

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Total joint arthroplasty, including total hip arthroplasty (THA) and total knee arthroplasty (TKA), is a popular surgical option for elderly patients with advanced joint disease.1234567891011 Unlike TKA, THA is not an operation that is commonly known to control the lower limb alignment. However, we can reasonably expect that lower limb alignment is influenced by changes in the hip joint profile after THA, eventually affecting the condition of knee joints.
Some studies have evaluated the effects of THA on knee joint.1213141516 Ollivier et al.15 and van Drongelen et al.16 reported that the hip–knee–ankle angle (HKA) changes in the varus direction after THA. In particular, van Drongelen et al.16 showed that this change could cause progression of medial knee OA. In contrast, Umeda et al.12 reported that the ipsilateral knee joint changed in the valgus direction after THA and this change was associated with a decreased femoral offset (FO). Furthermore, they reported that the OA progression was more prominent in the contralateral knee than in the knee ipsilateral to the THA. Similarly, Shakoor et al.14 reported that the progression of knee osteoarthritis (OA) after THA was higher in the contralateral knee joint than in the ipsilateral knee joint. Therefore, it remains unclear whether THA can affect coronal alignment in the ipsilateral limb and whether this alignment change can influence the condition of the ipsilateral knee joint, notably OA progression.
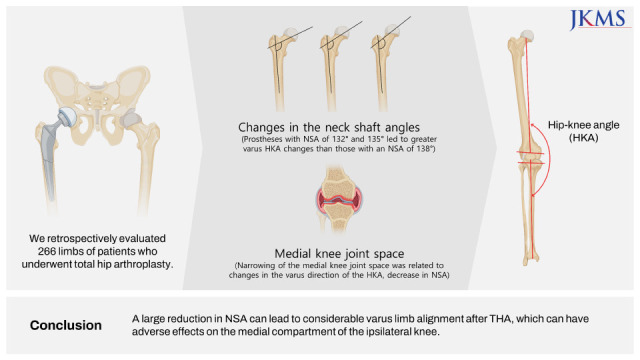
This study aimed to 1) assess the effect of THA on coronal limb alignment, namely, the HKA, 2) identify factors related to changes in the HKA, and 3) determine whether alignment changes influence the knee joint space width. We hypothesized that the ipsilateral coronal limb alignment, i.e., the HKA, would change after THA, and this change in the HKA would be affected by the change in the hip joint profile. In addition, such alignment changes would adversely affect the corresponding ipsilateral knee joint space, that is, the medial knee joint space in the case of more varus change, at the follow-up of more than 5 years.
METHODS
Subjects
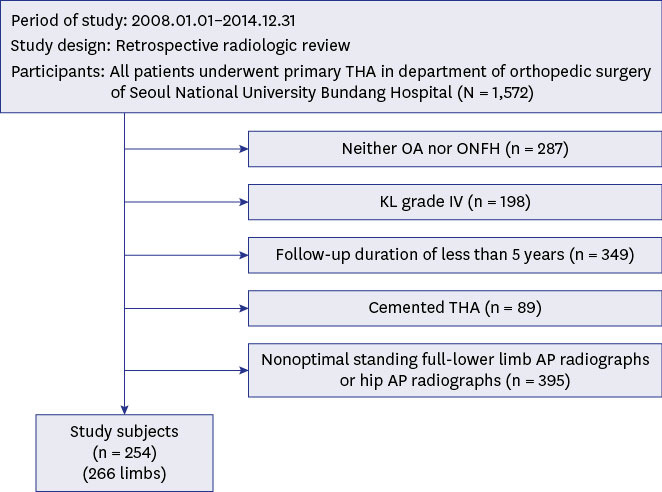
We retrospectively reviewed the records of 1,572 patients who underwent primary THA in a single institution between January 2008 and December 2014. The inclusion criteria were as follows: 1) osteonecrosis of the femoral head (ONFH) or OA, 2) ipsilateral knee of Kellgren-Lawrence (KL) grade17 I, II or III when undergoing THA, 3) follow-up period of at least 5 years, 4) underwent cementless THA, and 5) underwent optimal full lower limb anteroposterior (AP) radiography and a standing hip AP radiograph before and at least 5 years after THA. After implementing the inclusion criteria, 254 patients (120 men and 134 women) with 266 limbs (OA = 133, ONFH = 133) were enrolled (Fig. 1). Twelve patients with bilateral THA underwent separate procedures with separate radiographs and a follow-up of at least 5 years for each limb. The average age at the time of THA was 52 ± 14 years (range, 17–88 years), and the mean follow-up period was 6.9 years (range, 5–12 years, standard deviation [SD] = 1.9). The mean body mass index (BMI) was 24.4 ± 3.9 kg/m2 (range, 10.7–37.7). Post hoc power analysis was performed using the HKA as the primary outcome (preoperative HKA, mean = 1.4, SD = 3.9; postoperative HKA, mean = 2.7, SD = 4.3), and the statistical power was over 80% (G*Power 3.1.0).
