

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In recent years, colonoscopy has been widely used and highlighted as a screening tool for colorectal cancer.123 Proper bowel preparation is an essential prerequisite for high-quality colonoscopy, because inadequate bowel preparation can result in difficulties during polypectomy. Inadequate bowel preparation can also lead to missed polyps, resulting in interval colorectal cancers.4 Moreover, inadequate bowel preparation causes difficulties with colonoscope insertion and increases complication rates.567
Factors known to be associated with inadequate bowel preparation include increased body weight, male sex, high BMI, age >60 years, previous abdominal surgery, liver cirrhosis, Parkinson's disease, underlying diseases (such as diabetes), and constipation.891011 Bowel preparation can sometimes take longer in patients with chronic constipation than in those with normal bowel movement patterns.
The prevalence of chronic constipation has increased by 16.5% in Korea, Europe, and the United States. This is especially true in elderly patients, who represent a population who frequently undergo colonoscopies.12 A method of predicting the level of bowel preparation in patients with chronic constipation leading to proper bowel preparation would be very useful for increasing the rates of successful colonoscopy. The factors affecting bowel preparation have been assessed in many studies.891011 However, there are few reports of measurable or reproducible predictors of bowel preparation.1113 In particular, there have been no studies on the prediction of bowel preparation in patients with chronic constipation with a history of poor bowel preparation.
The colonic transit time (CTT) test, one of the basic methods of assessing the motor function of the large intestine, is widely used for patients with chronic constipation. This test can easily measure the transit time of each segment of the entire colon, provide objective information regarding abnormal bowel function, help in designing appropriate treatment plans, and determine disease classification based on the pathophysiology of chronic constipation.1415 We hypothesize that deceased bowel movements could lead to less effective wash out of bowel preparation solution followed by inadequate bowel preparation. We conducted this study to assess if CTT measured prior to scheduled colonoscopy can predict the degree of bowel preparation in patients with chronic constipation.
METHODS
This retrospective study was performed by reviewing the records of 160 patients who had visited Wonju Severance Christian Hospital from March 2007 to November 2012 for chronic constipation evaluations. The study was approved by the Institutional Review Board of Yonsei University Wonju Severance Hospital. Chronic constipation was diagnosed according to the ROME II diagnostic criteria, and all patients underwent colonoscopy and a CTT test.16
1. CTT Measurement
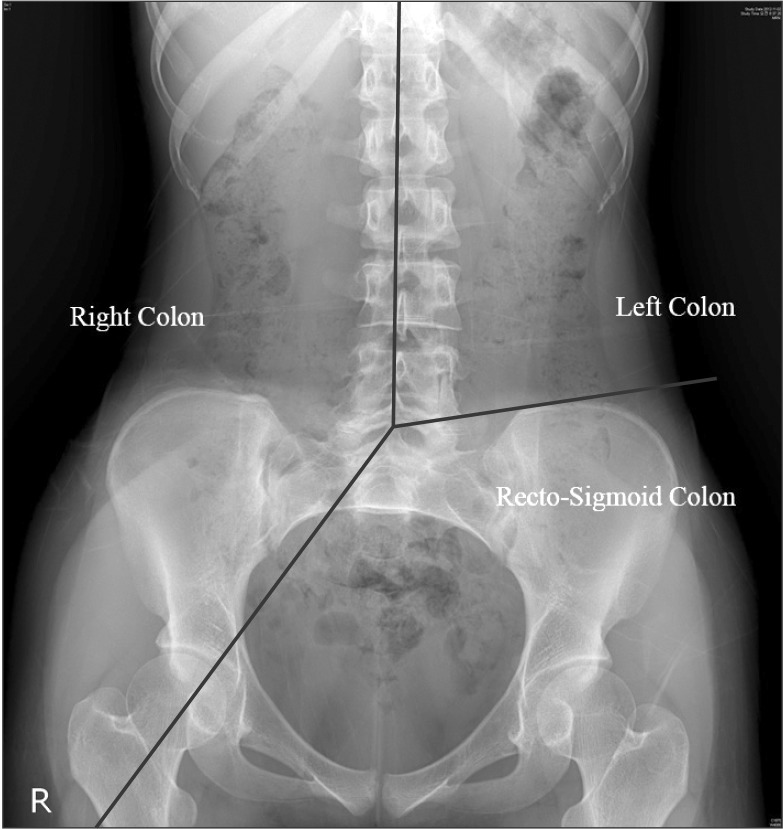
CTT was measured on days 4 and 7 using multiple radioopaque markers. Bowel preparation state was predicted by measuring markers on days 4 and 7. A single tablet of Kolomark™ (M. I. Tech, Pyeongtaek, Gyeonggi, Korea) containing 20 small rings was taken with water once per day for 3 days at 9 AM, and simple abdominal radiographs were taken at 9 AM on days 4 and 7. The right colon was identified on simple abdominal radiographs using two guidelines: one that connected all the spinous processes of the vertebrae and another that crossed from the 5th lumbar vertebral body to the right pelvic outlet. To identify the left colon, a line was drawn to connect all of the spinous processes, and the second line was drawn from the 5th lumbar vertebral body to the left anterior superior iliac spine. The portion of the colon within this plane was determined to be the left colon. A plane below these two lines, composed of a line that connected the right pelvic outlet and a second line that crossed the left anterior superior iliac spine, was determined to be the location of the rectum and sigmoid colon (Fig. 1).17 CTT was assessed by counting the number of radio-opaque markers on a plain radiogram on day 4. These numbers were multiplied by 1.2 and added to the number of radio-opaque markers counted on day 7.18 An average CTT has not been clearly determined for the Korean population, and previous studies have used various standards. However, recent studies have settled on a mean CTT of 30 hours.51920
