

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Self-harming behavior includes a wide range of behaviors that directly and deliberately harm one’s body. Among these behaviors, nonsuicidal self-injury (NSSI) is the intentional damaging of body tissue without the intent to die.1 The prevalence of NSSI is nearly 6% in the general population.2 Even higher rates were found among college students and adolescents, with studies reporting 15% to over 35% NSSI prevalence in samples.34 Self-harm is a severe problem that not only causes physical damage but is also strongly associated with various mental health challenges such as depression, anxiety, eating disorders, borderline personality disorder (BPD), and suicidality.56 Especially the high risk of suicide among individuals with NSSI stresses the importance of early screening for NSSI. Although they begin to engage in self-harming behaviors without serious suicidal intent, individuals who repetitively harm themselves experience desensitization to physical pain, increasing the risk of suicide.78 As large-scale prospective studies have demonstrated, individuals with NSSI show a 2 to 3 times higher risk of suicide ideation and suicide attempts compared to the general population.9 Furthermore, the rate of completed suicide was 37.2 times higher in individuals with NSSI than in the matched general population.10 There are also significant studies on the relationship between suicidality and NSSI in Korea. Research has shown that 57.4% of adolescents with a history of self-harm reported suicidal ideas.11 And in a retrospective chart review study on psychiatric patients with NSSI and/or suicide attempts, 33.75% of the participants reported both NSSI and suicide attempts, 17.5% reported NSSI only, and 48.75% reported only suicide attempts.12 These findings indicate coexisting but distinguishable characteristics of NSSI and suicidality.
NSSI includes a wide range of behaviors such as cutting, scratching or carving one’s skin with a sharp object, hitting oneself, banging, burning, or substance abuse. As a high percentage of the population engages in NSSI and exhibits various self-harm behaviors, it seems necessary to pay attention to the heterogeneity within them and to provide differentiated interventions for specific subtypes. Forms of self-harm are explicit and comparably easy to assess via early interviews or self-report measures in clinical settings. This makes collecting information about them helpful in checking the characteristics of individuals exhibiting NSSI, including the lethality of their NSSI behaviors.
A few studies have demonstrated that the forms of NSSI are associated with psychological characteristics of individuals who engage in NSSI to help explain psychiatric heterogeneity in NSSI.51314 Andover et al.5 identified differences in psychiatric symptoms among individuals with different NSSI methods. They reported that individuals who adopted skin cutting exhibited higher anxiety than those who engaged in other forms of NSSI. In their latent class analysis (LCA) study, Klonsky and Olino13 found that a preference for aggressive forms of NSSI, such as hitting oneself, was prevalent in one class, while a preference for other forms of NSSI, such as cutting, was prevalent in another class. They have also reported significant differences between groups of individuals with a preference for specific NSSI forms: individuals who used hitting as their NSSI method showed lower levels of depression in comparison to those who adopted other forms of NSSI. Similarly, Kleiman et al.14 focused on trait aggression and predicted that individuals who engage in hitting would be different from those who engage in other forms of NSSI methods, such as cutting. In their large sample, higher levels of trait aggression differentiated those who engaged in self-hitting from those who did not, and levels of trait aggression were also associated with the frequency of self-hitting. Given this small but growing body of research, it is suggested that different factors are involved in different forms of NSSI. Unfortunately, previous research contained limitations in terms of ecological validity, as they are retrospective and mainly focused on limited numbers of self-harm behaviors and a few emotions such as aggression, depression, and anxiety. Therefore, more research is required to investigate the various forms of NSSI and the underlying factors (e.g., emotions, behaviors) influencing certain forms of NSSI with multifaceted measures.
In addition to the studies on the forms of NSSI, there is an increasing number of studies examining differences in self-harm behavior at the longitudinal level, not limited to retrospective cross-sectional methods such as interviews or self-reports. One of the early studies utilizing longitudinal assessment by Nock et al.15 investigated forms and functions of self-injurious thoughts and behaviors among adolescents and young adults via an ecological momentary assessment (EMA). A recent study that reviewed EMA research on NSSI16 has supported that research with intensive longitudinal data was distinguishable from the ones with cross-sectional data: the EMA studies had strength in investigating emotional and cognitive contexts of self-harm, self-harm motives, and temporal changes in psychological variables before and after self-harm behaviors. Furthermore, a few studies have predicted the proximal time of self-harm episodes based on emotional changes and devised preventive interventions for individuals exhibiting self-harm behaviors.1718 Therefore, it would be even more meaningful to verify the validity of the subtype of individuals exhibiting self-harm, by comparing the differences in emotions and behaviors in daily life according to the differences in the subtypes.
