

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a highly contagious and pathogenic virus first discovered in December 2019 that caused a global pandemic of respiratory disease named coronavirus disease 2019 (COVID-19).12 Risk factors including old age, diabetes mellitus, chronic pulmonary disease, cardiovascular disease, chronic kidney disease, hypertension, obesity, metabolic disease, and smoking have been linked to higher risk of COVID-19.234567 Fortunately, several drugs have been proposed to have potential effects against COVID-19.8
Histamine-2 receptor antagonists (H2RA) and proton pump inhibitors (PPI) are acid suppressants most widely used for the management of gastrointestinal disorders. Gastric acid is a major defense mechanism against diverse pathogens including SARS-CoV-1. The activity of the SARS-CoV-1 spike protein, which enables the virus to attach and fuse into human cells, is sensitive to differences in pH conditions.9 Darnell et al. reports that highly acidic conditions of pH 1 and 3 inactivates SARS-CoV-1.9 In contrast, Jimenez et al. reports that acidic pH may increase susceptibility to SARS-CoV-2 infection. Lower pH associated with Barrett’s esophagus can drive increased expression of angiotensin-converting enzyme 2 (ACE2), the functional receptor through which SARS-CoV-2 enters the host cell. In addition, human monocytes cultured in acidic pH show increased expression of ACE2 and higher viral load of SARS-CoV-2.10
To date, the impact of acid suppressants on the risk of SARS-CoV-2 infection and severity of COVID-19 is not clearly understood. Previous studies identifying the association between the use of H2RA or PPI and the incidence111213141516 and clinical outcomes7121315171819202122 of COVID-19 report inconsistent results and vary widely in study design including study population, definition of acid suppressant use, adjusted covariates, and study period. Evaluating the potential impact of acid suppressants on COVID-19 would have substantial benefits considering the popular use of the drugs and the global health burden of COVID-19.
In this study, we used a population based, large-scale nationwide cohort in South Korea with propensity score matching to identify the effect of acid suppressants PPI and H2RA on susceptibility to SARS-CoV-2 infection and clinical outcomes of COVID-19. This study included data from the Korean National Health Insurance Service (NHIS) claims database and general health examination results.
METHODS
Data source
We performed a large-scale, population based nationwide cohort study using the Korean NHIS claims database, which is linked to the Korea Centers for Disease Control and Prevention data. During the COVID-19 pandemic, the South Korean government provided a claims database that included all individuals who underwent tests for SARS-CoV-2 between 1 January and 4 June 2020 in South Korea. The database includes inpatient and outpatient healthcare records (healthcare visits, prescriptions, diagnoses, procedures, and surgeries), pharmaceutical visits, insurance eligibility data, and general health examination results within the past 3 years.2324
Study population
The study population consisted of individuals aged 20 years or older who underwent testing for SARS-CoV-2 during the study period (1 January 2020 to 4 June 2020). SARS-CoV-2 infection was confirmed by a positive result from a real-time reverse transcriptase-polymerase chain reaction (RT-PCR) assay of pharyngeal and nasal swabs. The date of the first test for SARS-CoV-2 in each patient was defined as the index date.1225 H2RA and PPI users were defined as patients prescribed H2RA (famotidine, cimetidine, nizatidine, and ranitidine) or PPI (dexlansoprazole, esomeprazole, ilaprazole, lansoprazole, omeprazole, pantoprazole, and rabeprazole) within 1 year of the index date. Non-users were defined as individuals who were not prescribed either H2RA or PPI within 1 year of the index date. Individuals who were prescribed non-steroidal anti-inflammatory drugs (NSAIDs) within 30 days of the index date were excluded. This was because H2RA or PPI may have been initiated with NSAIDs in patients with early pneumonia symptoms,1226 Patients prescribed both H2RA and PPI within 1 year prior to the index date were excluded. Patients who tested negative for SARS-CoV-2 during the study period but were found to be positive in tests performed after the study period were also excluded.
Study outcome
The primary outcome was SARS-CoV-2 test positivity among individuals who underwent testing for SARS-CoV-2. Clinical outcomes of COVID-19, including death, intensive care unit (ICU) admission, and mechanical ventilation administration, in patients who tested positive for SARS-CoV-2 within 2 months of diagnosis were also evaluated.412
Data collection
We identified the claims data from the NHIS and combined them with the demographic data and general health examination results. Underlying comorbidities such as diabetes mellitus, hypertension, chronic pulmonary disease, chronic heart disease, cerebrovascular disease, renal disease, peripheral vascular disease, dementia, rheumatic disease, liver disease, malignancy, and dyslipidemia were identified by the presence of two or more claims within a year prior to the index date using International Classification of Diseases, 10th Revision (ICD-10) code.12 The Charlson Comorbidity Index (CCI) was calculated as a proxy of underlying disease burden using the ICD-10 codes as previously described,12 and the study population was classified into four groups according to CCI score: 0, 1, 2, and ≥ 3.1227 For type 2 diabetes mellitus, hypertension, and dyslipidemia, general health examination records were also used to define the comorbidities: E11–14 with antidiabetic medications or fasting blood glucose ≥ 126 for type 2 diabetes mellitus; I10–13 or I15 with antihypertensive medications, systolic blood pressure (SBP) ≥ 140, or diastolic blood pressure (DBP) ≥ 90 for hypertension; and E78 with antihyperlipidemic medications or total cholesterol ≥ 240 for dyslipidemia.