Based on the results of these studies, we classified patients with a CTT of >30 hours as the slow transit time (STT) group, and those with a CTT of <30 hours as the normal transit time (NTT) group. Furthermore, no standard transit time has been determined for cases of pelvic outlet obstruction, which delays passage through the sigmoid colon and rectum. Based on the mean CTT in each segment, we used 20 hours as the mean right and left CTT, and 10 hours as the mean transit time for the rectum and sigmoid colon. Slow transit constipation was diagnosed in people with a >20-hour delay in transit time in both right and left colons. Those with a transit time postponed by >10 hours in the rectum and sigmoid colon were defined as having pelvic outlet obstruction.
2. Bowel Preparation
All patients were instructed to avoid fiber-rich foods, fruits with seeds, and some grains for 3 days. They also took 4 L of PEG as a split dose: 2 L of solution in the evening before the procedure, and 2 L of solution the next morning at 8 am. Colonoscopies were performed within 5-7 hours after the end of bowel preparation. We enrolled patients who had finished their bowel preparation on schedule. To determine a bowel preparation scale without bias, all recorded colonoscopic images were reevaluated by one experienced physician (>5,000 colonoscopies). The medical record of each patient was also reviewed, and previous medical histories, previous colonoscopy reports, and pathologic findings were investigated.
The Boston Bowel Preparation Scale (BBPS) was used to evaluate the extent of bowel preparation. The scale splits the colon into three segments: the right, left, and transverse colons. Bowel preparation was measured on a scale from 0 to 3 in each segment. A part of the colon in which the mucosa cannot be observed on colonoscopy was given 0 points. When the mucosa could be clearly observed throughout the colon, the segment was given 3 points. Scores from each segment were added together, and the mean score was 6. Using a score of 6 as a reference, patients who received >6 points were classified as having proper bowel preparation, and patients who had <6 points in total or <2 points for one of any three segments were classified as having inadequate bowel preparation.20
3. Statistics
SPSS version 20.0 (SPSS Inc., Chicago, IL, USA) was used for all statistical analyses. Demographics and medical histories were assessed using a descriptive statistics method. The frequencies and ratios of categorical variables were determined and analyzed using Pearson's chi-square or Fisher's exact test. The mean, minimal, and maximal values of continuous variables were described, and values were analyzed using Student's t-test. A P-value <0.05 was considered statistically significant. Pearson's correlation coefficient was used to analyze the correlations between BBPS and CTT. A receiver operator characteristic (ROC) curve was drawn to determine which BBPS scores could best predict bowel preparation quality.
RESULTS
1. Patient Characteristics
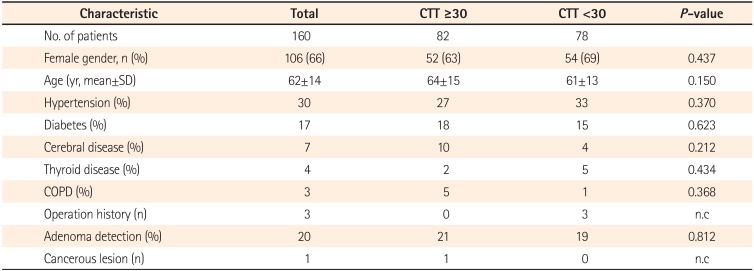
We analyzed a total of 160 patients with chronic constipation. There were 82 patients in the STT group (≥30-hour CTT), and 78 patients were classified in the NTT group (<30-hour CTT). Sixty-six percent of all patients were female, but no statistical differences in sex distributions (percentages of female patients) were observed between the two groups (STT vs. NTT, 63% vs. 69%; P=0.437). The mean patient age was 62±14 years. There were no differences in patient age between the two groups (STT vs. NTT, 64±15 years vs. 61±13 years; P=0.150). The proportions of patients with hypertension (STT vs. NTT, 27% vs. 33%; P=0.370) or diabetes (STT vs. NTT, 18% vs. 15%; P=0.623) determined from medical histories were not significantly different between the two groups. The proportions patients with neurovascular diseases including Parkinson's disease (STT vs. NTT, 10% vs. 4%; P=0.212), thyroid diseases including thyroid cancer (STT vs. NTT, 2% vs. 5%; P=0.434), and chronic obstructive pulmonary disease (STT vs. NTT, 5% vs. 1%; P=0.368), and history of abdominal surgery did not show any statistically significant differences between the two groups. Adenoma was identified in 32 patients (20%), but adenoma detection rate showed no significant difference between the two groups (STT vs. NTT, 21% vs. 19%; P=0.812). During colonoscopy, colon cancer was found in one patient from each group (Table 1).