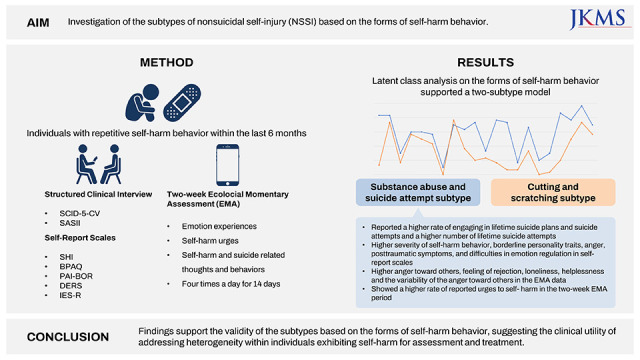
This study had two primary objectives. First, we aimed to identify forms of self-harm-based NSSI subtypes using an empirical classification approach. We administered latent class analysis on the items of the Self-Harm Inventory (SHI),19 which is a widely used and broad measure for self-harm to identify subtypes of NSSI. Second, we aimed to examine the validity of the subtypes by using: 1) baseline measures of relevant clinical variables and 2) EMA measures of emotion and self-harm-related variables. We compared the subtypes based on self-harm behaviors and investigated cross-sectional differences in psychosocial constructs relevant to NSSI. Intensive longitudinal data from a two-week EMA were used to examine the differences between subtypes in daily life. The data included real-time reports of participants on emotion experience, emotion variability, and urges to self-harm in their natural environment. By adopting EMA, an ecologically valid and clinically informative method,20 we expected to examine the extent to which the forms of self-harm-based subtypes were associated with significant differences in specific emotions. Based on the above analysis results, we propose an intervention method tailored to the characteristics of each subtype.
METHODS
Participants
The current study recruited adults aged 19 or older who repeatedly engaged in self-harm behavior within the last six months. All participants volunteered for this study and gave written informed consent after obtaining sufficient information regarding the study procedure. Individuals with developmental disorders, psychotic symptoms, and other neuropsychiatric disorders were excluded from participating in the study. Of the 65 individuals who voluntarily applied for the study, five participants who exhibited suggested psychotic symptoms were excluded from participating in the study after structured clinical interviews. As a result, 60 individuals were included in the final sample.
Measures
Clinical interviews
1. Structured Clinical Interview for DSM-5 Disorders Clinician Version (SCID-5-CV)
SCID-5-CV is a semi-structured interview that can be conducted by clinicians or trained mental health professionals, enabling systematic evaluation of major DSM-5 diagnoses. SCID-5-CV is a reliable and valid measure to diagnose mental disorders accurately.21 The Korean version of the SCID-5-CV, which was translated by Oh et al.,22 was adopted in the current study. We used questions in the SCID-5-CV to assess diagnoses, lifetime suicide planning, and suicide attempts in participants.
2. Suicide Attempt and Self-Injury Interview (SASII)
SASII is a structured interview developed by Linehan et al.,23 which comprehensively assesses factors related to self-harm behavior and suicide attempts. It intensively evaluates methods of suicide and self-harm, the lethality of the method, impulsiveness, suicidal intentions, and rescue possibilities and consequences of each self-harm behavior. In a review study,24 SASII showed the highest reliability among the measures for suicide attempts and self-harm behavior. The current study used the Korean version of the SASII, which was translated by a group of researchers, including the two authors (S. K. & J-S. L.) of this study.
Self-report measures
1. SHI
The SHI was developed by Sansone, Wiederman, and Sansone19 to measure intentional self-harm behavior. The Korean version of the SHI was validated by Kim, Woo, Koo, and Lee.25 It consists of 22 binary (Yes/No) questions on self-harm behaviors. A higher total score on the scale indicates engagement in many different self-harm behaviors. The internal consistency (Cronbach’s α) was 0.76 in the Kim et al.25 and 0.70 in the current study.
2. Buss-Perry Aggression Questionnaire (BPAQ)
The BPAQ is a self-report measure of aggression developed by Buss and Perry.26 The scale consists of 29 items on a 5-point Likert scale, ranging from 1 (extremely uncharacteristic of me) to 5 (extremely characteristic of me). The BPAQ has four empirically derived subscales: physical aggression, verbal aggression, anger, and hostility. We used the Korean version of the BPAQ validated by Lee,27 and the internal consistency (Cronbach’s α) was 0.89 in this study.