Demographic data and general health examination results included age, sex, region of residence, height, weight, waist circumference, smoking history, alcohol intake, physical activity, SBP, DBP, fasting plasma glucose (FPG), and blood lipid profile (including cholesterol, high-density lipoprotein [HDL], low-density lipoprotein [LDL], and triglyceride [TG] levels).28293031 We calculated body mass index (BMI) as weight in kilograms divided by the square of height in meters (kg/m2) and classified the study population into two groups: non-obese (BMI < 25 kg/m2) and obese (BMI ≥ 25 kg/m2) according to the definition of obesity for Asians.32 Metabolic syndrome was defined by the revised National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III) criteria with the combination of 1) central obesity, 2) hypertension or use of anti-hypertensives, 3) elevated TG levels or use of lipid-lowering drugs, 4) elevated FPG or use of diabetes medications, and 5) low HDL-cholesterol levels.3334 The region of residence was classified into two groups: Daegu and Gyeongbuk province, where large-scale outbreaks occurred during the study period, and other regions.25 Alcohol consumption was categorized as non-drinker and drinker (≥ 1 drink a month), and smoking was categorized as non-smoker and ever-smoker. Physical activity was defined as performing either > 30 minutes of moderate physical activity ≥ 5 times a week or > 20 minutes of strenuous physical activity ≥ 5 times per week. Previous medication history within 1 year prior to the test date were obtained and included aspirin, metformin, steroids, and immunosuppressive drugs other than steroids.1235
We identified clinical outcomes of COVID-19 patients using claim codes. The clinical outcomes included ICU admission (AJ code), mechanical ventilator administration (M5850, M5857, M5858, M5859, M5860), conventional oxygen therapy (M0040), high flow nasal cannula (M0046), extracorporeal membrane oxygenation (ECMO) (O1901, O1902, O1903, O1904), and continuous renal replacement therapy (CRRT) (O7031, O7032, O7033, O7034, O7035, O7051, O7052, O7053, O7054, O7055).35 We defined severe clinical outcome of COVID-19 as a composite of death, ICU admission, and mechanical ventilator administration. Death was identified by the classification code of treatment result. Use of inotropes and vasopressors, antiviral agents, and hydroxychloroquine after COVID-19 diagnosis were also evaluated. Drug codes (Anatomical Therapeutic Chemical [ATC] classification system) and diagnostic codes (ICD-10 code) used in this study are summarized in Supplementary Tables 1 and 2.
Statistical analysis
Descriptive statistics are shown as means and standard deviations for continuous variables, and numbers and proportions for categorical variables. Baseline characteristics were compared using the t-test and χ2 test. To evaluate the effect of H2RA and PPI use on the risk of COVID-19, 1:1 nearest neighbor propensity score matching method was applied.36 We selected variables that could potentially affect the study outcomes, including demographic characteristics, height, weight, BMI, waist circumference, systolic and diastolic blood pressure, FBG, lipid profiles, smoking history, alcohol intake, physical activity, comorbidities, CCI, and previous medications.2829303137 We evaluated the adequacy of matching between the user and non-user groups using standardized mean difference (SMD), and a value of < 0.1 was considered to indicate no major imbalance.38 To analyze the association between the use of H2RA or PPI and the study outcome, multivariate logistic regression analyses were performed using three models: 1) Model 1, unadjusted; 2) Model 2, adjusted for age, sex, region of residence, medication history, and comorbidities; and 3) Model 3, adjusted for age, sex, region of residence, medication history, comorbidities, smoking history, alcohol intake, physical activity, obesity, and metabolic syndrome. Statistical significance was defined as a P value of < 0.05. Statistical analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC, USA).
RESULTS
Study population and baseline characteristics
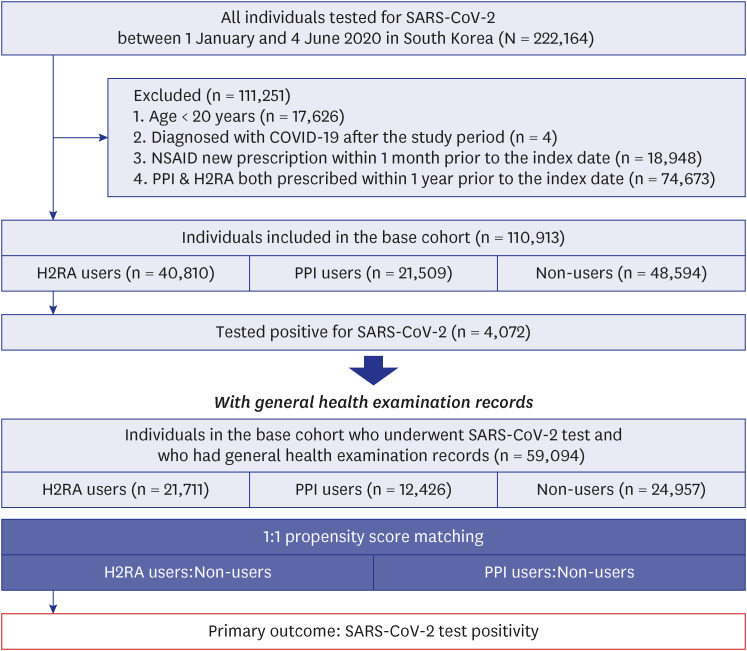
A total of 222,164 patients underwent testing for SARS-CoV-2 in South Korea between 1 January and 4 June 2020. Of these patients, 111,251 patients were excluded, including patients younger than 20 years old (n = 17,626), patients diagnosed with COVID-19 after the study period (n = 4), patients prescribed NSAIDs within 1 month prior to the index date (n = 18,948), and patients prescribed both H2RA and PPI within 1 year prior to the index date (n = 74,678). This left 110,913 patients in the base cohort, of which 40,810 were H2RA users, 21,509 were PPI users, and 48,594 were non-users (Fig. 1). Among the patients in the base cohort, 59,094 patients had general health examination records, including 21,711 H2RA users, 12,425 PPI users, and 24,957 non-users (Fig. 1).
