

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Vaccine administration is an essential component of the strategy for controlling the coronavirus disease 2019 (COVID-19) pandemic. Following the surge of delta variant cases,12 medical authorities, such as the World Health Organization (WHO), have encouraged the public to undergo vaccination as soon as possible.3 As of October 5, 2021, seven vaccines were approved by the WHO, and 22 vaccines were approved by at least one country.4 Among them, Pfizer/BioNTech [BNT162b2] was approved in 100 countries, and Moderna [mRNA-1273] in 76 countries, after demonstrating safety and efficacy through large phase 3 trials. Both trials showed that serious adverse effects of these vaccines are rare.56
However, there have been reports of rare or serious adverse effects following large-scale vaccine administration. A review of the risk of rare blood clots associated with the Oxford/AstraZeneca [AZD1222] vaccine was conducted by the European Medicines Agency (EMA), involving 30 cases of thromboembolic events, which had been reported among 5 million vaccinations.78 Furthermore, by April 7, 2021, the EMA acknowledged that the Oxford/AstraZeneca vaccine was associated with unusual blood clots (6.53 cases per 1,000,000 as of April 4, 2021).9 Several countries have limited Oxford/AstraZeneca vaccine administration to younger populations, even though the evidence of vaccine benefits outweighs the risks.10 By the end of March, Canada and Germany suspended the use of the Oxford/AstraZeneca vaccine for those under the age of 55 and 60 years, respectively.11 Italy and Spain restricted the vaccine to those > 60 years following the EMA statement. As for the United Kingdom, the Joint Committee on Vaccination and Immunization recommended alternative vaccines for people aged < 30 years.10 The South Korean Oxford/AstraZeneca vaccine age restriction changed to > 30 years on April 12, 2021.12 Safety of the Johnson & Johnson [Ad26.COV2.S] vaccine, which is the same type of vaccine as Oxford/AstraZeneca, was also investigated. As of April 21, 2021, the reported rates of thrombosis with thrombocytopenia syndrome (TTS) in the United States were 7 cases per 1,000,000 for women aged 18–49 years and 0.9 cases per 1,000,000 for women aged > 50 years. However, the Advisory Committee on Immunization Practices (ACIP) reaffirmed that the Johnson & Johnson vaccine is highly effective, and vaccination continues to be recommended for people aged > 18 years based on the risk-benefit analysis on April 23, 2021.13 Myocarditis has been recognized as a complication of mRNA [mRNA-1273, BNT162b2] vaccinations by the ACIP on June 23, 2021. Myocarditis reporting rates following the second doses of mRNA vaccines were 40.6 cases per 1,000,000 for males aged 12–29 years and 2.4 per 1,000,000 for males aged > 30 years; rates among females in these age groups were 4.2% and 1.0 per 1,000,000, respectively.14 However, vaccine benefits clearly surpass the risk of myocarditis; therefore, mRNA vaccines are recommended for people aged > 12 years in the US.1516
Because of limited experience with new vaccine platforms, vaccine safety discussion is inevitable.2 However, the reasons for vaccine acceptance and hesitancy could be connected to public announcements regarding the rare and fatal side effects of vaccines.17 Therefore, to overcome the pandemic, it is essential to evaluate whether the outcomes of vaccine adverse events influence the worldwide vaccination rate. In this study, regression discontinuity in time (RDiT) analysis was conducted to investigate the impact of adverse events of special interest (AESI) on the vaccination rate.
METHODS
Data
We integrated two datasets: one dataset from our world, which is produced and maintained by the Global Change Data Lab and contains the vaccination counts of all countries, and the other dataset from the Johns Hopkins University Center for Systems Science and Engineering, which contains the COVID-19 confirmed and death cases for each date. By integration, the dataset covered the number of vaccinations (completed), newly confirmed cases, and cases of death in 47 countries, including the US and European countries. Vaccination rates were calculated as the ratio of the number of completed vaccinations to the total population by country and date (Supplementary Table 1).
