13 Minor amputation was defined as resection through, or distal to the ankle including debridement.14 Major amputation was defined as resection proximal to the ankle.
Continuous and categorical variables were compared using Student’s t-test and χ2 test, respectively. Multivariate logistic regression was performed to determine the risk factors for major amputation. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. Statistical significance was set at P value < 0.05. All statistical analyses were performed using IBM SPSS Statistics version 25.0 (IBM Corp., Armonk, NY, USA).
RESULTS
The participants had an average age of 62.9 years, male-to-female ratio of 1.56:1, and an average duration of diabetes of 17.1 years. Sixty-one patients (33.7%) were undergoing dialysis. In total, 184 (87.6%) and 26 patients (12.4%) underwent minor (debridement, n = 108; toe or transmetatarsal amputation, n = 76), and major amputations (transtibial amputation, n = 23; transfemoral amputation, n = 3), respectively.
The baseline patient characteristics are presented in Supplementary Table 1. The clinical and biochemical variables were not significantly different between the minor and major amputation groups, except for GFR: 20.9 ± 12.9 mL/min/1.73 m2 and 15.7 ± 12.0 mL/min/1.73 m2 in the minor and major amputation groups, respectively (P = 0.049). Patients with an eGFR < 20 mL/min/1.73 m2 accounted for 53.8% patients in the minor amputation group and 73.1% patients in the major amputation group (P = 0.100). The number of patients using antiplatelets was higher in the minor amputation group without statistical significance (54.3% vs. 34.6%, P = 0.094). Regarding the DFU characteristics (location, Texas grade and stage, neuropathy, and MAC), the major amputation group had a significantly higher proportion of DFU located in the mid-or hindfoot than in the forefoot (P = 0.015) and DFU of higher Texas grades (P = 0.003) than the minor amputation group. The group differences in Texas stage (P-for-trend = 0.281), neuropathy (P = 1.000), or MAC (P-for-trend = 0.156) were non-significant.
The logistic regression analysis of the effect of the characteristics of diabetic foot on the risk of major amputation is presented in Table 1. Antiplatelet use, ulcer location, Texas grade, and MAC score were considered as covariates for the adjusted model. After adjustments, not only DFU located at the mid- or hindfoot (ref, forefoot; OR, 3.27; 95% CI, 1.26–8.5; P = 0.015) and Texas grades 2 or 3 (ref, Texas grade 0; OR, 5.78; 95% CI, 1.81–18.44; P = 0.003), but also severe MAC (ref, no MAC; OR, 4.46; 95% CI, 1.43–13.88; P = 0.010) were revealed as risk factors for major amputation. Concurrent use of antiplatelets was a possible protective factor for major amputation with borderline significance (OR, 0.37; 95% CI, 0.13–1.02; P = 0.055).
Table 1
Risk factor assessment for major amputations of diabetic foot ulcers
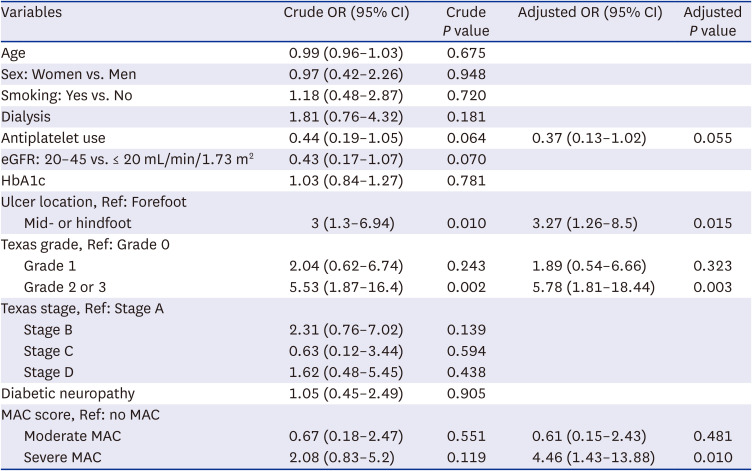
Texas grade 0, pre- or post-ulcerative site that has healed; grade 1, superficial wound not involving tendon, capsule, or bone; grade 2 or 3; wound-penetrating tendon or capsule or wound-penetrating bone or joint.
Texas stage A, clean wounds; stage B, non-ischemic infected wounds; stage C, ischemic non-infected wounds; stage D, ischemic infected wounds.
No MAC, 0 or 1 positive site; moderate MAC, 2 or 3 positive sites; severe MAC, 4 or 5 positive sites.
OR = odds ratio, CI = confidence interval, MAC = medial arterial calcification.
DISCUSSION
We assessed the DFU characteristics among patients with CKD stages 3b–5 and investigated the risk of major amputation. We found that ulcer location, extent of ulcer penetration, and severe MAC increased the risk of major amputation by 3–6 times.
DFU should be considered a multi-organ disease. A combination of infection, extension of ulcer penetration, and ischemia can prospectively affect 1-year outcomes of major amputation, mortality, and wound healing.15 In addition to the well-known risk factors for DFU amputation, we quantified the degree of vascular calcification by the MAC scoring system. As ABI was unavailable in 61% of the patients (data not shown), MAC was a useful substitute for vascular calcification.16 In diabetic patients with MAC, the lower extremity amputation rate was reported to be 3–5.5 times higher than that in patients without MAC.1718 In this study, patients with DKD stage 3b–5 with severe MAC had 4.5 times higher risk for major amputation than in patients without MAC. The concept of MAC, calcification of blood vessels due to the denervation of the intimal media of the small muscular arteries of the foot, was proposed in the 1980s.19 MAC is a multifactorial reaction caused by arterial pressure, immune response, oxidative stress, hyperglycemia, and mineral derangements of calcium and phosphorus metabolism.20 Arterial stiffness and vascular calcification appear in the early stages of DKD21 and may be useful predictors of diabetes-related complications. As it can be easily measured through foot radiography or ultrasonography,22 it can be used as a major DFU characteristic if a large amount of evidence is collected. In addition, the use of antiplatelets may reduce the risk of amputation; it should be confirmed by further studies whether antiplatelets can prevent peripheral arterial disease.2324
This study has some limitations. First, the sample size was relatively small. Second, the degree of microalbuminuria was not measured during DKD staging. Third, the DFU characteristics and outcomes were evaluated using electronic medical records from a single center; therefore, generalization of the results may be difficult. Fourth, the patients were enrolled for > 18 years, during which treatment strategy may have been changed. However, this study is the first to explore the possibility of using the MAC score as a predictor of DFU amputation in patients with DKD. The effect of MAC on DFU should not be underestimated, and further prospective larger studies with DFU might show noteworthy results.
In conclusion, severe MAC is a significant risk factor for major amputation in DFU patients with DKD.
 XML Download
XML Download