Fig. 1
Flowchart of population selection.
SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2, COVID-19 = coronavirus disease 2019, NSAID = non-steroidal anti-inflammatory drug, H2RA = histamine 2 receptor antagonist, PPI = proton pump inhibitor.
The most common type of H2RA prescribed was ranitidine (50.27%), followed by famotidine (40.14%), cimetidine (34.85%), and nizatidine (10.35%). The most common type of PPI prescribed was esomeprazole (51.10%), followed by rabeprazole (31.44%), pantoprazole (17.98%), lansoprazole (16.73%), dexlansoprazole (7.87%), omeprazole (6.40%), and ilaprazole (4.28%).
Baseline characteristics of H2RA users, PPI users, and non-users who underwent testing for SARS-CoV-2 are shown in Table 1. Compared to non-users, H2RA users and PPI users were more likely to be older, have more comorbidities with higher CCI, take more medications (metformin, aspirin, steroids, and other immunosuppressants), and have larger waist circumference, higher blood pressure, higher FBG level, and lower HDL level. They also tended to smoke less, drink less alcohol, and have metabolic syndrome.
Table 1
Baseline characteristics of individuals tested for SARS-CoV-2
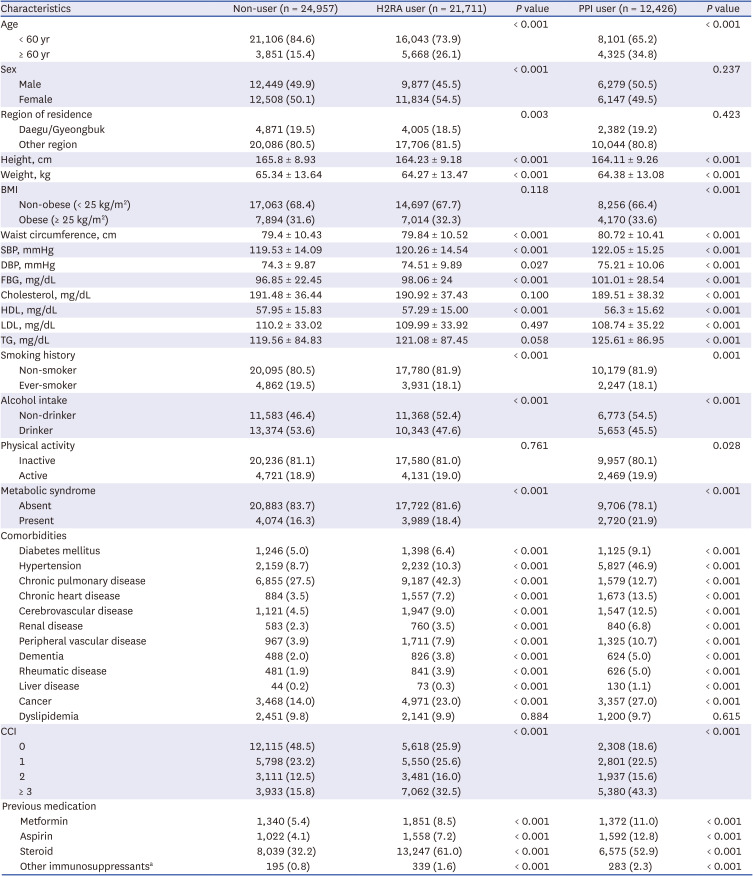
Values are presented as numbers (%) or mean ± standard deviation.
SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2, H2RA = histamine-2 receptor antagonist, PPI = proton pump inhibitor, BMI = body mass index, SBP = systolic blood pressure, DBP = diastolic blood pressure, FBG = fasting blood glucose, HDL = high-density lipoprotein, LDL = low-density lipoprotein, TG = triglyceride, CCI = Charlson Comorbidity Index.
aOther immunosuppressants: Immunosuppressants other than steroids.
