

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Since the first report of infection with the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) omicron variant in South Africa on November 24, 2021, the omicron variant has been rapidly spreading worldwide.1 The first omicron infection in South Korea was reported on December 1, 2021.2 In Korea, the percentage of SARS-CoV-2 sequences identified as omicron among samples subjected to weekly variant testing by the Korea Disease Control and Prevention Agency (KDCA) increased from 0.2% during the week ending on December 4, 2021, to 50.3% during the week ending on January 22 and 80.0% during the week ending on January 29, 2022.3 With the emergence of the omicron variant, the incidence of coronavirus disease 2019 (COVID-19) reached record levels in Korean children. As of December 31, 2021, the cumulative number of pediatric COVID-19 cases (0–19 years) in Korea was 113,348. However, from January 1 to March 31, 2022, more than 3.3 million pediatric cases were reported.3
Although the omicron variant is associated with increased transmissibility and partial escape from infection- or vaccine-induced immunity,4 it causes less severe disease than the delta variant.5678910 During the first omicron wave in South Africa, increased hospitalization rates were observed with rising case numbers of pediatric COVID-19, but most children with omicron infection had mild to moderate disease.6 Among the United States children and adolescents, during the delta and omicron predominant periods, the omicron variant peak was four times that of the delta variant peak, with the largest increase in children aged 0 to 4 years.4 Compared to the delta predominance, hospital length of stay and the proportion of hospitalized pediatric patients requiring intensive care unit (ICU) admission were lower during the omicron predominance.48 However, data on clinical characteristics and disease severity according to different SARS-CoV-2 variants and risk factors for severe diseases in children and adolescents are still limited. Awareness of the clinical characteristics of SARS-CoV-2 infections by different variants would help to respond appropriately to the next epidemic.
In this study, we aimed to evaluate the clinical characteristics and outcomes of hospitalized children with laboratory-confirmed SARS-CoV-2 infection before and after omicron became the predominant variant in Korea. In addition, we analyzed the risk factors associated with the severity of omicron variant infection compared with delta variant infection.
METHODS
Study design
We conducted a multicenter retrospective cohort study in hospitalized patients aged ≤ 18 years with laboratory-confirmed SARS-CoV-2 infection by real-time reverse transcription polymerase chain reaction at five university hospitals in South Korea. The five study sites are dedicated COVID-19 hospitals and are located in four different regions in Korea. The cohort entrance date for patients was the day of confirmed SARS-CoV-2 infection. To obtain data on omicron, we collected the data of hospitalized patients with confirmed SARS-CoV-2 infection from January 1 to March 31, 2022. To compare these data with those from the period before omicron, we utilized some of the previously collected data from another study11; the data were obtained from 753 patients with confirmed SARS-CoV-2 infection from January 1 to December 31, 2021, in 8 hospitals, including the current study sites (Supplementary Fig. 1).
The study periods were divided into the delta and omicron periods, which were defined as the periods when the corresponding variants accounted for > 90% of sequenced isolates according to nationwide data from the KDCA.3 According to the KDCA data, we defined the delta period as August 23, 2021 to January 2, 2022, and the omicron period as January 30 to March 31, 2022. We compared the clinical data of all hospitalized children with COVID-19 in the 5 study hospitals between the two periods.
Data and definitions
We reviewed the medical charts of the study patients using standardized case report forms. Data regarding the primary reason for hospital admission, symptoms at admission, underlying medical conditions, clinical diagnosis of SARS-CoV-2 infection, the need for respiratory support, and specific therapy for COVID-19 were collected.
In Korea, mandatory facility quarantine and hospitalization regulations were completely lifted in late November 2021. Since the decision for hospitalization and allocation of hospitalization resources to COVID-19 patients were primarily under the management of the KCDA and guided by the national COVID-19 response system, there were discrepancies with clinicians’ judgment on the need for hospitalization. Therefore, we reclassified ‘necessary admission’ based on the severity of COVID-19-related symptoms and signs and the risk for progression to severe illness in the adjusted comparisons of clinical severity and outcomes during the two periods. Reasons for admission that were likely not COVID-19 related included categories such as simple isolation, inpatient surgery, or asymptomatic nosocomial infection (positive for SARS-CoV-2 in universal inpatient screening). Primary classification of necessary admission was performed on the basis of the researchers’ judgment at each study site. Subsequently, two researchers (SHC and KWY) conducted a secondary review based on the collected case report form data. The Pediatric Medical Complexity Algorithm was used to categorize patients with no chronic disease, noncomplex chronic disease, and complex chronic disease.1213 The presence of complex chronic disease was defined as having chronic conditions in ≥ 2 body systems, a progressive chronic disease, malignancy, or continuous dependence on technology for at least 6 months.13 Obesity was defined as the presence of an age-sex-standardized weight-for-height (aged 0–23 months) or body mass index (aged ≥ 2 years) ≥ 95th percentile based on the 2017 Korean National Growth Chart.14 Obesity was not included in the category of chronic diseases.