Operative technique
All THAs were performed by three surgeons (YKL, YCH, and KHK) using the posterolateral approach.18 Acetabular and femoral components were inserted in a press-fit manner. Three combinations of cementless implants (Bencox M Stem, Mirabo cup [Corentec, Laguna Hills, CA, USA]: 94 cases; Corail Stem, plasma cup [Depuy, Raynham, MA, USA]: 97 cases; and Taperloc Stem, ABT cup [Zimmer Biomet, Warsaw, IN, USA]: 75 cases) were used. Delta ceramic bearings were used in all hips.
We used the combined anteversion technique to determine the location and orientation of the inserted implants.19 First, the femoral side was prepared. The cancellous bone in the femoral canal was removed with a box chisel, and a single starter reamer was inserted into the distal femoral canal to a level appropriate for the templated stem size. The femoral canal was prepared using stem-specific broaches. We used the smallest broach first and then progressively increased the broach size until the broach tightly engaged the medial and lateral cortex of the proximal femur. Next, we measured stem version of the final broach. The target anteversion of the metal shell was calculated using the following formula20: Cup Anteversion = 37.3° − (0.7 × Stem Anteversion). The target abduction of the metal shell was 43°.21 The acetabular cup was positioned at the target site using the method described by Ha et al.21 Follow-up visits were scheduled for 6 weeks, 6 months, 1 year, and every year thereafter. At each annual visit, standing full lower limb AP radiographs and standing hip AP radiographs were obtained.
Radiographic examination
Radiographic evaluations were performed using standing full lower limb AP radiographs and standing hip AP radiographs, which were obtained using a UT 2000 X-ray machine (Philips Research, Eindhoven, The Netherlands) set to 90 kV and 50 mAs. Standing full lower limb AP radiographs were acquired by vertically entering the horizontal center beam to the patellar height and vertical beam to the midline. The X-ray beam was centered at the midpoint between the upper part of the symphysis and the line connecting the anterior superior iliac spines on standing hip AP radiographs. Both standing full-lower limb AP and Standing hip AP radiographs were acquired with the patella facing forward. All radiographic images were digitally acquired using a Picture Archiving and Communication System (PACS). Assessments were performed on a 24-inch (61-cm) LCD monitor (T245; Samsung, Seoul, Korea) in portrait mode using the PACS software.