Statistical analysis
The study employed a series of RDiT analyses to evaluate whether AESI could have decreased the national vaccination rates. RDiT designs have been used in situations where the treatment is assigned based on a specific date in time.1819 Following methodological developments in the regression discontinuity literature,20 this study utilized nonparametric polynomial estimators to estimate average treatment effects. In the original regression discontinuity design, when Xi ∈ {0,1} is assigned to a sample of i ∈ {1,2,3,…n} such that Xi = 1 for Ti > c and Xi = 0 for Ti ≤ c (where Ti is a continuous time variable), the local average treatment effect (LATE) is estimated by linearly regressing the outcome variable Y on T − c, the treatment variable X, and the interaction (T − c) · X at local values close to the cutoff c. However, because we adopted a non-parametric estimation strategy, τ is approximated through weighted polynomials, whose weights are calculated through a uniform kernel function for each observation distance from the cutoff c.
The time variable for the US and the UK was the calendar day, whereas in Europe, the time variable was the calendar week. Since vaccination rates in Europe were not always reported daily, we used the weekly averages of daily vaccinations. For the US, RDiT analysis was conducted using two cutoff points, April 23rd, 2021(the day the US Center for Disease Control’s ACIP convened to vote on the continued administration of the Johnson & Johnson vaccine) and June 23rd, 2021 (the day an ACIP meeting was held regarding mRNA vaccines and myocarditis). For the UK, the cut-off was April 7th, 2021(the day the EMA held a press briefing regarding Oxford/AstraZeneca’s connection to thromboembolic events). For Europe, RDiT analysis was conducted using the fourteenth week of 2021 (the week of April 7, 2021) as the cutoff, excluding countries where the cumulative vaccination rate was still below 5% four weeks later (Table 1, Supplementary Fig. 1). The main models used 60-day bandwidths for the US and UK and 10-week bandwidths for Europe. All models were computed by applying uniform kernel functions. All estimations were made using the rdrobust command in the Stata software (version 15.0; StataCorp, College Station, TX, USA) (Supplementary Methods 1).
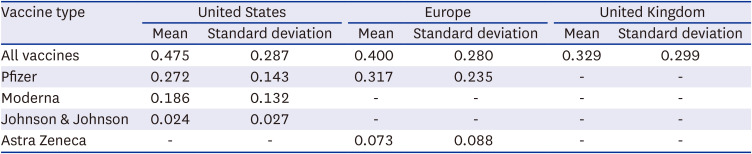
Table 1
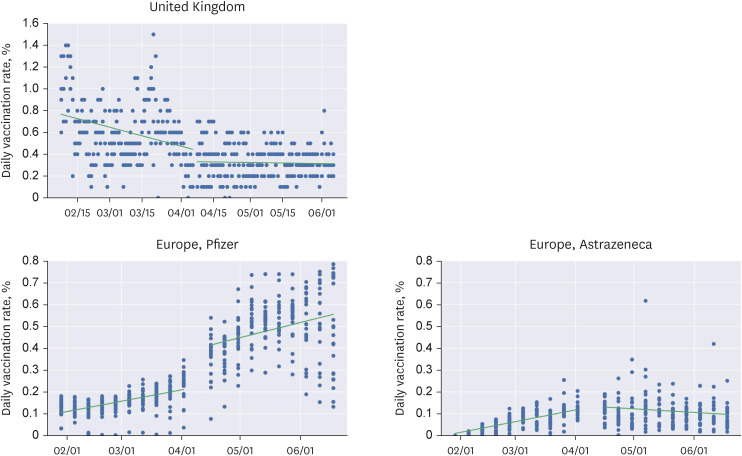
Daily vaccination rates per vaccine type
In the sensitivity analysis, we introduced additional features to the main models to address the potential sources of bias. First, we used a variety of other bandwidths, including mean squared error (MSE) optimal bandwidths. Because our models did not have many observations close to the cutoff point, shorter bandwidths served as tougher tests for the significance of the local average treatment effects. Second, because bandwidth selectors could generate substantial bias in the calculated estimator, we derived estimates of average treatment effect that are robust to MSE optimal bandwidths.20 Third, because the vaccination rates may have been influenced by the cumulative vaccination rates, we conducted a set of analyses including the cumulative vaccination rate as a control. Finally, we conducted placebo tests to assess the validity of the treatment cut-off. To address the possibility that the April 23rd cutoff for the US, being a Friday, simply reflects lower vaccination rates on the weekend, the first placebo test had 16th of April as its cutoff. The remaining placebo tests switched the cutoff dates for the US and Europe/UK.