The severity of COVID-19 was defined as follows: mild, upper respiratory infection not requiring oxygen or a simple febrile seizure; moderate, lower respiratory tract infection not requiring oxygen, croup/a febrile seizure requiring oxygen or a change in mental status without seizure; severe, lower respiratory tract infection requiring oxygen via nasal prongs or a mask, COVID-19-related conditions requiring a high-flow nasal cannula at ≤ 2 L/kg/min, or COVID-19-related end-organ (such as brain, kidney, or heart) damage; critical, unstable COVID-19-related conditions requiring ICU admission, mechanical ventilation, or extracorporeal membrane oxygenation, sepsis/septic shock, multiple organ failure, or death. To compare the characteristics according to severity, moderate, severe, and critical conditions were classified as serious illness.
Statistical analysis
We compared demographic data, clinical characteristics, illness severity, and clinical outcomes between the delta- and omicron-predominant periods and further stratified these data by age group (0–4 years; 5–11 years; 12–18 years). We used descriptive statistics, including medians, interquartile ranges (IQRs), counts and proportions. Categorical variables were compared by Fisher’s exact test and the χ2 test. Continuous variables were compared by the Mann-Whitney U test and Kruskal-Wallis test. Multivariable logistic regression was performed to assess the independent factors associated with the severity of COVID-19 during the delta and omicron-dominant periods, and adjusted odds ratios (aORs) and 95% confidence intervals (CIs) were calculated. Variables included age group, medical complexity, and underlying medical diseases for multivariable logistic regression analysis. We tested for multicollinearity with variance inflation factors to control confounding variables and performed the Hosmer-Lemeshow test for goodness-of-fit. Two-sided P values < 0.05 were considered statistically significant. Data were analyzed using Prism 9.3.1 (GraphPad Software Inc., San Diego, CA, USA).
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board (IRB) of Seoul National University Hospital, and the need for informed consent was waived (approved No. 2201-023-1286). In addition, this study was approved by the institutional review boards of each hospital, and the approved IRB numbers for each hospital were as follows: 2202-009-111 (Pusan National University Hospital), 2022-10-005 (Jeju National University Hospital), 2022-04-031 (Chungbuk National University Hospital), and 2022-10-021 (Nowon Eulji University Hospital).
RESULTS
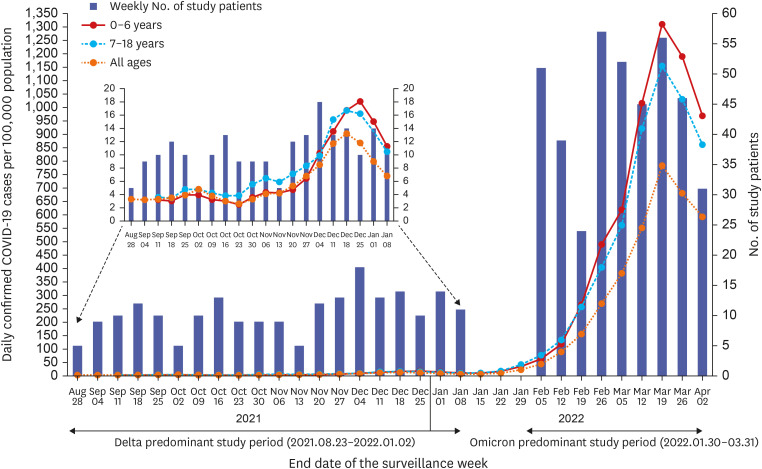
We identified a total of 612 hospitalized pediatric patients with SARS-CoV-2 infection, including 211 during the delta period and 401 during the omicron period (Supplementary Fig. 1). The median weekly numbers of hospitalizations during the delta and omicron periods were 10 (95% CI, 9–13) and 46 (95% CI, 31–56), respectively (Fig. 1).