Radiographic measurement
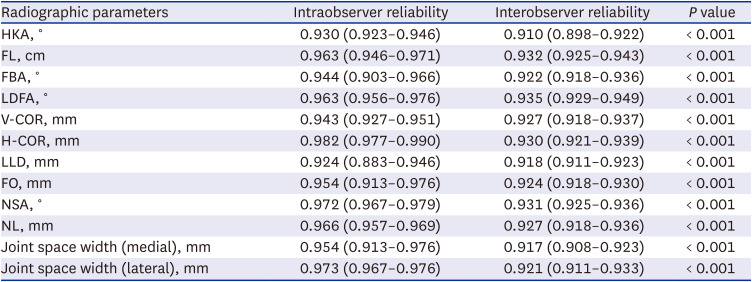
Preoperative radiographs were used as baseline for comparison. In the preoperative and final follow-up (minimum 5 years postoperatively) radiographs, several radiographic parameters were measured: HKA, femur length (FL), femoral bowing angle (FBA),2223 lateral distal femoral angle (LDFA), medial and lateral joint space width on standing full lower limb AP radiographs, hip center position (vertical center of rotation [V-COR], horizontal center of rotation [H-COR]),24 limb length discrepancy (LLD), FO, neck shaft angle (NSA), and neck length (NL) on standing AP hip radiographs (Fig. 2). HKA was defined as the angle between the mechanical axes of the tibia and femur. A positive value was assigned to the knees in varus alignment. The FL was defined as the distance from the uppermost margin of the head to the lowermost margin of the medial condyle. FBA was defined as the angle between the line connecting the points bisecting the femur at 0 and 5 cm below the lowest portion of the lesser trochanter and the line connecting the points bisecting the femur at 5 cm and 10 cm above the lowest portion of the lateral femoral condyle. Positive numbers were used if the femoral shaft displayed lateral bowing. LDFA was defined as the lateral angle between the femoral mechanical axis and the tangent of the distal femur. The medial and lateral joint space widths were measured as the minimum distance in each part of the knee joint. We measured two hip center positions: the V-COR and H-COR. The V-COR was defined as the vertical distance from the center of the femoral head to the inter-teardrop line. The H-COR was defined as the horizontal distance from the V-COR line to the radiographic teardrop. LLD was defined as the difference in the perpendicular distance between the line passing through the lower edge of the teardrop point to the corresponding tip of the lesser trochanter. FO was defined as the vertical distance from the center of rotation of the femoral head to a line bisecting the long axis of the femur. The NSA was defined as the angle between the longitudinal axis of the native or prosthetic neck and the anatomical axis of the femoral shaft. Postoperative NSA was also the measured NSA in the radiographs, not the implant angle. NL was defined as the distance from the cross point of the shaft axis and the central axis of the femoral neck to the head center. All radiographic parameters were measured by manual methods, and the minimum detectable changes by the software were 0.1° in angle and 0.1 mm in length. The intra- and inter-observer reliabilities of all radiographic measurements were evaluated using intraclass correlation coefficients (ICCs). Two orthopedic surgeons (YSC and TWK) independently measured the radiographic parameters. Radiologic parameters were re-measured twice at 3-week intervals by each examiner. The ICCs of the intra-and inter-observer reliabilities were > 0.9 (range: 0.910–0.982), indicating that the measurements were highly reliable (Table 1).
Fig. 2
Radiographic measurements. (A) HKA, FL. (B) LDFA. (C) FBA. (D) LLD. (E) Medial and lateral joint space widths. (F) V-COR: black line ‘a’; H-COR: black line ‘b’; FO, NSA: angle formed by white line ‘c’ and white line ‘d’; NL: white line ‘c’.
HKA = hip–knee–ankle angle, FL = femur length, LDFA = lateral distal femoral angle, FBA = femoral bowing angle, LLD = limb-length discrepancy, V-COR = vertical center of rotation, H-COR = horizontal center of rotation, FO = femoral offset, NSA = neck shaft angle, NL = neck length.
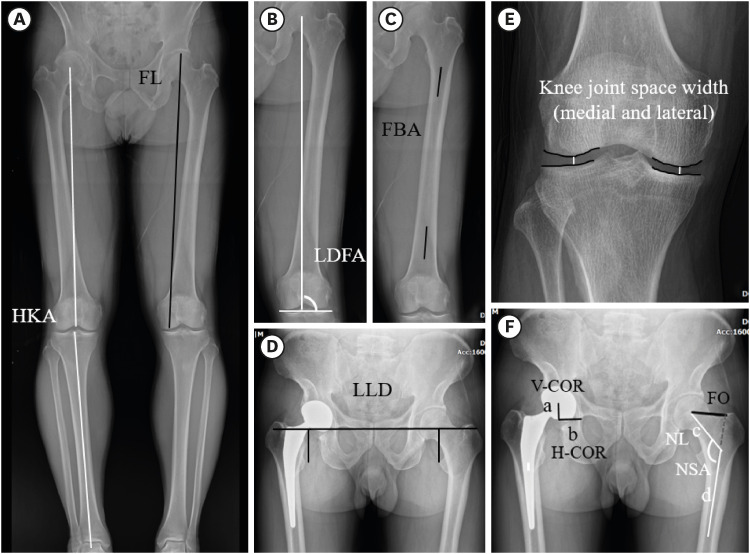
Table 1
Intraobserver & interobserver reliability of radiographic measurements
Clinical evaluation
We evaluated whether patients underwent ipsilateral TKA after THA by reviewing medical records and radiographs.