3. Personality Assessment Inventory-Borderline Features Scale (PAI-BOR)
The PAI-BOR is one of the 11 clinical scales of the Personality Assessment Inventory developed by Morey28 to evaluate adult personalities. It consists of 24 questions, including features of borderline personality disorder such as impulsivity/dyscontrol, mood instability, chronic emptiness, separation concerns, negative relations, and reckless spending. Items are rated on a 4-point Likert scale with items ranging from 0 (false) to 4 (very true). We used the Korean version of the PAI-BOR validated by Hong and Kim,29 and the internal consistency (Cronbach’s α) for the present study was 0.90.
4. Difficulties in Emotional Regulation Scale (DERS)
The DERS is a 36-item measure that assesses difficulties in emotion regulation.30 Items are rated on a 5-point scale ranging from 1 to 5; 1 is almost never (0–10%), 2 is sometimes (11–35%), 3 is about half the time (36–65%), 4 is most of the time (66–90%), and 5 is almost always (91–100%). Higher total scores indicate greater emotion dysregulation. The Korean version of the DERS was validated by Cho,31 which consists of six subscales: impulse control difficulties, lack of attention to and awareness of emotions, nonacceptance of emotions, lack of emotional clarity, limited access to emotion regulation strategies, and difficulties in engaging in goal-directed behavior, respectively. The present study’s internal consistency (Cronbach’s α) was 0.92.
5. Impact of Event Scales-Revised (IES-R)
The IES-R was developed by Weiss and Marmar.32 They revised the IES,33 which was designed to measure symptoms related to posttraumatic stress disorder. The IES-R consists of 22 items measuring intrusion, avoidance, hyperarousal, sleep problems, and numbness. The frequency of experienced symptoms over a period of a week is rated on a 5-point scale ranging from 0 (not at all) to 4 (extremely). We used the Korean version of the IES-R validated by Lim et al.34 The current study’s internal consistency (Cronbach’s α) was 0.91.
6. EMA
Based on previous studies on self-harm and suicide (e.g., Nock et al.15), we devised questions on emotions, thoughts, and urges related to self-harm and suicide. Participants were asked to respond to each question according to their experiences in their daily lives. The participants were given an ID and password and submitted their answers on a secured research web app via their smartphones. They were asked to mark their experienced emotion since the last online survey on their visual analog scale (VAS), ranging from 0 (not at all) to 10 (very much). In addition, participants reported their thoughts, urges, and behaviors related to self-harm and suicide since the last online survey.
Procedures
Participants were recruited by posting recruitment advertisements on Social Networking Services (SNS) (KakaoTalk, Instagram, Facebook, YouTube, etc.), online communities at universities, online cafes, and suicide prevention-related organizations. Those who volunteered for the study were contacted by a research assistant to check their history of repetitive self-harm. All participants were provided with sufficient information on the entire research procedure and signed a written consent form before their participation. In addition, participants accessed an encrypted web app using a personal ID and password to complete a packet of self-report measures, which took approximately 30 minutes and scheduled a structured interview. Clinical psychologists with a master’s degree or a Ph.D. conducted a structured interview using SCID-5-CV and SASII and gave a brief education on EMA. From the day after the interview, participants received text messages four times a day (10 a.m., 2 p.m., 6 p.m., and 10 p.m.) for 14 days and accessed an encrypted research web app to provide responses. In order to increase compliance, additional encouraging text messages were sent within 30 minutes of receiving the first text notification. Each online survey took an average of 2 minutes (ranging from less than 1 minute to 4 minutes, according to their experiences). Participants were fully debriefed and received pro-rata monetary compensation.
Statistical analysis
Descriptive analyses and subtype difference analyses were conducted using IBM SPSS, version 25.0 (IBM Corp., Armonk, NY, USA). To test group differences t-test was used for continuous variables, and χ2 test was applied for categorical variables. LCA was performed using Mplus version 7.35 LCA was used to discriminate homogeneous subtypes of NSSI based on their self-harm behavior. The LCA model included 21 dichotomous indicator variables, which were items of the SHI. The last item of the SHI (item 22. abused laxatives to hurt yourself) was excluded from the LCA since no participant endorsed it. These items reflected whether the participant had ever engaged in different forms of self-harm behavior. A step-by-step model class enumeration process was used. In each step, the number of the latent classes was increased by one. Better fitting models were those with relatively lower values for the Akaike Information Criterion (AIC),36 Bayesian Information Criterion (BIC),37 and Sample Size Adjusted Bayesian Information Criterion (SABIC).38 In addition, a significant Bootstrapped Likelihood Ratio Test (BLRT)39 implied that a particular k-class model showed a more optimal model fit than the previous k-1-class solution. Item endorsement probabilities helped with labeling latent classes. Entropy was used to inform classification accuracy.