Fig. 1
National incidence of COVID-19 and weekly distributions of study patients. The figure shows daily new confirmed COVID-19 cases per million people (7-day rolling average) in South Korea from August 22, 2021 to April 2, 2022. Nationwide population data were available from press releases by the Korea Disease Control and Prevention Agency (http://ncov.mohw.go.kr/en).3 The national incidence rate of COVID-19 (daily confirmed cases per 100,000 children) peaked during the omicron period in the week ending March 19, 2022, with 1,309.9 infected individuals aged 0–6 and 1,154.5 infected individuals aged 7–18 years. The incidence rates among children aged 0–6 and 7–18 years during the peak week in the omicron period were 72.4 and 69.1 times higher than those during the delta period.
COVID-19 = coronavirus disease 2019.
Characteristics of the study population
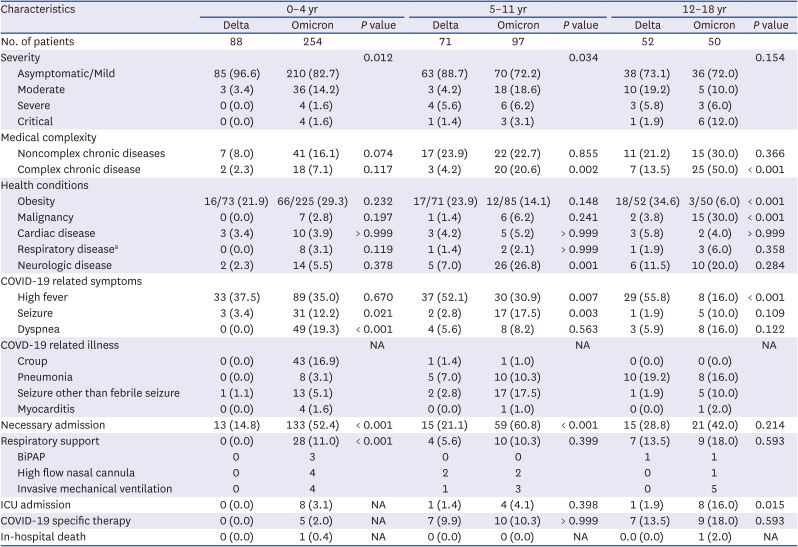
The characteristics of the study patients are summarized in Table 1. The median age of patients during the omicron period was significantly younger than that during the delta period (25 vs. 73 months; P < 0.001). In the omicron period, the proportions of patients with complex chronic diseases (12.5% vs. 6.2%; P < 0.001), malignancy (7.0% vs. 1.4%; P = 0.002), and neurologic disorders (12.5% vs. 6.2%; P = 0.017) were significantly higher than those in the delta period. Neurologic disorders were the most common underlying chronic medical condition throughout the two periods (Supplementary Table 1). The proportions of patients with croup (11.0%) and seizures (13.2%) increased significantly during the omicron period. The proportion of necessary admission for COVID-19 during the omicron period was significantly higher than that during the delta period (53.1% vs. 20.4%; P < 0.001).
Table 1
Characteristics of patients by the variant dominance period
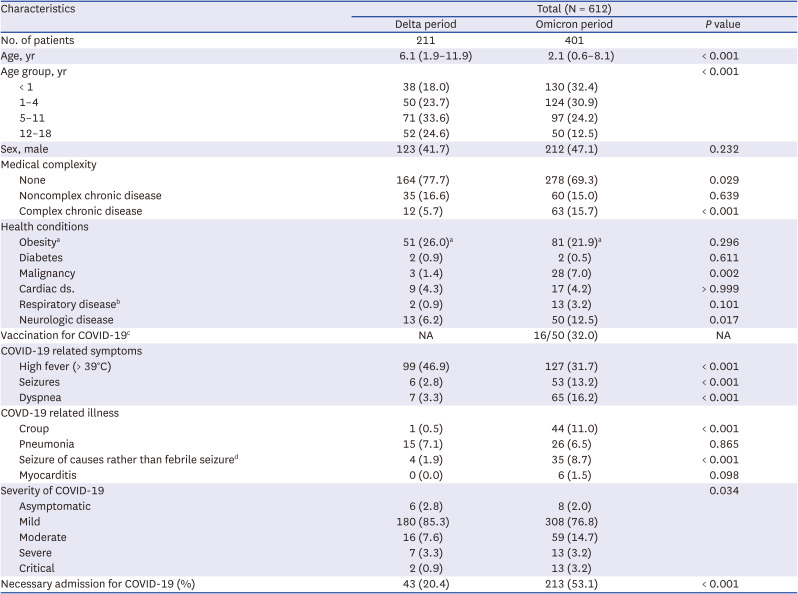
Values are presented as number (%) or median (interquartile range).