Statistical analysis
A paired t-test was used to confirm the effect of THA on HKA change (Δ). Changes in other radiological parameters were also analyzed (Δ: Postoperative Parameters − Preoperative Parameters).
An analysis of the relationship between demographic variables (gender, age, BMI) and ΔHKA was performed. An analysis of the relationship between gender and ΔHKA was were analyzed using the Student’s t-test, and an analysis of the relationship between age, BMI and ΔHKA was analyzed using the Pearson’s correlation analysis. Multiple regression analysis was used to determine the Δradiographic parameters that were significantly related to the ΔHKA. Subgroup analysis was performed to evaluate the effects of ΔNSA on ΔHKA. The subjects were divided according to ΔNSA: 1) ΔNSA < −5°, 2) −5° < ΔNSA < 5°, and 3) ΔNSA > 5°. No significant differences were noted in the preoperative HKA and KL grades between the groups (Table 2). Paired t-test and simple regression analysis were performed to confirm ΔHKA and the relationship between ΔNSA and ΔHKA in each group, respectively. Next, subjects were divided according to the three stems with different NSAs: 1) Bencox M Stem (NSA: 132°), 2) Corail Stem (NSA: 135°), and 3) Taperloc Stem (NSA: 138°), and the ΔHKA of these subgroups was compared according to NL: short, medium, and long necks. The differences in these subgroups were analyzed using a one-way analysis of variance test and post hoc analysis.
Table 2
Preoperative HKA and KL grade according to ΔNSA

HKA are presented as means ± standard deviation. KL are presented as number with the percent in parentheses.
NSA = neck shaft angle, HKA = hip–knee–ankle angle, KL = Kellgren-Lawrence, ΔNSA = Postoperative NSA − Preoperative NSA.
aDerived using the one-way analysis of variance test; bDerived using the linear by linear association.
Finally, to determine whether alignment changes influence the knee joint’s condition, a multiple regression analysis was performed to identify factors related to the Δknee joint space width, and subgroup analysis was also performed. The subjects were divided according to the Δknee joint space: 1) Δknee joint space > −1 mm (maintained joint space group) and 2) Δknee joint space < −1 mm (narrowed joint space group).25 The demographic variables of these groups were compared (Table 3). The Δradiologic parameters and proportion of ipsilateral TKA were compared according to these subgroups. ΔRadiologic parameters were compared using Student’s t-test, and the proportion of TKA were compared using the χ2 test. Statistical analysis was performed using SPSS (version 26.0; IBM, Armonk, NY, USA), and significance was set at P < 0.05.
Table 3
Patient demographics between maintained joint space group vs. narrowed joint space group

RESULTS
The HKA changed 1.3° in the varus direction (P < 0.001) (Table 4).
Table 4
Changes in radiographic parameters
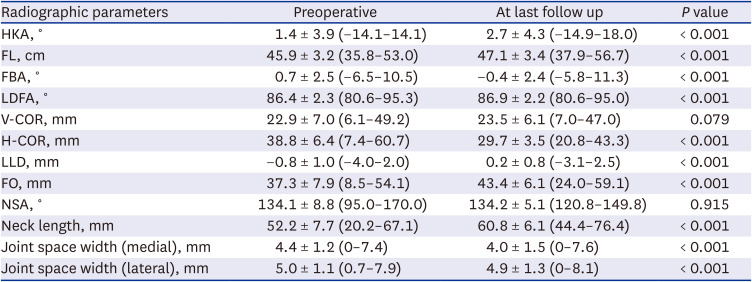
Data are presented as means ± standard deviations (minimum–maximum).