After class enumeration, the association between latent classes and external variables was examined. Subtype differences were examined in terms of age, gender, level of education, histories related to self-harm, psychotherapy, and medication. Furthermore, subtypes contrasted in clinical variables, including self-esteem, borderline personality features, aggression, posttraumatic symptoms, and difficulties in emotion regulation on self-report measures. Lastly, means and variabilities of emotions and urges to self-harm in daily life collected by EMA were also used to contrast the subtypes. Cohen’s d was used as an effect size measure for subtype differences.
RESULTS
Demographic characteristics
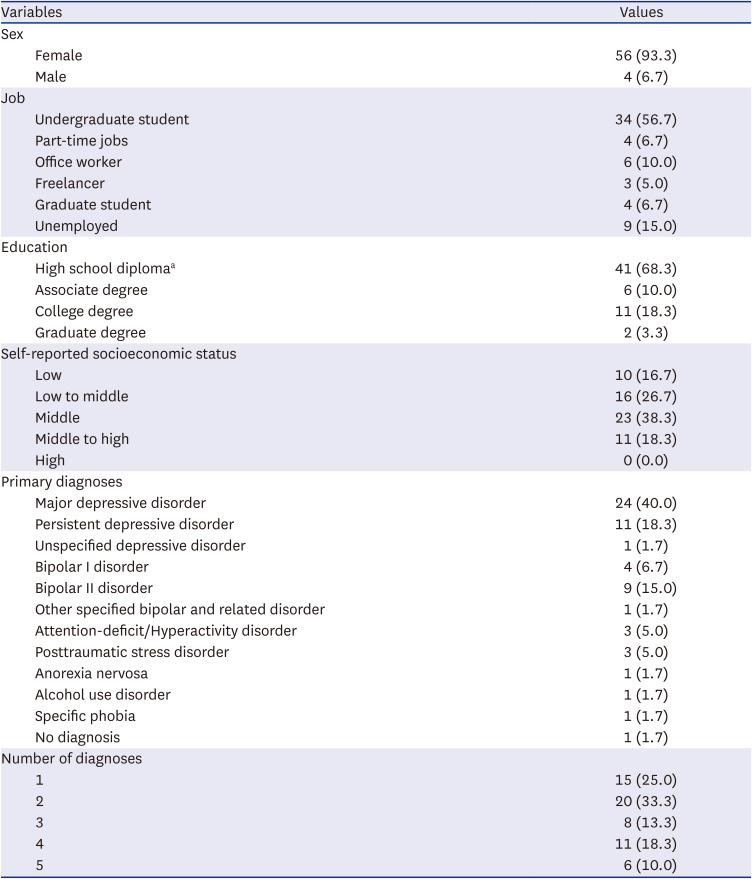
The mean age of the participants was 22.47 years (standard deviation [SD] = 3.35), ranging from a minimum of 19 years to a maximum of 36 years. Majority of the participants were female (n = 56, 93.3%). Among the participants, thirty-four (56.7%) were undergraduate students, nine (15%) were unemployed, four (6.7%) were part-time workers, four (6.7%) were graduate students, and four (6.7%) had other occupations. Clinical interviews via the SCID-5-CV showed that the mean number of psychiatric diagnoses was 2.57 (SD = 1.35). In terms of primary diagnosis, 49 participants were diagnosed with depressive disorders, which accounted for the highest percentage (81.67%): 27 had major depressive disorders, 14 had persistent depressive disorders, and eight had premenstrual dysphoric disorders. It was followed by 16 (26.67%) individuals with social anxiety disorders, 15 (25%) with trauma and stress-related disorders, including nine individuals with posttraumatic stress disorders, and six individuals with other specified trauma- and stress-related disorders. In addition, a total of 14 individuals (23.33%) had bipolar disorders, including four individuals with bipolar I disorder, nine people with bipolar II disorder, and one with unspecified bipolar and related disorder. For detailed information on the demographic characteristics of the participants (Table 1).