SARS-CoV-2 test positivity in H2RA and PPI users
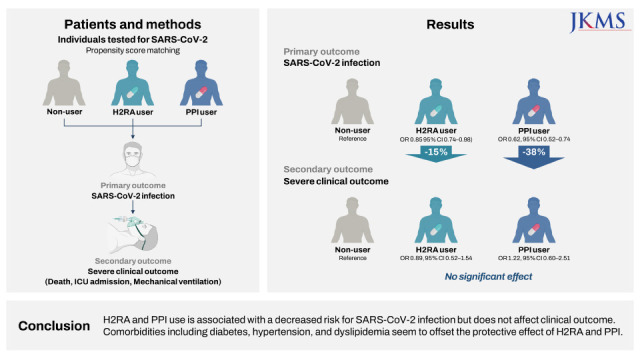
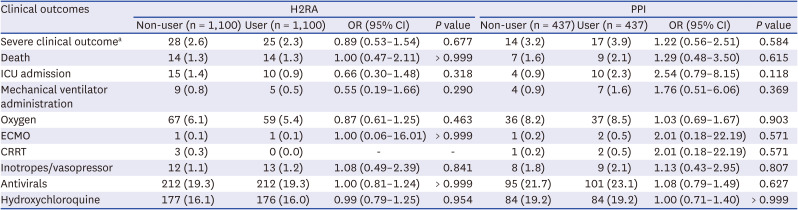
H2RA users (n = 32,287) and PPI users (n = 17,560) were matched individually to an equal number of non-users in each propensity score-matched cohort (Table 2). No major imbalance was noticed in the demographic and clinical characteristics between the user and non-user groups (SMD < 0.1 for all covariates) for either H2RA or PPI. The odds ratio (OR) of testing positive for SARS-CoV-2 associated with H2RA or PPI use is shown in Table 3. In H2RA users, SARS-CoV-2 test positivity was 2.59%, which was significantly lower than SARS-CoV-2 test positivity in the matched non-users (3.11%), with an adjusted OR (aOR) of 0.85 (95% confidence interval [CI], 0.74–98). In PPI users, SARS-CoV-2 test positivity was 2.28%, which was significantly lower than SARS-CoV-2 test positivity in the matched non-users (3.44%), with an aOR of 0.62 (95% CI, 0.52–0.74) (Table 3).
Table 2
Propensity score-matched baseline characteristics and SARS-CoV-2 test positivity in H2RA users, PPI users, and non-users
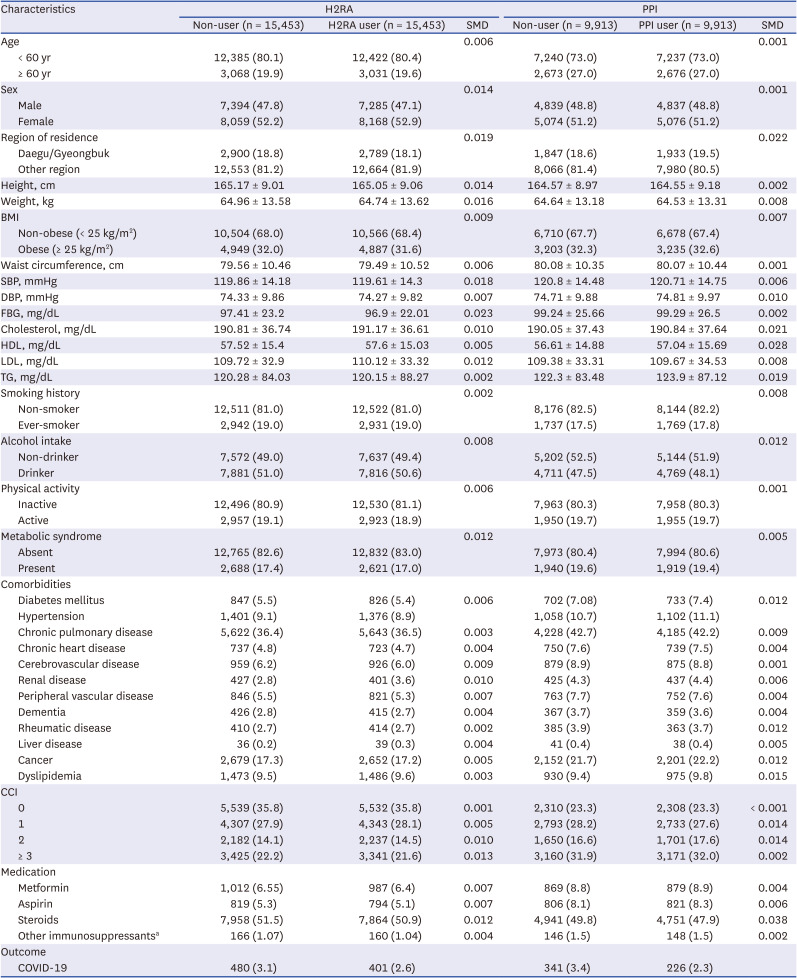
Values are presented as numbers (%) or mean ± standard deviation. An SMD < 0.1 indicates no major imbalance.
SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2, H2RA = histamine-2 receptor antagonist, PPI = proton pump inhibitorm SMD = standardized mean difference, BMI = body mass index, SBP = systolic blood pressure, DBP = diastolic blood pressure, FBG = fasting blood glucose, HDL = high-density lipoprotein, LDL = low-density lipoprotein, TG = triglyceride, CCI = Charlson Comorbidity Index.
aOther immunosuppressants: Immunosuppressants other than steroids.