HKA = hip–knee–ankle angle, FL = femur length, FBA = femoral bowing angle, LDFA = lateral distal femoral angle, V-COR = vertical center of rotation, H-COR = horizontal center of rotation, LLD = limb-length discrepancy, FO = femoral offset, NSA = neck shaft angle.
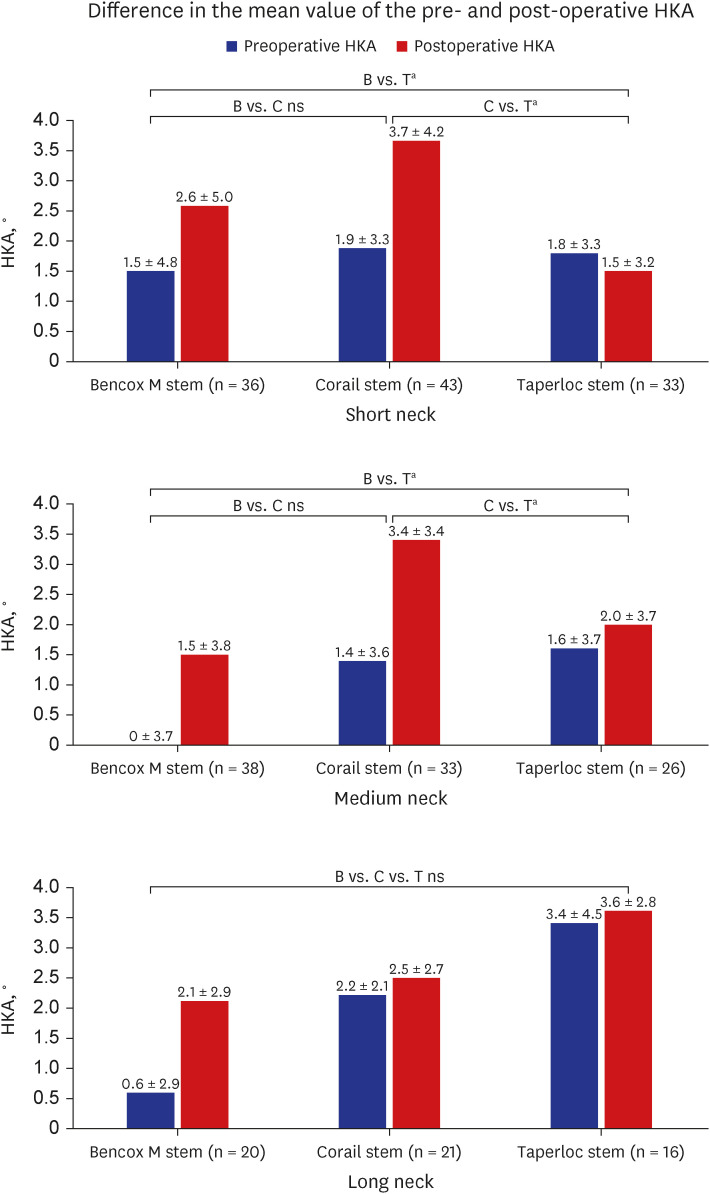
There was no significant relationship between demographic variables and ΔHKA (Table 5). ΔHKA was related to ΔNSA (coefficient: −0.45, P < 0.001), ΔLDFA (coefficient: 0.27, P < 0.001), and ΔFBA (coefficient: 0.19, P < 0.001). The lower limb changed in the varus direction when the NSA decreased or LDFA or FBA increased compared with the preoperative value after THA. In the ΔNSA < −5° group, the preoperative mean HKA was 1.4° varus (SD = 4.5°), which changed to 4.6° varus (SD = 4.6°) after THA (P < 0.001) (Fig. 3). A significant correlation was noted between ΔNSA and ΔHKA in this group (coefficient = −0.68, P < 0.001) but not in the other two groups. Thus, the smaller the NSA after THA, the greater the change in the varus direction in this group. In the short neck group, both the Bencox M Stem (132°) and Corail Stem (135°) changed the HKA in the varus direction more than the Taperlock Stem (138°) (P = 0.009 and P < 0.001, respectively). However, no significant difference was noted in ΔHKA between Bencox M Stem (132°) and Corail Stem (135°) (P = 0.292). The same pattern was observed in the medium-neck group; however, in the long neck group, no significant difference was noted in ΔHKA (P = 0.298) between the three stems (Fig. 4).