RESULTS
Our study analyzed vaccination rates in Europe and the US between January 1, 2021, and September 1, 2021. The European nations included in the study are listed in the supplement. The cumulative vaccination rates in the US were daily, and those in Europe were weekly averages (Supplementary Fig. 1).
United States
On April 23, 2021, the day the US Center for Disease Control’s ACIP convened to vote on the continued administration of the Johnson & Johnson vaccine, the daily vaccination rate seemed to have experienced discontinuities in all three types of vaccines. The local average treatment effect of the ACIP meeting was −0.249 (95% confidence interval [CI], −0.360 to −0.138) for all vaccines, −0.133 (95% CI, −0.189 to −0.076) for Pfizer, −0.064 (95% CI, −0.115 to −0.012) for Moderna, and −0.038 (95% CI, −0.047 to −0.030) for Johnson & Johnson (Fig. 1A, Table 2). These are sizeable effects, as they are larger than half of each vaccine’s mean daily vaccination rates.
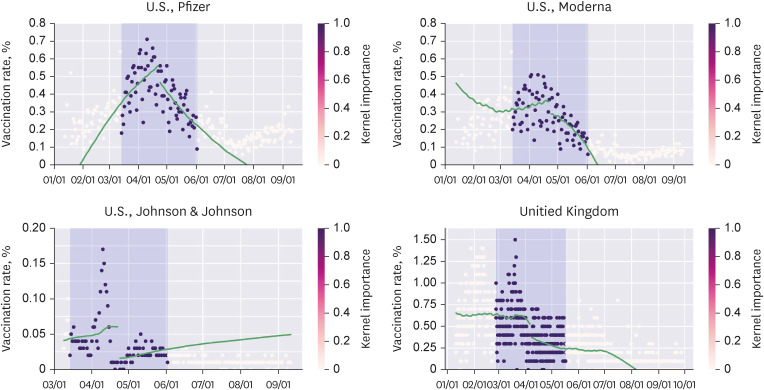
Fig. 1
Regression discontinuities in the United States with (A) April 23rd, 2021, as the cutoff (B) June 23rd as the cutoff.
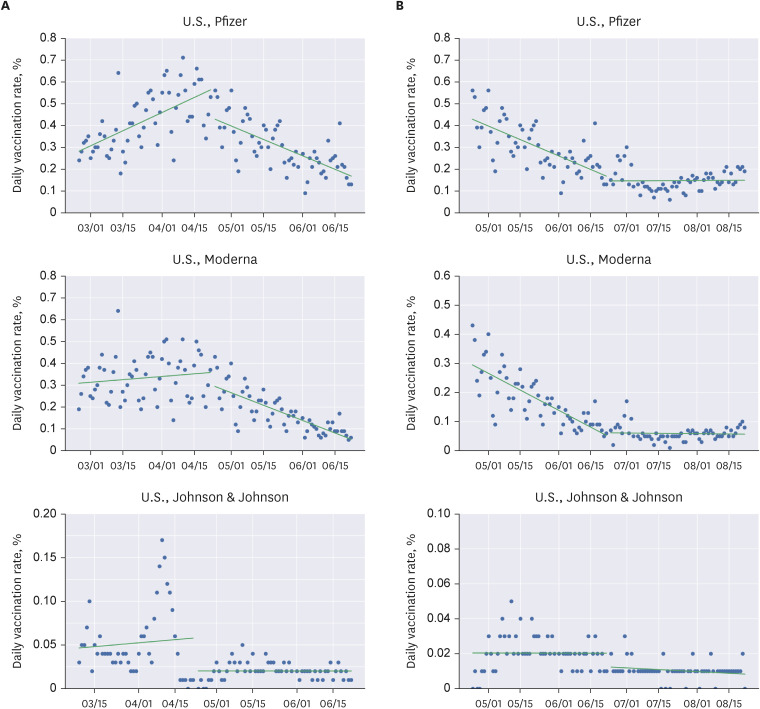
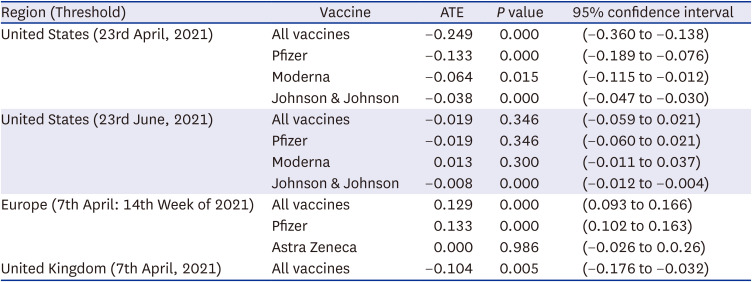
Table 2
Main analysis
In contrast, on June 23, 2021, on the day an ACIP meeting was held regarding mRNA vaccines and myocarditis, the daily vaccination rate did not exhibit any substantial discontinuities. The change in vaccination rate was −0.019 (95% CI, −0.059 to 0.021) for all vaccines, −0.019 (95% CI, −0.060 to 0.021) for Pfizer, 0.013 (95% CI, −0.011 to 0.037) for Moderna, and −0.008 (95% CI, −0.012 to −0.004) for Johnson & Johnson (Fig. 1B, Table 2). Despite a P value < 0.001 for the Johnson & Johnson vaccine, the treatment effect was small.