Table 3
Propensity score-matched association of H2RA and PPI use with SARS-CoV-19 test positivity
H2RA = histamine-2 receptor antagonist, PPI = proton pump inhibitor, SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2, OR = odds ratio, CI = confidence interval, BMI = body mass index.
aNon-adjusted.
bAdjusted for sex, age, region of residence, medication, and comorbidities (chronic pulmonary disease, congestive heart failure, myocardial infarction, peripheral vascular disease, cerebrovascular disease, dementia, rheu matic disease, peptic ulcer disease, liver disease, diabetes mellitus, hypertension, renal disease, and cancer).
cAdjusted for sex, age, region of residence, medication, comorbidities (chronic pulmonary disease, congestive heart failure, myocardial infarction, peripheral vascular disease, cerebrovascular disease, dementia, rheumatic disease, peptic ulcer disease, liver disease, diabetes mellitus, hypertension, renal disease, cancer, and dyslipidemia), metabolic syndrome, smoking history, alcohol intake, physical activity, and BMI.
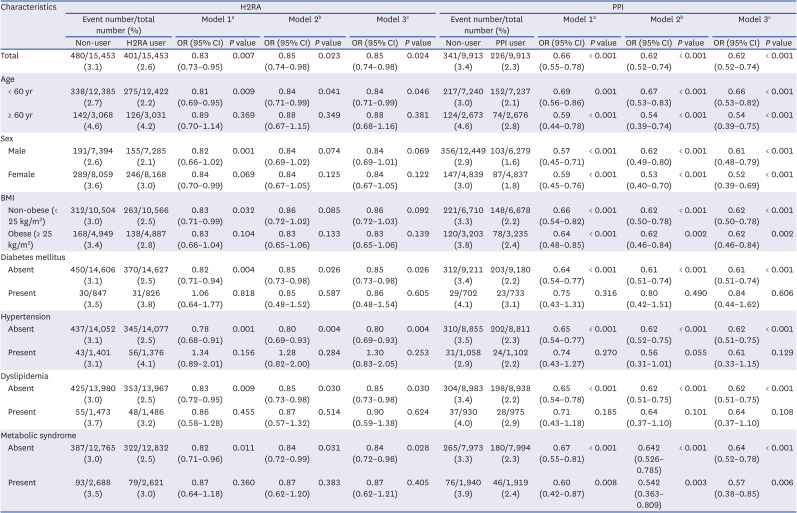
In subgroup analysis, risk of SARS-CoV-2 infection in H2RA or PPI users was significantly lower in patients without comorbidities such as diabetes mellitus (H2RA: OR, 0.85; 95% CI, 0.73–0.98 and PPI: OR, 0.61; 95% CI, 0.51–0.74), hypertension (H2RA: OR, 0.80; 95% CI, 0.69–0.93 and PPI: OR, 0.62; 95% CI, 0.51–0.75), or dyslipidemia (H2RA: OR, 0.85; 95% CI, 0.73–0.98 and PPI: OR, 0.62; 95% CI, 0.51–0.75) in the propensity score-matched cohort. However, the protective effects of H2RA and PPI were not significant in individuals with such comorbidities (Table 3, Figs. 2 and 3). In addition, SARS-CoV-2 test positivity in H2RA users was significantly lower compared to non-users in individuals aged < 60 years and individuals without metabolic syndrome, while H2RA users aged ≥ 60 years and H2RA users with metabolic syndrome did not show such an association.
Fig. 2
Propensity score-matched association of H2RA use with SARS-COV-2 test positivity.
H2RA = histamine 2 receptor antagonist, SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2, BMI = body mass index, aOR = adjusted odds ratio, CI = confidence interval.
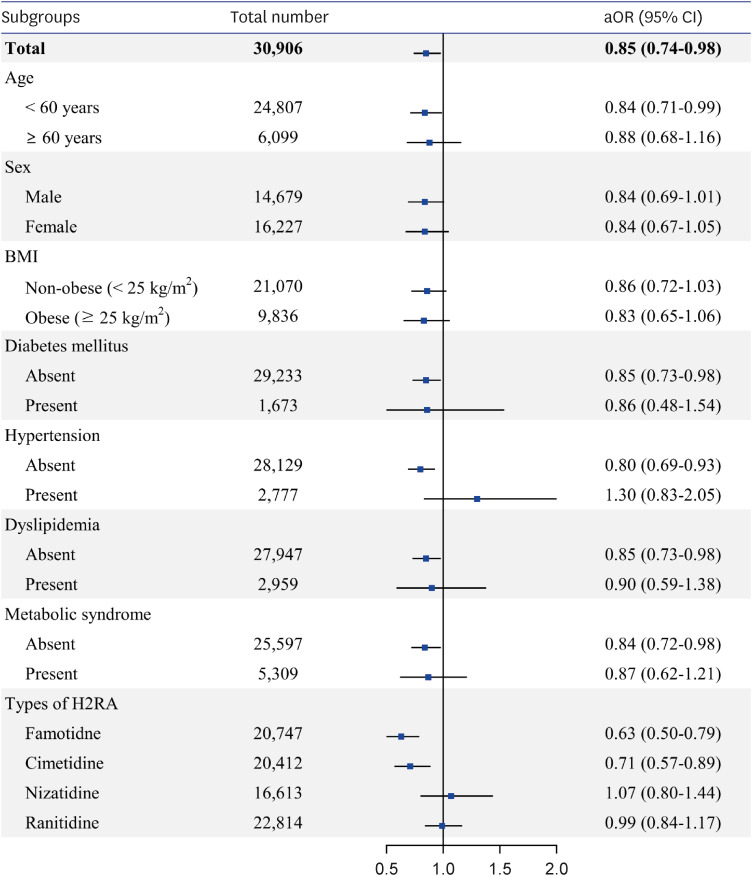
Fig. 3
Propensity score-matched association of PPI use with SARS-COV-2 test positivity.