Table 1
Demographic statistics (N = 60)
Latent class analysis on the forms of self-harm behaviors
In order to determine the number of latent classes based on the SHI, the indices calculated by latent class analyses were examined. Table 2 displays fit indices for models with different numbers of latent classes. Models with two to four latent classes were estimated. The two-class solution showed the lowest values of AIC,36 BIC,37 SABIC,38 and BLRT.39 Furthermore, the significant BLRT result for the three-class model, followed by the nonsignificant BLRT result for the four-class model, indicated that an additional latent class over three subgroups did not significantly improve the model fit. Therefore, the two- and three-class models were considered. Considering the sample size and theoretical possibility of each group, the two-class model was considered the most suitable.
Table 2
Fit indices for the latent class analysis models based on the forms of self-harm behavior in the SHI

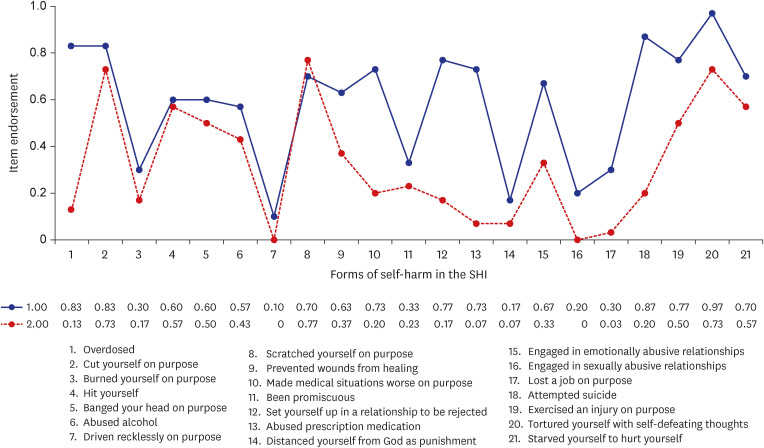
The two identified classes were labeled as substance abuse and suicide attempt (Class 1; n = 30; 50%) and cutting and scratching (Class 2; n = 30; 50%) subtypes, and the classes significantly differed regarding indicator variables on the SHI items (Fig. 1). The identified latent classes showed quantitative differences or severity-based differences in self-harm behaviors as well as qualitative differences that reflected different subtypes of self-harm. The substance abuse and suicide attempt subtype exhibited higher scores in overall items except item 8 (item 8. Scratching your body deliberately) when compared to the cutting and scratching subtype. Inter-class differences were observed in the items on drug abuse, suicide attempt, and setting oneself in non-rewarding circumstances (item 1. Overdosed, item 12. Set yourself up in a relationship to be rejected, item 13. Abused prescription medicine, and item 18. Attempted suicide). For these items, the substance abuse and suicide attempt subtype showed significantly higher endorsement than the other subtype (endorsement rate of class 1–class 2 > 0.60). The cutting and scratching subtype was characterized by high scores in items 2, 4, 8, 20, and 21 (item 2. Cut yourself on purpose, item 4. Hit yourself, item 8. Scratched yourself on purpose, item 20. Tortured yourself with self-defeating thoughts, and item 21. Starved yourself to hurt yourself). The substance abuse and suicide attempt subtype showed the highest endorsement rates in items 1, 2, 18, and 20 (item 1. Overdosed, item 2. Cut yourself on purpose, item 18. Attempted suicide, and item 20. Tortured yourself with self-defeating thoughts). Both subtypes showed a simultaneous rising in items 2, 8, and 20 (item 2. Cut yourself on purpose, item 8. Scratched yourself on purpose, and item 20. Tortured yourself with self-defeating thoughts).