COVID-19 = coronavirus disease 2019, NA = non-available.
aObesity was not included in the category of chronic diseases. Data for obesity were available from 196/211 (92.9%) in the delta period and 370/401 (92.3%) in the omicron period.
bIncluded airway abnormality, oxygen dependency, and tracheostomy dependency. Excluded asthma.
cData were collected only from adolescents aged 12–18 years during the omicron period. In South Korea, COVID-19 vaccination for children aged 12–15 years began on November 1, 2021. Patients who completed COVID-19 vaccination were defined as those who had received the second dose of a 2-dose series ≥ 14 days after the final dose in the primary series before receiving a positive severe acute respiratory syndrome coronavirus 2 test result.
dIncluding febrile status epilepticus, fever-provoked seizures, exacerbated seizures in patients with known epilepsy, and seizures in COVID-19-related encephalitis or encephalopathy.
In the subgroup analysis of necessary admission (Table 2), there were no significant differences in the proportions of underlying chronic diseases and seizures between the two periods. However, compared to the delta period, the proportions of young children aged 0–4 years (61.5% vs. 30.3%) and patients with croup (17.8% vs. 2.3%) were higher during the omicron period. The proportions of adolescents aged 12–18 years (9.9% vs. 34.9%) and individuals with obesity (21.9% vs. 39.5%), pneumonia (12.2% vs. 34.9%), moderate to critical severity (39.9% vs. 58.1%), and specific therapy for COVID-19 (11.3% vs. 32.6%) during the omicron period were significantly lower than those during the delta period. Compared with those in the delta period, the proportions of patients requiring ICU admission (8.9% vs. 4.6%) and invasive mechanical ventilation (5.6% vs. 2.3%) during the omicron period were higher, but the differences were not statistically significant.
Table 2
Comparison of necessary admission by the variant dominance period
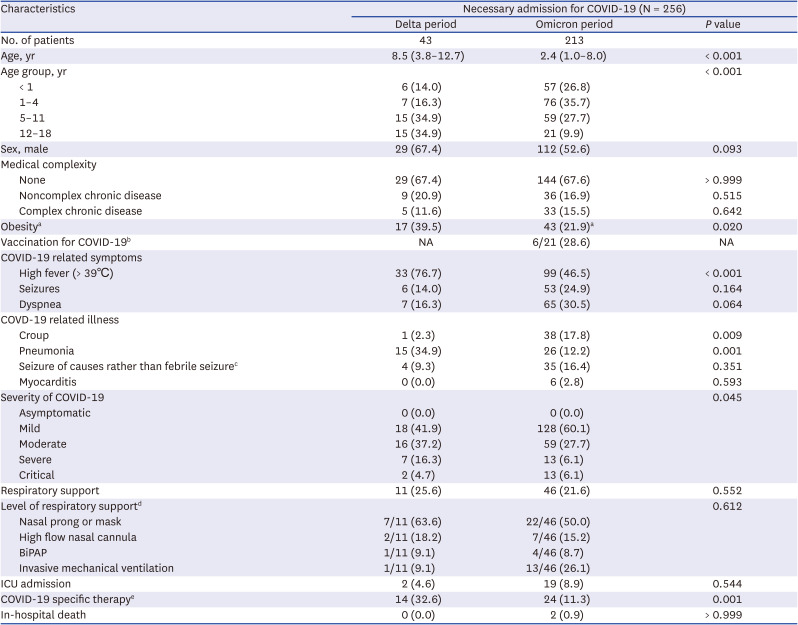
Values are presented as number (%) or median (interquartile range).
COVID-19 = coronavirus disease 2019, NA = non-available, BiPAP = bilevel positive airway pressure, ICU = intensive care unit.
aObesity was not included in the category of chronic diseases. Data for obesity were available from 43/43 (100.0%) in the delta period and 196/213 (92.0) in the omicron period.
bData were collected only from adolescents aged 12–18 years during the omicron period. In South Korea, COVID-19 vaccination for children aged 12–15 years began on November 1, 2021. Patients who completed COVID-19 vaccination were defined as those who had received the second dose of a 2-dose series ≥ 14 days after the final dose in the primary series before receiving a positive severe acute respiratory syndrome coronavirus 2 test result.
cIncluding febrile status epilepticus, fever-provoked seizures, exacerbated seizures in patients with known epilepsy, and seizures in COVID-19-related encephalitis or encephalopathy.
dThe highest level of respiratory support applied to the patient.
eAdministration of remdesivir, systemic steroids (dexamethasone 0.15 mg/kg for 10 days or equivalent glucocorticoids), or tocilizumab.