Table 5
Relationship between demographic variables and ΔHKA after total hip arthroplasty

| Variables | ΔHKA, ° | ΔHKA (r) | P value | |
|---|---|---|---|---|
| Gender | 0.914 | |||
| Women (n = 144) | 1.2 ± 2.8 | |||
| Men (n = 122) | 1.3 ± 2.7 | |||
| Age | −0.081 | 0.186 | ||
| BMI | −0.096 | 0.118 | ||
Fig. 3
Difference in the mean value of the pre- and post-operative HKA in the three subgroups based on the change in NSA induced by THA. HKA is presented as means ± standard deviations.
HKA = hip–knee–ankle, NSA = neck shaft angle, THA = total hip arthroplasty, ΔNSA = Postoperative NSA − Preoperative NSA, ns = not significant.
***Statistically significant (P < 0.001).
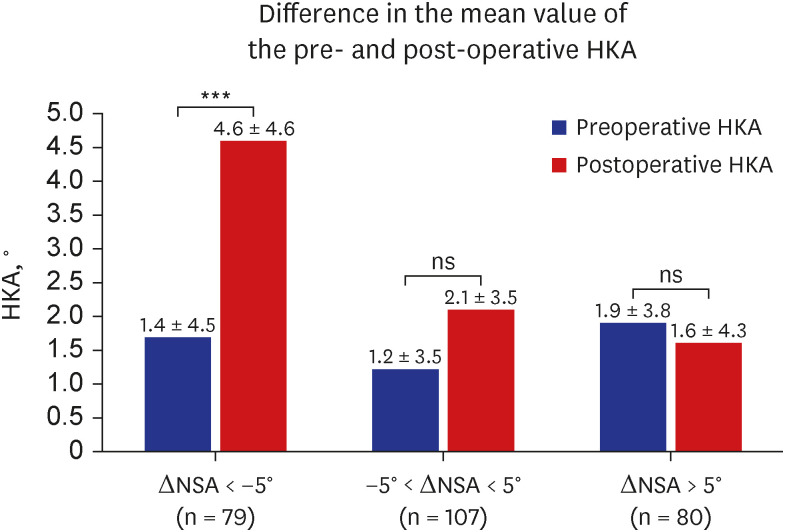
Fig. 4
Difference in the mean value of the pre- and post-operative HKA in the three prosthesis groups based on the neck length. HKA is presented as means ± standard deviations. Short neck: ANOVA test (P = 0.002), post hoc analysis (B vs. T, P = 0.009; C vs T, P < 0.001; B vs C, P = 0.292). Medium neck: ANOVA test (P = 0.004), post hoc analysis (B vs. T, P = 0.016; C vs. T, P = 0.006; B vs. C, P = 0.882). Long neck: ANOVA test (P = 0.298).
HKA = hip–knee–ankle angle, ns = not significant, B = Bencox M Stem, C = Corail Stem, T = Taperloc Stem, ANOVA = analysis of variance.
aStatistically significant.
As the change in the varus direction of the lower limb increased after THA, the medial knee joint space width narrowed. ΔMedial knee joint space width was related to ΔHKA (coefficient: −0.418, P < 0.001). The narrowed joint space group showed a greater varus ΔHKA (1.0° vs. 2.1°), a greater chance of undergoing TKA (3/210 [0.014%] vs. 6/56 [10.7%]; odds ratio = 8.3, P < 0.001) compared with the maintained joint space group. Additionally, ΔNSA of the maintained joint space group and narrowed joint space group was 0.8° and −2.7°, respectively, and ΔFO was 5.5 and 8.5 mm, respectively (Table 6).