PPI = proton pump inhibitor, SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2, BMI = body mass index, aOR = adjusted odds ratio, CI = confidence interval.
Subgroup analysis by type of H2RA or PPI used is shown in Figs. 2, 3, and Supplementary Table 3. Among the 4 types of H2RAs evaluated, famotidine (aOR, 0.63; 95% CI, 0.50–79) and cimetidine (aOR, 0.71; 95% CI, 0.57–0.89) use were each associated with significantly lower SARS-CoV-2 test positivity compared to non-users. Among the 7 types of PPIs evaluated, use of dexlansoprazole (aOR, 0.34; 95% CI, 0.16–0.74), esomeprazole (aOR, 0.55; 95% CI, 0.43–0.69), ilaprazole (aOR, 0.14; 95% CI, 0.02–0.99), lansoprazole (aOR, 0.50; 95% CI, 0.33–0.75), pantoprazole (aOR, 0.44; 95% CI, 0.29–0.68), and rabeprazole (aOR, 0.64; 95% CI, 0.50–0.83) were each associated with significantly lower SARS-CoV-2 test positivity. Nizatidine, ranitidine, and omeprazole use were not significantly associated with risk of SARS-CoV-2 infection.
The baseline characteristics, propensity score-matched characteristics, and SARS-CoV-2 test positivity of the base cohort, which includes individuals with and without health examination records, are described in Supplementary Tables 4 and 5. The OR for SARS-CoV-2 test positivity was 0.87 (95% CI, 0.80–0.95) and 0.65 (95% CI, 0.57–0.73) for H2RA users and PPI users compared to non-users, respectively.
Clinical outcomes of patients diagnosed with COVID-19
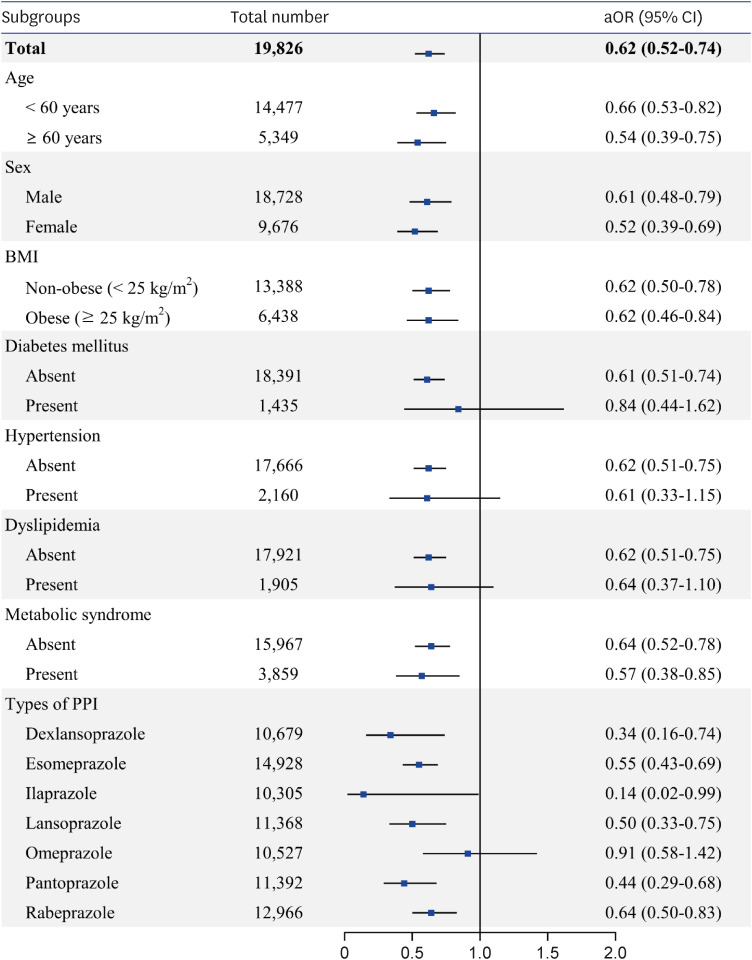
In the base cohort, the overall SARS-CoV-2 positivity rate was 3.67% (4,072/110,913). Among 4,072 patients diagnosed with COVID-19, 1,416 were H2RA users, 479 were PPI users, and 2,177 were non-users (Supplementary Fig. 1, Supplementary Table 6). After propensity score matching, 1,100 H2RA users and 437 PPI users were matched individually to an equal number of non-users. No major imbalance was noticed between the user and non-user groups (SMD < 0.1 for all covariates) for either H2RA or PPI (Supplementary Tables 7 and 8). Propensity score-matched association of H2RA and PPI use with clinical outcomes of COVID-19 are shown in Table 4. After propensity score matching, risk of death, ICU admission, mechanical ventilator administration, and severe clinical outcome, a composite of the previous three outcomes, did not show significant association with the use of H2RA or PPI. Other outcomes such as oxygen demand and use of ECMO, CRRT, inotropes, vasopressors, antiviral agents, and hydroxychloroquine were not significantly associated with H2RA or PPI use either.
