

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Polycystic ovary syndrome (PCOS) is the most common endocrine disorder among women of reproductive age and is characterized by typical features including clinical or biochemical hyperandrogenism, irregular menstrual cycles, and polycystic ovarian morphology, according to the Rotterdam 2003 consensus.12 The prevalence of PCOS was 8–13% among women of reproductive age, depending on the population studied and definitions used.3 A recent population-based study indicated that the annual incidence of PCOS has increased steadily among Korean women in recent years.4 Women with PCOS have a greater risk of several cardiometabolic disorders including obesity, insulin resistance, type 2 diabetes mellitus (DM), dyslipidemia, hypertension, metabolic syndrome, and cardiovascular diseases.5 Mothers with PCOS are also at increased risk of gestational diabetes, endothelial dysfunction, and pre-eclampsia, which can affect both the fetal endocrine environment and long-term health of their offspring.67 There is growing evidence that daughters of mothers with PCOS may be at a higher risk for various reproductive and metabolic disorders, in addition to being diagnosed with PCOS.89101112
However, it is still controversial whether maternal PCOS is independently associated with childhood growth and obesity of the offspring.13 Early childhood obesity is significantly indicative of future cardiometabolic health, such as insulin resistant hyperinsulinism.14 Furthermore, longitudinal population-based studies demonstrated that higher body mass index (BMI) and early timing of adiposity rebound in childhood were associated with PCOS diagnosis in later life.15 Few studies have investigated the association between maternal PCOS and offspring growth and obesity, and their results have been conflicting. A Danish prospective cohort study showed that both maternal PCOS and high maternal BMI are associated with an increased risk of childhood obesity in offspring, at 3 years of age, and faster catch-up growth.16 However, other recent population-based cohort studies reported contrasting results, finding no significant association between maternal PCOS and early childhood BMI in offspring through 3–4 years of age.1718 These studies were mostly conducted in Western populations, and it is unclear whether the offspring of East Asian women with PCOS, characterized by a lower incidence of obesity compared to Western women with PCOS,3 have an increased risk of obesity in early childhood.
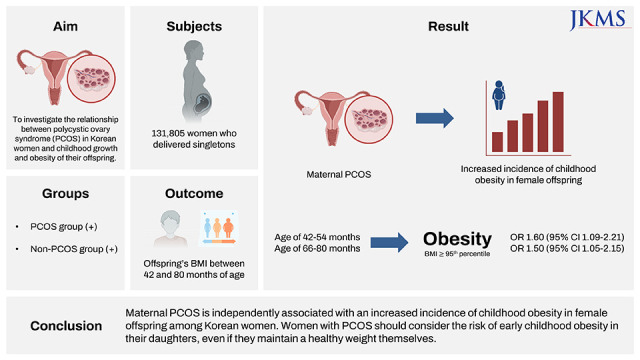
Thus, this study aimed to evaluate the association between maternal PCOS and childhood obesity in offspring among Korean women using nationwide population-based data.
METHODS
Data source
In Korea, 97% of the population is enrolled in the Korea National Health Insurance (KNHI) program. All claims information for these individuals are encoded in the KNHI claims database. The study data were collected from the KNHI claims database for 2007–2008. Additionally, data from the National Health Screening Examination (NHSE) provided by the KNHI and the National Health Screening Program for Infants and Children (NHSP-IC) were used to assess pre-pregnancy characteristics and offspring growth. The NHSE consists of 2 components: a health interview and health examination. The NHSP-IC was started in 2007 and comprised seven consecutive health examinations based on age groups: 4 to 9 months, 9 to 18 months, 18 to 30 months, 30 to 42 months, 42 to 54 months, 54 to 66 months, and 66 to 80 months. Data from this program, including physical examination, anthropometric examination, and developmental screening, were also contained within the program database.