In the subgroup analysis by age group, there were differences in medical complexity, health conditions, and COVID-19-related symptoms and illness between the two periods (Table 3). Among children aged 0–4 years, there were no significant differences in the proportions of underlying chronic diseases and obesity between the two periods. In the 5–11 and 12–18 years age groups, a higher proportion of patients during the omicron period (20.6% and 50.0%, respectively) had complex chronic diseases than during the delta period (4.2% and 13.5%, respectively; P < 0.01 in both). Among adolescents aged 12–18 years, the proportion of obese patients during the omicron period (6.0%) was significantly lower than that during the delta period (34.6%). Compared with the delta period, the proportions of patients with moderate severity were significantly increased during the omicron period among children in the 0–4 and 5–11 years age groups.
Table 3
Characteristics of the study patients by age group and variant predominance period
COVID-19 severity
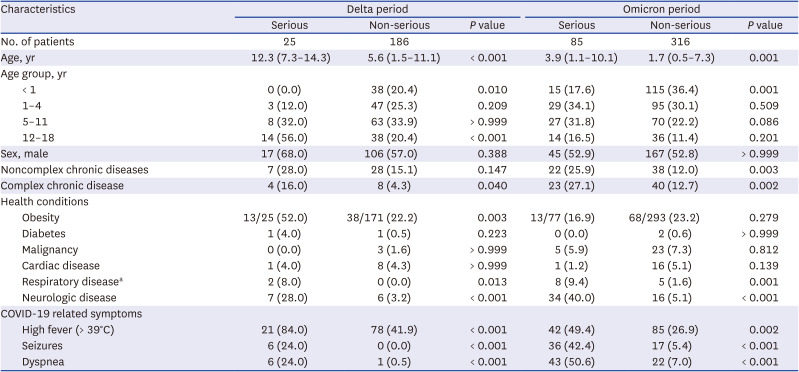
In the total study period, 2.3% (14/612) of patients were asymptomatic. During the omicron and delta periods, the proportions of individuals with serious illness (moderate, severe, and critical severity) were 21.2% and 11.8%, respectively (P = 0.034). The median age of patients with severe/critical illness was significantly older than that of patients with moderate or asymptomatic/mild illness during the omicron period: severe/critical, 9.9 years (IQR, 3.3–13.0) vs. moderate, 2.2 years (IQR, 1.0–7.4) vs. asymptomatic/mild, 1.7 years (IQR 0.5–7.3) years; P < 0.001 (Supplementary Fig. 2).
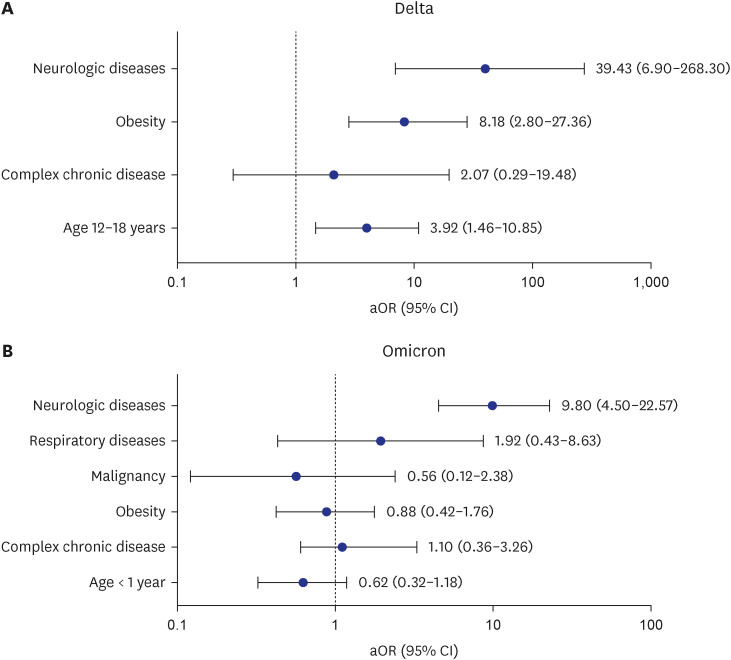
The proportions of patients with complex chronic diseases, respiratory diseases except for asthma, and neurologic diseases were significantly higher among patients with serious illness during the two periods (Table 4). There was a significant association between medical complexity and illness severity. Compared with patients without chronic diseases, patients with complex chronic diseases had higher odds of serious illness, with an aOR of 5.36 (95% CI, 1.30–19.43) during the delta period and an aOR of 3.42 (95% CI, 1.84–6.30) during the omicron period (Fig. 2). In the multivariable logistic regression analysis, the independent risks associated with serious COVID-19 illness were obesity (aOR, 8.18; P < 0.001) and neurologic diseases (aOR, 39.43; P < 0.001) and in adolescents aged 12–18 years (aOR, 3.92; P = 0.007) during the delta period (Fig. 3A, Supplementary Tables 2 and 3). However, the presence of neurologic disease (aOR, 9.80; P < 0.001) was the only risk factor for serious illness during the omicron period (Fig. 3B, Supplementary Tables 2 and 4).