Table 4
Propensity score-Matched association of H2RA or PPI use with clinical outcomes of COVID-19 patients
Values are presented as numbers (%).
H2RA = histamine-2 receptor antagonist, PPI = proton pump inhibitor, COVID-19 = coronavirus disease 2019, OR = odds ratio, CI = confidence interval, ICU = intensive care unit, ECMO = extracorporeal membrane oxygenation, CRRT = continuous renal replacement therapy.
aSevere clinical outcome: composite of death, ICU admission, and mechanical ventilator administration.
DISCUSSION
In this nationwide population-based cohort study, use of either H2RA or PPI was associated with decreased risk of SARS-CoV-2 infection and was not associated with severe COVID-19 outcomes. However, the protective effect of acid suppression against SARS-CoV-2 infection seems to be null in the presence of comorbidities including diabetes, hypertension, and dyslipidemia.
The incidence of COVID-19 infection in this study was 3.67% which was similar to other population-based studies (3.61–6.4%).1112 Previous studies that evaluate the association of H2RA and PPI with the susceptibility to SARS-CoV-2 and clinical outcome of COVID-19 show inconsistent results. These studies vary widely in the study population, type of study, definition of antacids use, covariate adjustments, and study period. Supplementary Table 9 shows difference in methods and results of previous studies regarding the association of acid suppressants and risk of SARS-CoV-2 infection and clinical outcome of COVID-19 and this study.
Almario et al.11 conducted an online survey of 53,130 participants and report that people who use PPI have increased risk of SARS-CoV-2 infection, while people who use H2RA have decreased risk SARS-CoV-2 infection. Fan et al.13 used the UK Biobank data of 9,469 participants and report that neither H2RA nor PPI is associated with SARS-CoV-2 infection. However, both studies are based on self-reported data of drug intake, either online surveys or verbal interviews. In addition, the use of H2RA and PPI is defined as current use at the time of the survey, which includes past H2RA and PPI users in the reference group and makes assessing the effect of past H2RA and PPI use difficult. Most other studies evaluate the association of either H2RA or PPI use, not both, with the risk of SARS-CoV-2 infection and report inconsistent results.121416 Lee et al.12 conducted a nationwide cohort study in South Korea using NHIS data, which is similar to our study. They report that PPI use is not associated with positive SARS-CoV-2 test results but is related to increased risk of severe clinical outcomes of COVID-19.12 The main differences between the two studies are that our study evaluated both H2RA and PPI, included general health examination results for covariate adjustment such as BMI and presence of metabolic syndrome, smoking history, alcohol intake, physical activity, and laboratory findings, and excluded more types of recently used NSAIDs. Considering previous studies that reported obesity and metabolic disease as risk factors for SARS-CoV-2 infection,3940 adjusting such covariates may have contributed to the different results of the two studies.
In terms of the clinical outcomes of COVID-19 patients, several multicenter retrospective cohort studies have reported similar results to our study.7131921 In contrast, Freedberg et al.18 reports that H2RA use is associated with reduced risk of severe clinical outcomes of COVID-19 and PPI use is associated with increased risk, while Zhou et al.22 reports that both H2RA and PPI are associated with an increased risk. Interestingly, a recent meta-analysis suggests that the association of PPI and increased risk of pneumonia might have been overestimated due to protopathic bias and reverse causality.26 Although several studies have reported the association of acid suppressant use and increased risk of COVID-19, when the studies that adjusted for NSAID use, BMI, and smoking history were analyzed separately, the significant association disappeared.15 Notably, the majority of previous studies that reported elevated risk of COVID-19 outcomes were those that did not include BMI for covariate adjustment.12414243444546 Previous studies suggest that acid suppressants may be associated with immune system impairment, resulting in increased susceptibility to infections such as pneumonia.26 However, in our study, both H2RA and PPI were associated with reduced risk of SARS-CoV-2 infection. Recently, a study using computational methods reported that famotidine likely inhibits the 3-chymotrypsin-like protease, which acts on proteins essential for virus replication.8 The protective effect of famotidine on SARS-CoV-2 infection can be explained by on-target histamine receptor-H2 activity, receptor mediated immunomodulatory effects on mast cell activation, and histamine–cytokine cross talk.47 which may also explain the effect of other H2RAs. PPIs have shown antiviral effects in various in vitro and in vivo studies.48 Possible mechanisms of PPI against SARS-CoV-2 include exerting anti-fibrotic and anti-inflammatory effects, targeting endosomal complexes, and raising endolysosomal pH via vacuolar ATPase pumps.48 However, caution is warranted in interpreting in vitro experimental results, as many drugs that were reported to be effective in vitro, such as hydroxychloroquine, did not show such effect in clinical studies.4950
In subgroup analysis, the protective effect of H2RA and PPI against SARS-CoV-2 infection was not significant in patients with diabetes mellitus, hypertension, or dyslipidemia. This may be due to the many direct links between COVID-19 and the metabolic system. Patients with metabolic syndrome and its components are highly susceptible to SARS-CoV-2 infection51 and are at increased risk of developing severe COVID-19.52 Metabolic dysfunction leads to a state of chronic inflammation, and in metabolic syndrome patients, inflammatory cytokines such as tumor necrosis factor-α, interleukin (IL)-1β, and IL-6 are upregulated in the adipose tissue.52 The chronic systemic inflammation and dysregulated immunometabolism provoked by metabolic associated preconditions may intensify inflammation associated with SARS-CoV-2 infection.34 In addition, expression of ACE2, the entry receptor of SARS-CoV-2, is increased following inflammatory stress and metabolic syndrome.51 Enhanced expression of ACE2, combined with endothelial dysfunction and dysregulation of adipocytokines in metabolic syndrome and associated preconditions, may play a crucial role in the susceptibility to SARS-CoV-2 infection and development of COVID-19.51 In subgroup analysis, individuals with obesity, diabetes mellitus, hypertension, metabolic syndrome, as well as old age and female sex showed higher SARS-CoV-2 test positivity rates both in non-users and acid suppressant users, compared to individuals without comorbidities, young age, and male sex (Supplementary Table 3). Considering the possible effect of H2RA and PPI on immunomodulation and anti-inflammation, the comorbidity of diabetes mellitus, hypertension, or dyslipidemia may have offset the protective effect of acid suppressants against SARS-CoV-2 infection.