Differences between subtypes of demographic data and self-reported measures
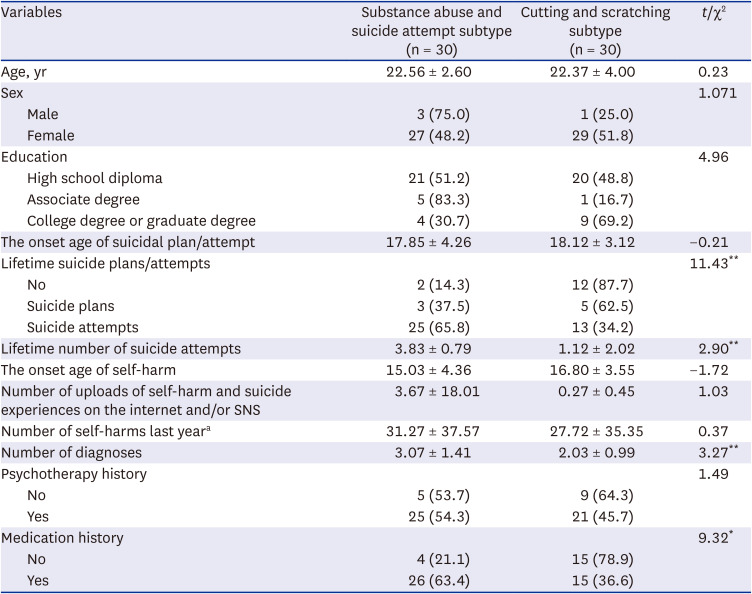
Subtype differences were investigated in demographic data such as age, gender, level of education, and psychiatric histories, including self-harm-related histories such as the onset age of suicidal plan/attempt, number of uploads of self-harm and suicide experiences on the internet and/or SNS, number of self-harms in the previous year, lifetime suicide plans and suicide attempts, lifetime number of suicide attempts and histories of psychotherapy and medication (Table 3). Results demonstrated no subtype differences in age, gender, or level of education, all P > 0.05. Among the psychiatric histories, lifetime suicide plans and attempts, lifetime number of suicide attempts, the number of diagnoses and medication history were significantly different. The substance abuse and suicide attempt subtype engaged in lifetime suicide plans and attempts more frequently (χ2 = 11.43, P = 0.003) and reported higher numbers of lifetime suicide attempts (t = 2.90, P = 0.005). They also showed a higher number of diagnoses (t = 3.27, P = 0.002), and higher endorsement in medication history (χ2 = 9.32, P = 0.002).
Table 3
Differences between subtypes in demographic data (N = 60)
In terms of self-report measures, t-tests were conducted to find inter-subtype differences in self-esteem, borderline personality characteristics, aggression, posttraumatic symptoms, and difficulties in emotion regulation. Results showed that mean scores of the substance abuse and suicide attempt subtype were significantly higher than those of the cutting and scratching subtype in terms of borderline personality characteristics (t = 3.64, P = 0.001), aggression (t = 3.07, P = 0.003), posttraumatic symptoms (t = 2.91, P = 0.005), and difficulties in emotion regulation (t = 2.05, P = 0.045). No significant difference in self-esteem was identified between the two subtypes (t = −0.60, P = 0.55) (Table 4).
Table 4
Differences between the subtypes in self-report measures
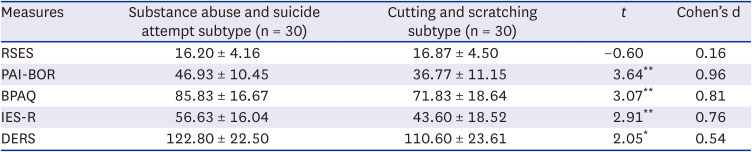
Values are presented as mean ± standard deviation.
RSES = Rosenberg Self-Esteem Scale, PAI-BOR= Personality Assessment Inventory-Borderline Features Scale, BPAQ = Buss-Perry Aggression Questionnaire, IES-R = Impact of Event Scales-Revised, DERS = Difficulties in Emotional Regulation Scale.
*P < 0.05, **P < 0.01.
Differences in emotions and urges to self-harm in daily life
Emotion experiences and emotion variabilities in daily life
In order to investigate the differences in emotion experiences and emotion variabilities in daily life, inter-subtype differences in EMA data on discrete emotions were compared via t-tests. Scores of emotions at each time point in the EMA during the two-week period were averaged to calculate the means of the emotions, and the variances were also calculated to investigate the variability of the emotions for each subtype.
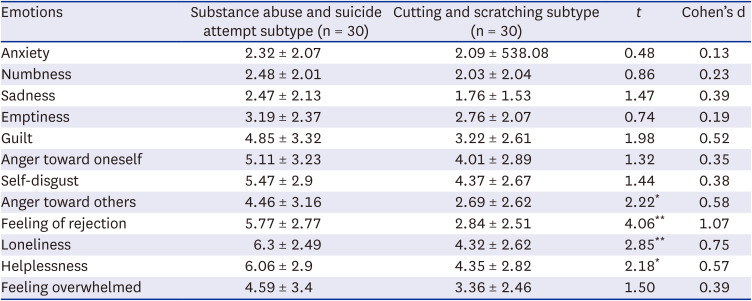
Results of the t-tests on the mean level of emotion experiences in EMA demonstrated that the substance abuse and suicide attempt subtype showed significantly higher scores in anger toward others (t = 2.22, P = 0.031), feeling of rejection (t = 4.06, P < 0.001), loneliness (t = 2.85, P = 0.006), and helplessness (t = 2.10, P = 0.042) when compared to the cutting and scratching subtype. There were no significant differences in other items, all P > 0.05 (Table 5).