2. Comparison of CTT and BBPS
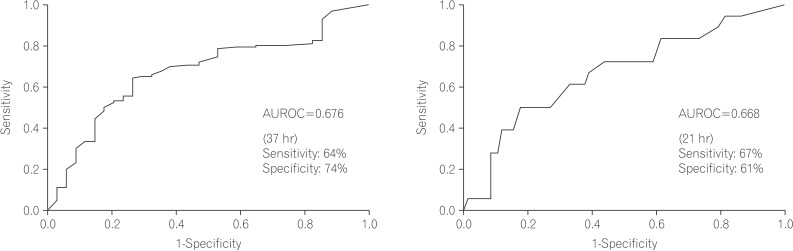
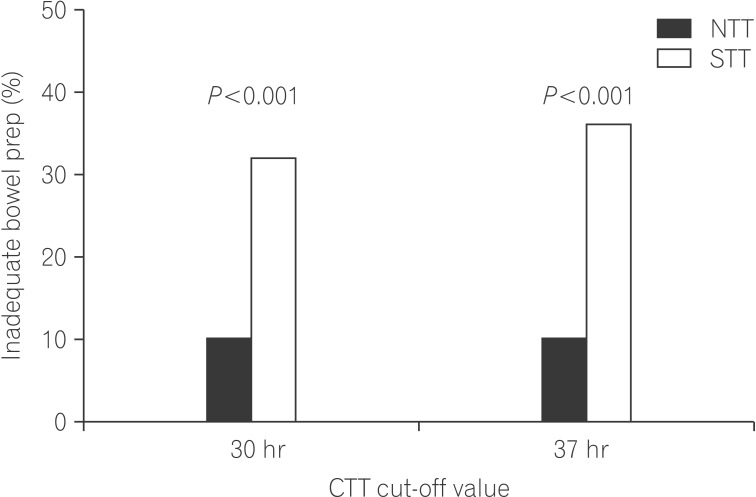
With reference values set to a mean CTT of 30 hours and a mean BBPS score of 6, the proportions of patients with a BBPS <6, reflecting inadequate bowel preparation, were 10.3% and 31.7% in the NTT and STT groups, respectively. The rate was 3-times higher in the STT group, and this difference was statistically significant (P=0.001) (Fig. 2). There was also a significant difference in the mean values of BBPS scores between the two groups (STT vs. NTT, 6.1±1.5 vs. 7.0±1.2; P<0.001). Although age, sex, history of diabetes, neurovascular diseases including Parkinson's, thyroid diseases, and CTT (reference, 30 hours) were found to be related to inadequate bowel preparation in other studies, this study showed that CTT was the only factor associated with inadequate bowel preparation(OR, 0.261; 95% CI, 0.107-0.634; P=0.003). Using ROC curve analysis, we found that a cut-off CTT of 37 hours could predict inadequate bowel preparation with 0.735 specificity and 0.643 sensitivity. This method was a more effective predictor of bowel preparation than CTT (area under the ROC curve: 0.676) (Fig. 2A). When the reference value for CTT was changed to 37 hours, the inadequate bowel preparation rates were 10.0% in the NTT group and 35.7% in the STT group, representing a larger difference (Fig. 3).
3. Comparison Between the Groups and Subgroup Analysis
Subgroup analysis was performed in the STT group. Those with a >20-hour delay in the transit times of the right and left colons were classified as the slow transit constipation group, and those with a >10-hour delay in the rectum and sigmoid CTT were classified as the pelvic outlet obstruction group. The slow transit constipation group included 82 patients, while the pelvic outlet obstruction group contained 57 patients. The number of patients with both slow transit constipation and pelvic outlet obstruction was 46. Because most pelvic outlet obstruction patients had mixed-type constipation, 11 were diagnosed with pelvic outlet obstruction only. All patients were then further divided into three groups: group A (only slow CTT), group B (only pelvic outlet obstruction), and group C (mixed constipation types). When each group was compared with the NTT group, the relationship between CTT and inadequate bowel preparation revealed statistically significant differences for groups A and C, which included patients with slow transit constipation (group A vs. NTT group, 26.0% vs. 9.4%; P=0.027) (group C vs. NTT group, 30.4% vs. 9.4%; P=0.008). However, group B showed no statistically significant relationship between inadequate bowel preparation and CTT (group B vs. NTT group, 18.0% vs. 9.4%; P=0.593).