With respect to the types of drugs used, notable exceptions were found with omeprazole, nizatidine, and ranitidine, which did not show a significant association with risk of SARS-CoV-2 infection. One previous study that evaluated the effect of acid suppressants on the risk of COVID-19 shows a similar trend, reporting that omeprazole users are more likely to have positive SARS-CoV-2 test results compared to users of other PPI.13 Another study identifying the effect of famotidine on cytokine storm reported that while famotidine activates the vagal inflammatory reflex to attenuate cytokine storm, ranitidine did not show such effect even at high doses.53 However, the mechanism behind these tendency is yet to be discovered.
Individuals who were prescribed NSAIDs within 1 month the index date were excluded in the consideration that acid suppressants may have been initiated with NSAIDs in COVID-19 patients with early pneumonia symptoms who are not yet diagnosed.1226 The period of 1 month seems reasonable since previous studies reported the time from symptom onset to diagnosis to be as long as 4 weeks.5455
This study has several limitations. First, the study was based on NHIS claims data, which may not accurately reflect patients’ drug intake. Although the patients’ exposure to H2RA and PPI is highly accurate because a prescription is required to obtain H2RA and PPI in South Korea, drug compliance could not be screened by this study. Second, as with all retrospective studies, the possibility of unmeasured confounders cannot be excluded. Although we have adjusted most of the confounders, including demographic characteristics, various underlying diseases, medication history, and general health examination data, other variables that may affect outcomes, such as socioeconomic status or education level, were not included. Third, underlying disease and general health examination data were assessed from past ICD codes and health check-up data, which may not reflect the individuals’ exact status on the index date. Fourth, the period of one year could be insufficient to explain the biologic plausibility of the drugs. Also, this study did not differentiate between current and past user group. However, a previous study reported that majority of patients who are prescribed with acid suppressants have a tendency to take the drugs in intermittent or on-demand basis in a long-term period.56 This suggests that patients who are prescribed acid suppressants months before diagnosis could still take medications long after the date of prescription, which could contribute to biological plausibility. This tendency can make it difficult to differentiate current users from past users when using claims data, since patients who are prescribed acid suppressants long ago but take the drug on demand or intermittently until test date could be defined as past users by study definition, but actually be current users.56 Also, a previous study that compared the time window of PPI prescription and diagnosis of COVID-19 reported a decreasing, but still significant tendency in the protective effect of PPI on COVID-19 infection as the window period changed from 6 months, 1 year, to 2 years.57 We believe this results could indicate the possibility of the biologic effect of acid suppressants in a long term period although the mechanism should be further identified. Lastly, cumulative exposure and dose dependent risk could not be evaluated. In the future, prospective, well-matched, long-term studies are warranted to overcome these limitations.
The strengths of this study include a large sample size from a well-characterized national cohort that included the whole population that underwent testing for SARS-CoV-2. Vigorous adjustment for potential confounders, which included not only demographics, comorbidities, and medications but also anthropometry and laboratory data, was performed. We also applied strict exclusion criteria for individuals who received new prescriptions of NSAIDs or prescriptions of both H2RA and PPI within 1 year prior to the index date, to minimize bias. We believe the results of this study could provide additional knowledge to the effect of acid suppressant in the process of infection of SARS-CoV-2, especially in relation with metabolic preconditions.
In this large-scale propensity-matched nationwide study, H2RA and PPI use was associated with a lower risk of SARS-CoV-2 infection but did not show significant association with clinical outcomes of COVID-19 patients. Comorbidities including diabetes, hypertension, and dyslipidemia seem to offset the protective effect of the medications. Our results provide improved insight into the association between acid suppressants and risk of COVID-19.
 XML Download
XML Download