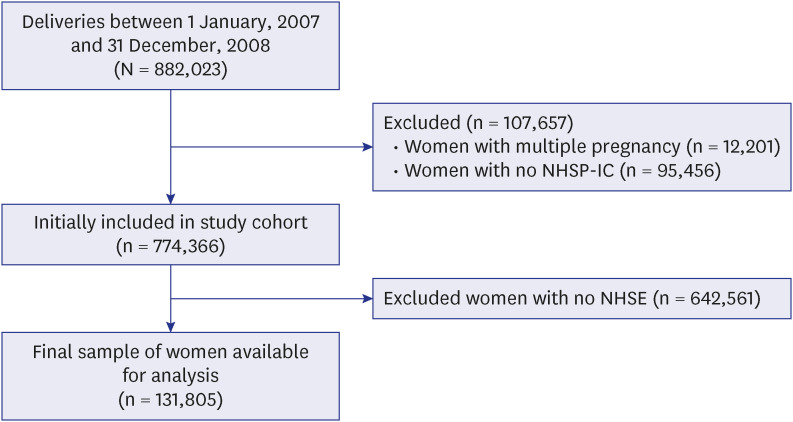
In this study, using the KNHI claims database, we identified all women who delivered singletons between January 1, 2007, and December 31, 2008, and whether they had PCOS before pregnancy based on the International Classification of Diseases-10th Revision (ICD-10 codes). To evaluate the pre-pregnancy characteristics, only women who underwent NHSE within 1 year prior to pregnancy were included. Women were excluded from the analysis if their offspring had not undergone at least one of the seven consecutive NHSP-IC health examinations. The data of women who met the inclusion criteria were linked to the data of their offspring available in the NHSP-IC database. Fig. 1 shows a flowchart of the study participants’ enrollment.
Outcomes and variables
Offspring growth was assessed using BMI measurements that had been taken between 30 and 80 months of age. For this analysis, we used the results from the 5th, 6th, and 7th NHSP-IC screening examinations because the data on BMI measurements were available for those periods in the NHSP-IC database. Current BMI was categorized according to age- and sex-specific BMI, which was derived from the NHSP-IC. Childhood obesity was defined as a BMI ≥ 95th percentile.
Data on maternal and offspring outcomes were analyzed: pregnancy outcomes such as maternal pre-pregnancy hypertension, pre-pregnancy diabetes, and delivery mode using the KNHI claims database, and neonatal outcomes such as neonatal sex, gestational age at birth, and birth weight. Preterm birth was defined as gestational age < 37 weeks.
Pre-pregnancy characteristics were evaluated using the NHSE data. The NHSE consists of 2 components: a health interview and health examination. Using the health interview, data for the smoking status was obtained. Health examination included the BMI (in kilograms per square meter). The participants were categorized into four groups based on their BMI as per the cutoff points for Asia-Pacific populations: underweight (< 18.5 kg/m2), normal weight (18.5–22.9 kg/m2), overweight (23–24.9 kg/m2), and obese (≥ 25 kg/m2). For statistical analyses in this study, data from participants in the overweight category were combined with those from participants in the normal weight category. Blood pressure (BP) was measured using a standard mercury sphygmomanometer. All blood samples were obtained after a minimum fast of 8 hours. The levels of aspartate aminotransferase (AST), alanine transaminase (ALT), and total cholesterol were measured by using enzymatic methods. Elevated liver enzymes and high cholesterol were defined as AST or ALT ≥ 31 IU/L and ≥ 200 mg/dL, respectively.19
Statistical analysis
Continuous and categorical variables were expressed as mean ± standard deviation and percentages, respectively. Clinical characteristics were compared using the t-test for continuous variables and the chi-square test for categorical variables. Multivariable logistic regression analysis was used to estimate the adjusted odds ratio (OR) and 95% confidence intervals (CIs) for the association of a history of PCOS with obesity in offspring at each follow-up period of NHSP-IC, using data from the 5th, 6th, and 7th screening examination results. Generalized estimating equations (GEE) were used to evaluate the association between maternal history of PCOS and childhood obesity in the offspring longitudinally, taking into account the correlation between repeated measurements in the same individual. All tests were two-sided, and statistical significance was set at P < 0.05. Statistical analyses were performed using SAS for Windows (version 9.4; SAS Inc., Cary, NC, USA).