DISCUSSION
Inadequate bowel preparation decreases the effectiveness of colonoscopy due to difficulties in colonoscope insertion and retrieval, and by increasing the chances of missing small and large colorectal polyps.61821 Additional testing due to inadequate bowel preparation leads to significantly increased national healthcare costs.21 Inadequate bowel preparation rates have been reported at between 20% and 30%, but this number may differ depending on the standards used.89101122 In the present study, inadequate bowel preparation was reported in 21.3% of cases, and this rate was similar to the results of previous studies.
Although previous studies have demonstrated factors causing inadequate bowel preparation, predicting the exact state of bowel preparation by these factors alone still has limitations. In particular, inadequate bowel preparation is frequently observed in patients with chronic constipation. However, there are no measurable and efficient tools to predict bowel preparation quality appropriately prior to colonoscopy.8 Hassan et al. reported that using a model incorporating a combination of factors, it is possible to predict the degree of bowel preparation with 60% sensitivity and 59% specificity.10 However, it is doubtful whether these factors could be uniformly applied to patients of all races and genders. Fatima et al. reported that it is possible to predict inadequate bowel preparation using a description of the patient's last stool, but this method depends entirely on the patient's personal description and may not be objective.13 Therefore, we tried to determine an accurate and objective method of predicting inadequate bowel preparation in patients with chronic constipation (those who are most likely to experience inadequate bowel preparation).
In this study, we focused on CTT as a predictor of inadequate bowel preparation in chronic constipation patients. Delayed CTT was shown to be the best predictor of inadequate bowel preparation in these patients. There is no standard reference CTT because this metric shows wide variations according to age, sex, ethnicity, and environment. In general, CTT is longer in women than in men, and in Western than in Eastern patient populations.519 Ina domestic study, the average CTT in healthy adults was found to be 20.5-30.3 hours.23
In this study, we used 30 hours as a reference to classify normal and delayed CTT. The sensitivity and specificity of using 30 hours as the standard for predicting inadequate bowel preparation were 74% and 56%. ROC curve analysis determined that the best specificity and sensitivity (74% and 64%, respectively) were obtained at 37 hours.
Patients with delayed CTT were divided into two groups: patients with delayed left to right movement within the colon (slow transit group),and patients with delayed transit in the recto-sigmoid colon (pelvic outlet obstruction group). Inadequate bowel preparation was significantly associated with the slow transit group, but was not related to the pelvic outlet group even though the test was performed in a small number of patients. This means that in patients with slow transit constipation, the main physiological characteristic of inadequate bowel preparation is slow CTT. It also shows that constipation due to pelvic outlet obstruction is not the cause of inadequate bowel preparation. In the case of patients with slow transit constipation, left to right CTT can predict inadequate bowel preparation, and showed the best specificity and sensitivity (61% and 67%) at 21 hours under ROC curve analysis (Fig. 2B).
Studies have shown that some drugs, such as magnesium hydroxide24 and bisacodyl, could be helpful for bowel preparation in patients with constipation, especially those with slow CTT.2526 Therefore, we suggest that these medications could be helpful for bowel preparation in patients with slow CTT.
There are a number of limitations to the present study. The study was retrospective in design and included a relatively small number of patients (160). In addition, because of a lack of previous data, we did not include clinical data such as Bristol stool scale scores, frequency of bowel movements, and drug history, which may be important for predicating inadequate bowel preparation. Therefore, the relevant factors known to be associated with inadequate bowel preparation may not be properly reflected in our analysis, and it is possible that these known factors were not fully taken into account due to the small patient population. Furthermore, some bias may be present due to the patient selection method used. In this study, diagnosis of constipation was performed in accordance with the Rome II diagnostic criteria, but some data pertaining to the symptoms of IBS were missing. Therefore, it is possible that IBS was misdiagnosed as chronic constipation in some patients. For these reasons, future large-scale prospective studies are necessary to validate the results of this study, and to create a new model that can more accurately predict the degree of bowel preparation using CTT and several other factors.
In conclusion, despite the inherent limitations of retrospective studies, this study shows that CTT measurement in patients with chronic constipation is a good method of predicting the level of bowel preparation before colonoscopy. CTT measured prior to colonoscopy may be useful for developing individualized strategies for bowel preparation in patients with slow CTT who are likely to experience inadequate bowel preparation.
 XML Download
XML Download