Table 5
Differences between the subtypes in emotion experiences in daily life
Further, to examine the inter-subtype differences in the variabilities of emotions, t-tests were conducted. Results showed a significant difference in anger toward others (t = 2.04, P = 0.046, d = 0.54), which indicated that the degree of changes in anger toward others was greater in the substance abuse and suicide attempt subtype than that of the cutting and scratching subtype. There were no significant differences in other items, all P > 0.05.
Urges to self-harm in daily life
The difference between the two subtypes in the presence of urges to self-harm with or without suicidal intent for a two-week EMA period was investigated via cross-analysis. Of the total sample, four individuals who did not respond to the question were excluded, and data from the remaining 56 individuals were analyzed. More than half of the participants reported having the urge to self-harm at least once during the two-week EMA period (n = 29, 51.8%). Results of the cross-analysis indicated that there was a significant difference in the frequency of urges to self-harm between the two groups (χ2 = 7.212, P = 0.007): Among the total of 27 individuals in the substance abuse and suicide attempt subtype, approximately 70% of the individuals reported the urge to self-harm (n = 19, 70.4%), while only 34.5% of the 29 individuals in the cutting and scratching subtype reported urges in the same two-week EMA period (n = 10, 34.5%). The results indicate that the individuals in the substance abuse and suicide attempt subtype were more likely to develop the urge to self-harm compared to the cutting and scratching subtype in their everyday lives (Table 6).
Table 6
Differences between subtypes in the urges to self-harm in daily life

DISCUSSION
The current study identified subtypes of NSSI based on the forms of self-harm behavior in the Korean community adult sample and provided evidence of their validity using baseline psychological variables in self-reports and naturalistic data on emotion experience, emotion variability, and the urge to self-harm via EMA. The LCA yielded two subtypes: substance abuse and suicide attempt subtype and cutting and scratching subtype. The first subtype was characterized by more severe symptoms in overall self-harm behaviors, and especially substance abuse, relational problems, and suicide attempts were highly reported among them. In contrast, the second subtype showed lower probabilities in endorsements of self-harm behaviors and mainly endorsed cutting and scratching. The two subtypes were significantly different in their psychiatric history, clinical variables in self-report measures, and everyday emotions and urge to self-harm in EMA.
Previous literature has categorized self-harm behavior in accordance with the severity of their forms. Mild forms of self-harm include hitting oneself, picking one’s wounds, and banging, while moderate/severe forms of self-harm consist of cutting, carving one’s skin, burning, and substance abuse40. Both subtypes provided by the LCA in the current study were mainly endorsed in moderate/severe forms of self-harm rather than mild forms. This finding might be relevant to the characteristics of our sample, which were young adults in the community. Compared to early adolescents who start to engage in NSSI, adults have a higher possibility of having a long history of NSSI engagement and adaptation to more severe methods.1341 Considering the early onset age of self-harm identified within our sample (mean age, 15. 92 ± 4.04 years), the self-harm methods of participants may have evolved into more serious forms over time. In addition to the general characteristics of our sample, there were significant differences between subtypes. The substance abuse and suicide attempt subtype showed a higher probability of endorsing a broad range of self-harm behaviors and was characterized by more severe methods, including substance abuse and suicide attempts. These results correspond with previous findings, which state that individuals who use various and more severe self-harm methods tend to show a higher risk of suicide attempts.13
At the item level, the most evident differences between the two subtypes were found in items 1, 10, 12, 13, and 18 (item 1. Overdose, item 10. Making medical situations worse on purpose, item 12. Setting oneself up in a relationship to be rejected, item 13. Abused prescription medication, and item 18. Attempted suicide). The substance abuse and suicide attempt subtype showed more lethal self-harm behaviors, which could lead to irreversible consequences such as substance abuse, injuring oneself, and ultimately, suicide attempts. In addition, they tend to use passive coping behaviors and maladaptive interpersonal behaviors (e.g., setting themselves in a relationship to be rejected, preventing wounds from healing, and making medical situations worse on purpose). These features may reflect complex problems in personality and deficits in coping resources underlying self-harm in the substance abuse and suicide attempt subtype.