Table 6
Comparison of Δradiographic parameters of the maintained joint space group and narrowed joint space group
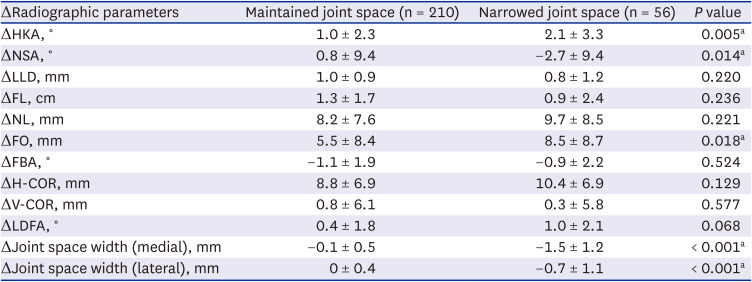
Data are presented as means ± standard deviations. ΔRadiographic parameter = Postoperative Radiographic Parameter − Preoperative Radiographic Parameter.
HKA = hip–knee–ankle angle, NSA = neck shaft angle, LLD = limb-length discrepancy, FL = femur length, NL = neck length, FO = femoral offset, FBA = femoral bowing angle, H-COR = horizontal center of rotation, V-COR = vertical center of rotation, LDFA = lateral distal femoral angle.
aStatistically significant.
DISCUSSION
This study showed that the HKA of the ipsilateral limb changed in the varus direction at least 5 years after THA. In particular, a significant relationship was noted between the large decrease in the NSA and the change in the varus direction. Narrowing of the medial knee joint space was related to an increase in the varus direction. Thus, we assumed that significant varus change in coronal limb alignment would mainly occur immediately after THA, if there is a large reduction in NSA. Our results suggest that significant varus change could lead to progression of medial knee joint space narrowing (Fig. 5).
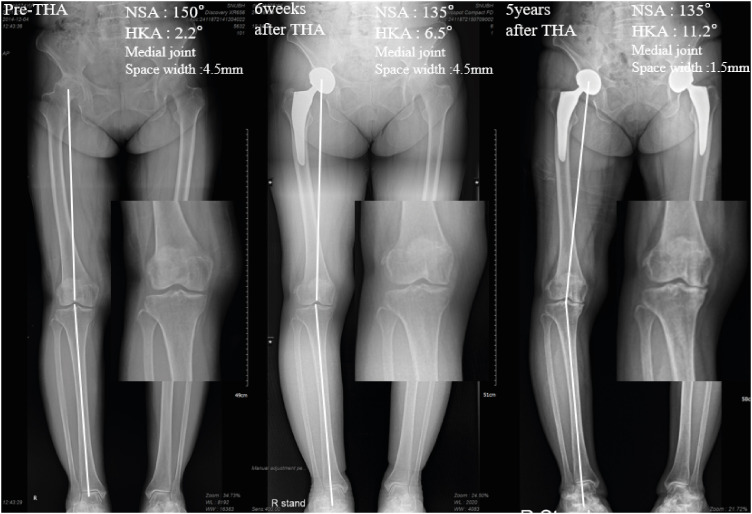
Fig. 5
Exemplar change in HKA and medial knee joint space width after THA.
THA = total hip arthroplasty, HKA = hip–knee–ankle, NSA = neck shaft angle.
Changes in HKA and FO are known to be related to varus changes in lower limb alignment after THA. Ollivier et al.15 and van Drongelen et al.16 reported that the ipsilateral HKA changed in the varus direction by approximately 1.5° and 1° after THA, respectively, and that FO increased after THA, which could change the lower limbs to varus alignment. In the present study, the mean HKA and FO increased by 1.3° and 6.1 mm, respectively after THA. We also found that the mean H-COR decreased by 9.1 mm after THA, indicating medialization of the hip center. This is in line with a recent study by Akasaki et al.26 in which the authors suggest that varus change (0.8°) after THA is related to medial shifting of the hip center. Furthermore, we found that the change in HKA was related to various radiological parameters, such as ΔNSA, ΔLDFA, and ΔFBA. Although whether each parameter has a causative relationship with varus change is unclear, the increase in HKA seems to be multifactorial rather than related to a single strong radiologic parameter. One possible logical explanation is that simultaneous increase in FO and medialization of the hip center could result in an increase in HKA by medial shifting of the hip center without altering the knee and ankle centers. In this setting, the HKA could be additionally increased if the femur changed to varus alignment (smaller NSA, larger LDFA, and FBA).