Table 4
Comparison of serious COVID-19 with non-serious COVID-19 by predominant variant period
Values are presented as number (%) or median (interquartile range). Serious COVID-19: moderate, severe, or critical severity; Non-serious COVID-19: asymptomatic or mild severity.
COVID-19 = coronavirus disease 2019.
aIncluded airway abnormality, oxygen dependency, and tracheostomy dependency. Excluded asthma.
Fig. 2
Association between the underlying medical conditions and coronavirus disease 2019 severity. (A) Distribution of illness severity according to medical complexity and the association between medical complexity and moderate or severe/critical illness during the delta period. (B) Distribution of illness severity according to medical complexity and the association between medical complexity and moderate or severe/critical illness during the omicron period.
aOR = adjusted odds ratio, CI = confidence interval.
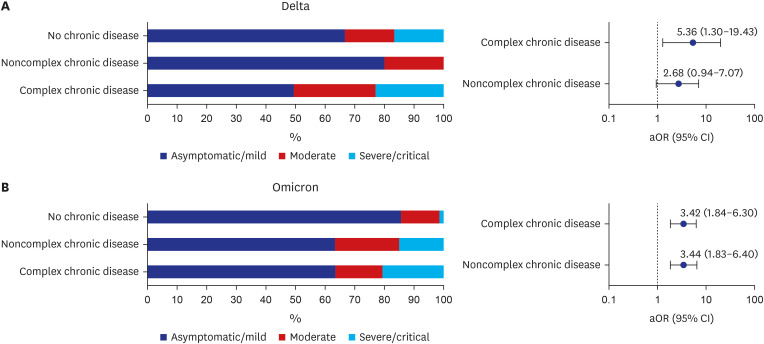
Fig. 3
Predictors of serious illness among patients with coronavirus disease 2019. (A) The delta period and (B) the omicron period.
aOR = adjusted odds ratio, CI = confidence interval.
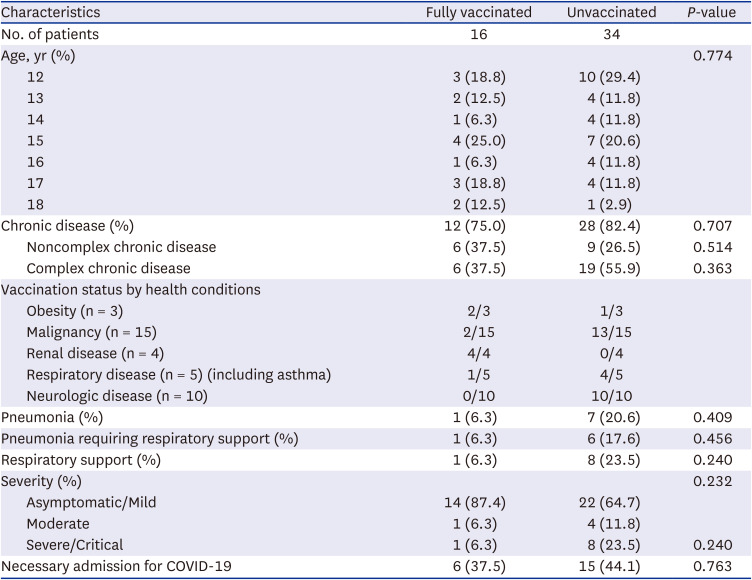
During the omicron period, 32.0% (16/50) of adolescents aged 12–18 years were fully vaccinated against COVID-19 (≥ 14 days after the final dose in the primary series) (Table 5). None of the patients with neurologic diseases received COVID-19 vaccination. The proportions of serious illness were 12.5% in the fully vaccinated group and 35.3% in the unvaccinated group (aOR, 0.57; 95% CI, 0.02–5.92; P = 0.667).