Europe
On April 7th, 2021, which was the day the EMA held a press briefing regarding Oxford/AstraZeneca’s connection to thromboembolic events, no significant drop in the weekly averages of vaccination rates was observed. The change in vaccination rate was 0.129 (95% CI, 0.093 to 0.166) for all vaccines, 0.133 (95% CI, 0.102 to 0.163) for Pfizer, and −0.000 (95% CI, −0.026 to 0.026) for Oxford/AstraZeneca (Fig. 2, Table 2).
Fig. 2
Regression discontinuities in the United Kingdom and Europe with April 7th, 2021, as the cutoff.
When the RDiT analysis was conducted only among European countries that reported daily vaccination rates, there was no observable drop in vaccination rates. Oxford/AstraZeneca showed similar rates to pretreatment levels, whereas Pfizer’s vaccination rate increased by 0.130 (95% CI, 0.060 to 0.210) (Supplementary Fig. 2).
United Kingdom
In the UK, a significant drop was observed in the first dose vaccination rates following the reports on the EMA’s press briefing on Oxford/AstraZeneca’s connection to thromboembolic events on April 7th. The first-dose vaccination rate for all vaccines changed by −0.104 (95% CI, −0.176 to −0.032) (Fig. 2, Table 2), which amounts to approximately a third of the mean daily vaccination rate in the UK.
Sensitivity analysis
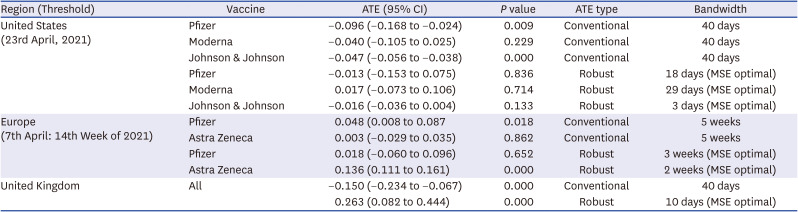
To evaluate the robustness of the discontinuity, sensitivity tests were performed on the US data using 40-day and MSE-optimal bandwidths and by conducting placebo tests with different cutoff thresholds. With 40-day bandwidths in the US, Pfizer and Johnson & Johnson vaccines exhibited discontinuities on April 23, 2021, with average treatment effects of −0.096 (95% CI, −0.168 to −0.024) and −0.047 (95% CI, −0.056 to −0.038), respectively. However, the results were not robust to MSE optimal bandwidths. Because the unit of analysis was country-day, the MSE-optimal bandwidths severely restricted the sample. Fig. 3 illustrates the results of sensitivity analysis when the cumulative vaccination rate was included as a covariate.
In the UK, vaccination rates fell significantly after April 7, 2021, in a sensitivity test that used a 40-day bandwidth. The first-dose vaccination rates changed by −0.150 (95% CI, −0.234 to −0.067) after the cutoff. However, as with the US, these results are not robust to MSE optimal bandwidths (Table 3).