RESULTS
Among a total of 131,805 women, 1,213 women had a history of PCOS and 130,592 women did not; in addition, their BMI values were 21.3 ± 3.0 and 20.8 ± 2.6, respectively (P < 0.001). Table 1 shows a comparison of the baseline characteristics between the two groups. In addition to higher BMI, women with PCOS had a higher prevalence of type 2 DM and gestational diabetes mellitus (GDM) and higher serum levels of AST, ALT, and total cholesterol (Table 1). The BMI of the participants’ offspring until 80 months of age stratified by maternal history of PCOS is presented in Table 2. Until 66 months of age, the BMI of offspring was not significantly different according to maternal history of PCOS in both sexes. However, the BMI of female offspring aged 66 to 80 months was significantly higher in those born to women with PCOS than those born to women without PCOS; on the other hand, the BMI of male offspring aged 66 to 80 months did not differ regardless of maternal history of PCOS (Table 2).
Table 1
Basic participant characteristics stratified by maternal history of PCOS
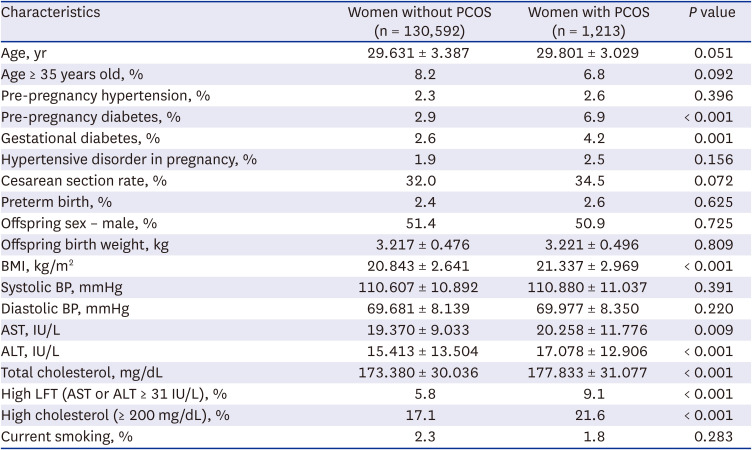
Table 2
BMI of offspring until 80 months of age stratified by maternal history of PCOS
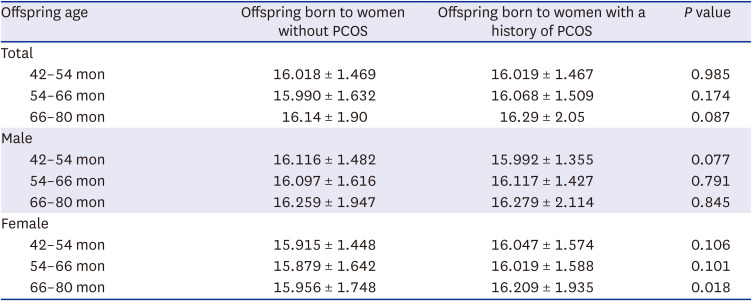
Table 3 shows the results of the GEE and multivariable logistic regression analyses for the risk of obesity in male and female offspring until 80 months of age according to the maternal history of PCOS. Maternal PCOS was significantly associated with higher odds of being obese in female offspring during the age of 42–54 and 66–80 months after adjusting for maternal age, pre-pregnancy hypertension, pre-pregnancy DM, GDM, gestational hypertension, smoking, BMI, blood pressure, high AST, high ALT, high cholesterol, birth weight of offspring, and preterm birth. The odds of obesity in male offspring were not significant according to maternal PCOS until 80 months of age (Table 3). According to the results of subgroup analyses divided by maternal BMI, among the group of normal-weight women, the female offspring born to women with PCOS had significantly higher odds of being obese during the age of 42–54 and 66–80 months (OR, 1.9; 95% CI, 1.32–2.83 and OR, 1.9; 95% CI, 1.26–2.72, respectively), compared to the female offspring born to women without PCOS, after adjusting for the same variables included in the multivariable analysis presented in Tables 3 and 4. However, the odds of obesity in both male and female offspring were not significant according to maternal PCOS until 80 months of age among the underweight women and the obese women (data not shown).