Table 5
Characteristics and outcomes by COVID-19 vaccination status among adolescents aged 12–18 years during the omicron
COVID-19-related illness
The patients with COVID-19 pneumonia during the omicron period were younger than those during the delta period (median, 7.9 vs. 12.6 years; P = 0.020). Compared with the delta period, patients with COVID-19 pneumonia during the omicron period had a higher proportion of complex chronic diseases (53.8% vs. 13.3%; P = 0.019) and a lower proportion of obesity (7.7% vs. 73.3%; P < 0.001) (Supplementary Table 5).
Compared with that in the delta period, seizures in patients without underlying neurological disease tended to be more frequent (60.4% vs. 33.3%; P = 0.386) during the omicron period (Supplementary Table 6). Among patients with seizures during the omicron period, obesity (n = 11; 9 without underlying chronic diseases, 2 with neurologic diseases) was the most common underlying medical condition after neurologic diseases (n = 21, 43.8%). All seizure patients with accompanying pneumonia (n = 6) had neurologic diseases during the omicron period.
Forty-four patients with croup (median age, 13 months) were identified during the omicron period. Thirteen (29.5%) patients needed respiratory support, mostly oxygen therapy via nasal prongs (Supplementary Table 7). Six patients had myocarditis, and two patients with myocarditis died during the omicron period: a 13-month-old girl without any underlying medical condition and a 17-year-old girl with central apnea and encephalopathy. The data of the patients with myocarditis are summarized in Supplementary Table 8.
DISCUSSION
In this study, the proportions of COVID-19-related hospitalizations among young children aged 0–4 years and patients with comorbidities were significantly higher during the omicron period than during the delta period. During the omicron period, different clinical illnesses, such as croup and seizures, were frequently observed. Overall disease severity in the omicron dominant period, especially moderate illness, increased in parallel with the increase in young children with croup or febrile seizures requiring supplemental oxygen. There was no significant difference in the proportions of severe and critical COVID-19 during the two periods, and the majority of severe or critical patients had comorbidities.
Some studies in the US showed that the incidence rate of COVID-19 due to the omicron variant was 5–8 times that of the incidence rate of COVID-19 due to the delta variant in children aged < 5 years, but the proportion of severe clinical outcomes was lower.810 Although disease severity appeared lower with the omicron variant, the daily 7-day moving average of COVID-19 cases, emergency department visits, and hospitalization rapidly increased during the omicron period in the US.15 In South Korea, the national incidence rate of COVID-19 (daily confirmed cases per 100,000 children) peaked during the omicron period in the week ending March 19, 2022, with 1,309.9 infected individuals aged 0–6 and 1,154.5 infected individuals aged 7–18 years. The incidence rates among children aged 0–6 and 7–18 years during the peak week in the omicron period were 72.4 and 69.1 times higher than those during the delta period.3 The high volume of outpatients and hospitalizations resulting from high transmission rates during a short period strained local health care systems.
In a Qatari study,5 infection with the omicron variant was associated with significantly lower odds of moderate or severe/critical disease than infection with the delta variant (aOR, 0.12; P < 0.001), and the presence of comorbidity was associated with higher odds of moderate or severe/critical disease (aOR, 3.16; P = 0.033). In our study, during the omicron period, the presence of complex chronic diseases was significantly associated with serious COVID-19. In the multivariable analysis, neurologic disease was a predictor of serious illness (aOR, 9.80; P < 0.001). Shi et al.16 reported that during the period of omicron predominance, a larger proportion of children aged 5–11 years hospitalized with COVID-19 had neurologic diseases (33.4%) compared with those hospitalized during the period of delta predominance (24.5%; P = 0.02). Several studies noted that neurologic disorders increased the risk for severe illness in other respiratory viral infections, such as influenza or respiratory syncytial virus.17181920 Havers et al.19 noted that children with neurologic disorders had 5- to 7-fold higher risk for hospitalization due to respiratory infections than all children. In patients with neurologic disorders, several factors may contribute to the increased risk of lower respiratory tract infections, such as impaired mobility, decreased muscle tone, aspiration risk, inability to clear secretions, and likelihood of the underlying condition being exacerbated by infection.18 In our study, half of the patients with neurologic diseases had a complex chronic disease, and some of the patients were bedridden or tracheostomy dependent.