Significant differences in psychiatric history, self-report measures, and EMA data supported the differences between the two subtypes. First, in psychiatric history, the substance abuse and suicide attempt subtype showed a higher endorsement of lifetime suicide plans and suicide attempts and a higher number of lifetime suicide attempts. These results supported the findings from the LCA on the SHI in this study that a higher risk of suicide can characterize the substance abuse and suicide attempt subtype. Moreover, this subtype demonstrated a higher number of diagnoses and higher endorsement of medication history than the cutting and scratching subtype. These findings suggest that the substance abuse and suicide attempt subtype tend to have more comorbid disorders other than self-harm itself, which means that they may have more complicated psychological problems and are more likely to visit clinical settings where medication is available. It not only shows their severity of impairment but also supplies a clinical implication in the treatment. Considering the high endorsement of overdose and abuse of prescription medication of this subtype, it is suggested that clinicians pay more attention to guiding and monitoring the medication of their patients who exhibit self-harming behaviors.
Second, the substance abuse and suicide attempt subtype also showed significantly higher scores on the majority of psychological measures: scales on the borderline personality trait, anger, posttraumatic symptoms, and difficulties in emotion regulation, except for one measure on self-esteem. As supposed by the data on psychiatric history, the substance abuse and suicide attempt subtype had more serious personality problems, psychological symptoms, and difficulties in emotion regulation. However, the finding that the two subtypes did not differ in self-esteem was unexpected, as negative self-cognition is one of the cardinal risk factors of self-harm.4243 Our conjecture is that this finding might be related to the fact that both subtypes share common characteristics as self-harm subtypes. Since negative self-cognition is pervasive among individuals who exhibit self-harm, all participants in our study who engaged in repetitive self-harm behaviors have reported low levels of self-esteem. Furthermore, it could be due to the limitation of the measure on general self-esteem. Previous research on self-cognition has examined more specific constructs such as self-criticism, self-disgust, or self-punishment.434445 Therefore, it would be meaningful to examine the subtype differences in those self-related constructs in future research.
Lastly, the two subtypes were different in their experiences of emotion and the urge to self-harm in daily life. On the mean level of the emotion experience in EMA data, the substance abuse and suicide attempt subtype showed higher scores in anger toward others, feeling of rejection, loneliness, and hopelessness, than the other subtype. On emotion variability, a significant subtype difference was observed only in anger toward others. Other emotions, such as depression, anxiety, anger toward oneself, self-disgust, emotional numbness, sadness, emptiness, and guilt did not differ between the two subtypes. These results reported that neurotic emotions such as depression, anxiety, and negative emotions toward oneself did not show significant inter-subtype differences, while anger toward others, loneliness, and feeling of rejection was higher in the substance abuse and suicide attempt subtype, suggesting that they may have insecure and negative interpersonal perception. Also, the fact that their hopelessness was higher might be related to the chronicity of experienced problems and lack of coping resources.46 Furthermore, in the two-week real-time tracking of urges to self-harm in daily life, the substance abuse and suicide attempt subtype reported a significantly higher probability of urges to self-harm, which was almost double the number than in the cutting and scratching subtype, which strongly implies that their emotional vulnerabilities increase the risk of self-harming behaviors via the urge to self-harm.
In conclusion, it is suggested that forms of self-harm behavior can identify subtypes of NSSI, and individuals with more severe symptoms are characterized by more severe psychological symptoms, difficulties in emotion regulation, and unstable interpersonal relationships. Previous research found that individuals who engage in self-harm while also having borderline personality disorder were distinctive from those without borderline personality disorder.414748 Individuals with borderline personality disorder present a variety of symptoms which include identity disturbance, unstable and intense interpersonal relationships characterized by alternating between extremes of idealization and devaluation, impulsivity, affective instability, chronic emptiness, inappropriate and intense anger, and frantic efforts to avoid real or imagined abandonment.49 They show pervasive patterns of these problems, making interventions for borderline personality disorder difficult. Corresponding with the suggestions from previous research, which stated that differentiated approaches should be given to self-harm groups with and without borderline personality traits,4750 the results of this study support the need to assess personality traits and problems in coping skills and to provide specialized interventions for each subtype of self-harm. Furthermore, intensive behavioral and cognitive interventions for emotion regulation are required to prevent lethal self-harm behaviors for each subtype.
This study contributes to the literature as it examines the ecological difference between the two subtypes in daily life by analyzing intensive longitudinal data obtained via EMA as well as conducting self-report measures and clinical interviews. It was particularly meaningful that the two subtypes were identified based on a broad range of direct and indirect self-harm behaviors, and the validity of the subtypes was confirmed with both real-time and retrospective data.
There are also some limitations to note in this study. We had a small sample size, and the majority of our participants were females in their twenties. We welcome future research to examine the subtypes of self-harm that we found in the study with a larger sample, including males who engage in self-harm and recruit clinical and community samples to increase the generalizability of these research findings.
 XML Download
XML Download