Table 3
Prevalence of offspring obesity and the results of logistic regression analyses for the association between the maternal history of PCOS and offspring obesity until 80 months of age, stratified by offspring sex and age
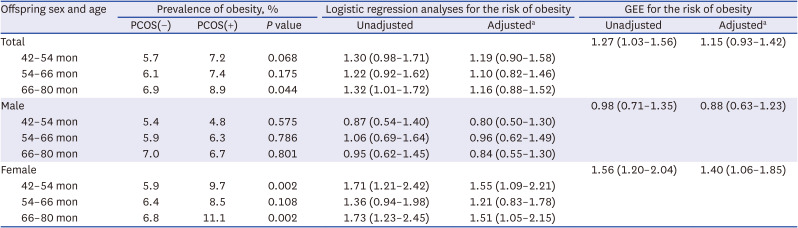
PCOS = polycystic ovary syndrome, GEE = generalized estimating equation
aAdjusted for maternal age, body mass index, blood pressure, high liver function test, high total cholesterol, current smoking, pre-pregnancy hypertension, pre-pregnancy diabetes, gestational diabetes, hypertensive disorders in pregnancy, preterm birth, and birth weight.
Table 4
Prevalence of offspring obesity and the results of logistic regression analyses for the association between maternal history of PCOS and offspring obesity until 80 months of age, stratified by offspring sex and age, among the normal-weight women
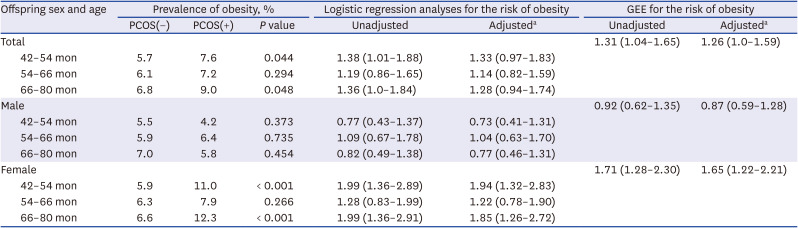
PCOS = polycystic ovary syndrome, GEE = generalized estimating equation.
aAdjusted for maternal age, body mass index, blood pressure, high liver function test, high total cholesterol, current smoking, pre-pregnancy hypertension, pre-pregnancy diabetes, gestational diabetes, hypertensive disorders in pregnancy, preterm birth, and birth weight.
DISCUSSION
This large population-based study showed that female offspring born to a mother with a history of PCOS have an increased risk of obesity until 80 months of age after adjusting for several important confounding factors, including maternal BMI, history of diabetes, preterm birth, and birth weight. To the best of our knowledge, this is the first study to reveal this association among Korean women whose metabolic and PCOS-related phenotypes are different from those of the Western population. Recent international guidelines for the management of PCOS recommend that all women with PCOS should be offered regular monitoring for weight changes and excess weight,3 regarding the association of obesity with cardiovascular risks and a more prominent manifestation of PCOS.20 Although there are no recommendations or comments regarding the childhood obesity and metabolic health of the offspring in the guidelines, our findings suggest that women with PCOS should consider not only their metabolic health, but probable early childhood obesity of their female offspring as well, even if they maintain healthy weight.