Table 3
Sensitivity tests
Finally, the placebo tests yielded the expected results, with the exception of the Johnson and Johnson vaccines in the US (Supplementary Table 2). The Friday the week before the US’s 23rd April, 2021 threshold did not result in a negative regression discontinuity. Using Europe’s cut-off date in the US and vice versa also yielded no significant drop in vaccination rates (Supplementary Table 2).
DISCUSSION
The EMA statement related to TTS caused vaccine discontinuity in the UK and US. However, reports of myocarditis were not related to vaccine discontinuities. The following factors could have affected the differences in discontinuities between the two vaccine platforms.
(1) Fatality rate of severe adverse events
Both adverse events occurred mostly in the younger population, depending on the case. TTS had a fatality rate of 20–30%.21 Conversely, very rare fatal cases of myocarditis have been reported.22
(2) Differences in policy responses to vaccines
Regulators placed age limits based on the incidence of adverse events and fatality rates.10 Oxford/AstraZeneca is restricted in most countries. Conversely, despite safety concerns regarding mRNA vaccines among children, no age restriction was imposed on the older population (> 12 years).
(3) Confidence gaps between the vaccine platforms
The survey conducted by YouGov, a British polling firm, shows that confidence in the Oxford/AstraZeneca vaccine decreased sharply in European countries (February and March 2021).23
(4) Date of publication of adverse events
The adverse reactions of the mRNA vaccine were acknowledged two months later.22 Furthermore, the time to confirm rare adverse events did not significantly affect the entire population.
This study is the first to evaluate how government announcements on severe vaccine-related side effects had an impact on the vaccination rate based on data from Western countries that administered multiple types of vaccines. Additionally, changes over time were observed in RDiT analyses.
This study had several limitations. First, as a time-series analysis, we could not include all the factors that changed over time in our study design. For instance, regulatory decisions by countries regarding the rapid spread of the delta variant and increasing public awareness regarding vaccines. Second, despite the gap of 2 months, the trend of the epidemic could have acted as a confounding factor. The public is expected to return to pre-pandemic conditions in April owing to the high vaccination rate and social distancing schemes. However, with the surge in the delta variant in June, countries have emphasized the importance of vaccination.24 Third, decreased vaccination rates could be influenced by a decline in the target groups owing to the EMA statement.25 However, it should be noted that the US did not modify the age recommendation. In addition, some European countries have restricted the use of Oxford/AstraZeneca to the younger population before the EMA statement. Fourth, vaccination could be independently affected by disparities in vaccine supply. Even though the target countries in our study achieved a smooth supply of vaccines, most countries faced limited supplies in the first half of 2021.26 Moreover, several European countries have offered alternative vaccines to replace Oxford/AstraZeneca.27 Therefore, it is possible that vaccination rates are less affected by the adverse effects of adenoviral vector vaccines. Lastly, vaccination rates may have been influenced by cumulative vaccination rates. Despite high vaccine acceptance in some countries, the vaccination rate could not reach > 80% of the population; an inclined S pattern can be seen in the vaccination curve.28 However, even if vaccine hesitancy is influenced by the cumulative vaccination rate, mRNA vaccines should be most affected by the intensive media coverage in June. However, there were no significant shifts in the mRNA vaccination rates.
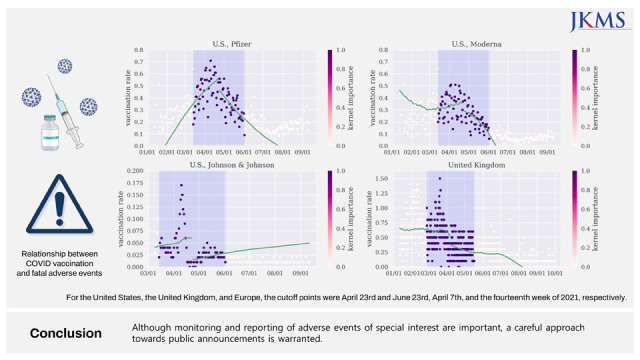
In conclusion, vaccine conviction is a key component of high vaccination coverage to overcome the pandemic. The relationship between vaccine acceptance, hesitancy, and documentation of AESI should be highlighted when implementing the vaccine coverage plan. Although it is important to monitor and report adverse effects of vaccines, a careful approach towards public announcements is warranted.
 XML Download
XML Download