Interestingly, the HKA changed much more in the varus direction in certain groups where the NSA became significantly smaller after THA (Fig. 3). Umeda et al.12 reported that the ipsilateral knee joint changed in the valgus instead of in the varus direction after THA. This may be because prostheses with a high NSA were used, and the FO decreased in their study. The relationship between ΔNSA and ΔHKA may be explained by the FO, which is usually restored or increased to improve the efficiency of the gluteus medius and reduce polyethylene wear during THA.272829 According to the ΔNSA subgroup analysis, ΔFO in ΔNSA < −5°, −5° < ΔNSA < 5°, and ΔNSA > 5° were 12.8, 5.7, and 0.1 mm, respectively. If the NSA increases after THA, the potential to restore FO is limited. Therefore, in the ΔNSA > 5° group, the change in the varus direction was not as apparent as in the other groups. Consequently, to prevent an increase in HKA, an excessive decrease in NSA throughout THA should be avoided. While other radiological parameters are difficult to manipulate during THA, NSA could be adjusted using different femoral stems, NLs, and lateralized stems. Among the three femoral stems used in this study, the Taperloc Stem demonstrated the least change in HKA compared with Bencox M Stem and Corail Stem (Fig. 4).
In this study, we found that THA could be associated with the medial knee joint space narrowing. Shakoor et al.14 reported that the peak load and adduction moment of the medial compartment of the knee were already high in end-stage hip OA; thus, the adapted knee state did not recover even after THA. However, our study was not limited to end-stage hip OA but was conducted on hip OA and ONFH at various stages. Ollivier et al.15 showed that HKA changes in the varus direction after THA, as in our study; however, this did not affect the knee joint. Concurrently, van Drongelen et al.16 reported that HKA changes in the varus direction after THA and that this increases the knee adduction moment; thus, medial knee OA can progress. Our study also confirmed medial knee joint space narrowing after THA, similar to van Drongelen et al.’s study,16 and further confirmed that medial knee joint space narrowing was associated with ΔHKA, ΔNSA, and ΔFO. In this study, the narrowed joint space group showed more varus changes and a higher chance of experiencing ipsilateral TKA. This may be associated with the greater decrease in NSA and increase in FO compared with the maintained joint space group. However, it cannot be said that our study elucidated these relationship, and it is clinically meaningful that the possibility that such a relationship may exist has been shown. These findings should preclude surgeons from making the decrease in NSA too large in patients with preexisting varus limb alignment or medial knee OA.
This study has limitations. First, the age range of the study subjects is wide. As age would potentially affect changes of limb alignment and knee joint conditions, such chronological effect on physiological changes of the limb and knee joint during > 5 years follow-up may be different between young and old subjects. However, age would not be related to degrees of alignment and knee joint condition changes in this study cohort (Tables 3 and 5), probably because of relatively small proportion of very young and/or very old subjects. Second, we were unable to assess the differences between manufacturers, surgeons, or prosthesis sizes. Lateralized femoral stems were not used in this study. Lateralized stems are currently widely used especially in THA of dysplastic hips where medialization of the hip center is frequently required. Further studies assessing the standard and lateralized stems by the same manufacturers are warranted. Third, exclusion criteria eliminate 83% of the target THA population. However, as most of them were excluded due to unavailable optimal radiographs rather than intrinsic characteristics of the subjects, it is not expected that this will affect the generalizability of the results of this study.
In conclusion, coronal limb alignment tended to change in the varus direction after THA, but the average HKA change was small (1.3°). Nevertheless, a large reduction in NSA can be associated with considerable varus limb alignment change after THA, which can have adverse effects on the medial compartment of the ipsilateral knee. This study does not suggest the current best practice in the field of THA should be changed. Nevertheless, information in this study would be useful for estimation of limb alignment change after THA by a surgeon and counseling and further planning for a subset of patient who are expected to experience aggravation of varus malalignment and deterioration of established medial knee OA.
 XML Download
XML Download