In previous studies, obesity was associated with an increased risk for severe COVID-19 in children.72122 In the study by Shi et al.,16 the proportion of obesity among children hospitalized with COVID-19 was lower during the omicron period than during the delta period (21.3% vs. 30.6%; P = 0.02). In our study, in contrast to the delta period, obesity was not a risk factor for serious illness in the omicron period. Furthermore, there was a significant difference in the proportion of obesity in only those aged 12–18 years between the two periods. Although it could not be confirmed in our study, we cautiously suggest that this reason may be related to COVID-19 vaccination. In Korea, COVID-19 vaccination eligibility was expanded to include children aged 12–15 years on November 1, 2021.323 As of January 30, 2022 (the first entrance date of the omicron study period), 59.4% of the population aged 12–17 years and 92.6% of those aged 18–19 years had completed the COVID-19 primary vaccination series.3 Many healthy and obese adolescents may have been vaccinated against COVID-19. In the US, once omicron became predominant in December 2021, the monthly hospitalization rate among unvaccinated adolescents aged 12–17 years was six times that among fully vaccinated adolescents.4 Price et al.24 reported that among adolescents aged 12–18 years, vaccine effectiveness against critical COVID-19 was 79% (95% CI, 51–91) during the omicron-predominant period.
Similar to this study, several studies reported that the incidence of COVID-19-associated croup increased significantly during the omicron period.252627 Martin et al.26 noted that SARS-CoV-2-positive croup rates increased with progression from the pre-omicron to the omicron period in the US (1.5% vs. 4.1%, P < 0.001). Young children are especially vulnerable to upper airway infection due to their relatively small upper respiratory tract. Hui et al.28 reported that omicron replicated faster in the bronchi but less efficiently in the lung parenchyma than all other studied SARS-CoV-2 variants. The lower replication competence of the omicron variant in human lungs may explain the reduced severity of infection due to the omicron variant.
In our study, seizures in patients without underlying neurological diseases were observed frequently (60.4%) during the omicron period. Ludvigsson29 reported the data of three patients with COVID-19 and convulsions who were admitted to a Swedish hospital during the omicron period. In a multicenter observation study from South Africa, seizures were identified in 25 (20.0%) of 125 children with available data.6 Twenty-one had uncomplicated seizures; however, four were not in the age range (age < 1 year or > 5 years) for febrile seizures.
This study has several limitations. First, since this study was conducted in a limited number of university hospitals, there was potential selection bias. It is possible that many patients with specific chronic diseases or health conditions were included. Furthermore, the decision for hospitalization and allocation of hospitalization resources to COVID-19 patients were primarily under national control, and the strategy against SARS-CoV-2 variants was changed with the epidemic situation. Second, due to the retrospective review of medical records, the judgment of the need for hospitalization or the severity of illness was potentially misclassified. Third, validation of the severity classification was not performed in this study. However, researchers reviewed the data throughout several steps and applied objective clinical indicators for the definition of severity. Fourth, there was a lack of specific analysis of the patients with severe to critical illness. Finally, our data do not represent the national situation, and these findings might not be generalizable to all Korean children and adolescents. Despite these limitations, we attempted to collect and analyze various clinical data from the majority of symptomatic pediatric patients aged 0 to 18 years. We described the characteristics of clinical illness by variants, such as croup and seizures, which were distinct features during the omicron era.
In conclusion, during the period of omicron dominance in South Korea, the proportion of hospitalized young children with moderate severity of COVID-19 significantly increased, coinciding with the high occurrence of croup and seizures. Among adolescents hospitalized with COVID-19 during the omicron period, the proportion of obese patients decreased significantly, and there was no significant change in overall disease severity. However, patients with complex chronic diseases had a high risk of severe COVID-19 in the two distinct variant-dominant periods. Therefore, COVID-19 vaccination should be recommended for vulnerable children with underlying medical complexities. In preparation for the emergence of the novel variants epidemic, hospital surge capacity and the ability of adequate healthcare systems for the pediatric population are imperative.
 XML Download
XML Download