The Upstate KIDS study is a population-based prospective cohort study from the United States that included 4,949 children (1,745 twins) born to 4098 mothers (435 self-reported PCOS) and reported that children of mothers with PCOS did not have significant differences in weight, length/height, and BMI over 3 years of age, compared with children born to mothers without PCOS.21 However, they did not investigate the association between maternal PCOS and offspring BMI stratified by maternal obesity. Approximately 70% of PCOS mothers were overweight/obese (BMI ≥ 25 kg/m2) in the Upstate KIDS study, whereas only 28% of PCOS mothers were overweight/obese (BMI ≥ 23 kg/m2, according to the Asia-Pacific criteria) in our study. While a sex-stratified analysis was not performed in the Upstate KIDS study, the present study found that maternal PCOS was associated only with childhood obesity in female offspring. A recent large-scale nationwide cohort study conducted in Finland reported that maternal PCOS (or anovulatory infertility) was associated with an increased risk of offspring obesity from an early age, irrespective of their sex; the hazard ratio (HR) for obesity was increased in offspring below 9 years of age (HR, 1.58; 95% CI, 1.30–1.81), and in those 10–16 years of age (HR, 1.37; 95% CI, 1.19–1.57), but not in those aged 17–22 years (HR, 1.24; 95% CI, 0.73–2.11).22 These results are partially in line with those of our present study. However, obesity in offspring in that study was defined based on ICD codes instead of measured or self-reported weight and height, which carries a risk of underestimating the incidence of obesity and considerable bias.22
It is supposed that the offspring of mothers with PCOS are exposed to intrauterine excess androgen in fetal life, which would be a potential transcriptional inducer of their impaired metabolic health.23 During its early development, the fetus is highly sensitive to steroid hormone exposure, particularly androgens.24 Intrauterine exposure to androgens can lead to epigenetic changes and subsequent alterations in the genes expressed in the developing fetus,25 although its exact mechanisms are not fully elucidated. High androgen levels observed in the term umbilical vein and increased anogenital distance in newborn daughters of women with PCOS.2627 In gestational testosterone-exposed female nonhuman primates, PCOS-like traits were observed in response to circulating testosterone levels comparable to those found in male fetuses.28 These findings suggest that gestational hyperandrogenism may significantly impact the female offspring of a mother with PCOS rather than the male offspring. A recent prospective population-based study with a long-term follow-up demonstrated that maternal hyperandrogenism during pregnancy is associated with a higher risk of being overweight and developing type 2 diabetes in female offspring during adolescence and adulthood.29 However, there are also conflicting results from several human and animal studies regarding whether intrauterine hyperandrogenism affects offspring growth, and further studies are warranted to confirm it.30 Additionally, an altered gut microbiota and its metabolites have been reported in women with PCOS, which might reflect a maternal–fetal gut microbiota pathway in offspring metabolic health.31 Finally, PCOS is associated with various pregnancy complications that are likely to provide a suboptimal intrauterine environment,32 and there would also be several shared risk factors, such as maternal adiposity. However, in the present study, the association between maternal PCOS and offspring obesity was still significant after controlling for confounding conditions, including mothers’ BMI, pre-pregnancy DM, GDM, gestational hypertension, preterm birth, and offspring birth weight. Therefore, the exact mechanism linking maternal PCOS with offspring metabolic health, including childhood obesity, remains unclear, and further studies are warranted.30
To the best of our knowledge, this is the first large population-based longitudinal study with long-term follow-up, which revealed an independent association between maternal PCOS and early childhood obesity in female offspring, entirely measured by physicians rather than self-questionnaires or diagnostic codes, in an Asian population. However, our study had some limitations. First, the incidence of PCOS might be underestimated in the NHIS database because it was estimated based on physicians’ diagnoses of the disease; in addition, the control group of our study had a potential risk of including asymptomatic women with PCOS who had not visited a gynecological clinic and thus were not diagnosed with PCOS by physicians. Second, this study could not assess the diagnostic details and types of PCOS due to the characteristics of the claims database. Further studies are needed to confirm our findings according to the type of PCOS, particularly whether it includes hyperandrogenism. Third, it is unclear why the prevalence of obesity in female offspring aged 42–54 months and 66–80 months were associated with maternal PCOS, whereas that in female offspring aged 54–66 months was not; a further study with a large sample size would be needed to corroborate these findings. Fourth, although several confounding factors were considered in this study, there could be other factors that could not be controlled in this study, mainly due to the lack of data in the NHIS database, including weight gain during pregnancy, history of treatment with oral contraceptive pills or metformin, and eating habits, which might be shared risk factors for mothers and their offspring. These limitations should be assessed in future cohort studies.
In conclusion, female offspring born to Korean women with PCOS had higher BMI and an increased risk of obesity in their early childhood until the age of 80 months, unlike male offspring. Maternal PCOS showed an independent association with obesity in female offspring, particularly among normal-weight women. Women diagnosed with PCOS should consider both the risk of early childhood obesity and transgenerational susceptibility to PCOS in their daughters, even if they maintain a healthy weight for their own metabolic health.
 XML Download
XML Download