

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Antimicrobial agents are prescribed to 17–90% of terminally ill patients, although the appropriateness of this is currently debated.12345678910 Excess antibiotic use raises concerns about futile use, adverse events including increased Clostridiodes difficile infections and multidrug-resistant organisms, as well as significant patient and social cost burdens.910 The Infectious Diseases Society of America (IDSA) and the Society for Healthcare Epidemiology of America (SHEA) recommend that antimicrobial stewardship programs (ASPs) should be provided for decisions related to antibiotic treatment at the end of life of patients and suggest that antimicrobial agents should be withheld if prolonging survival is not a primary goal.11 However, determining whether to implement or withhold antimicrobial agents in terminally ill patients is difficult because of conflicting evidence, and requires an individualized approach and ethical consideration.1213141516
The impact of antimicrobial agents on terminally ill patients has not been consistently demonstrated. Previous research has shown that antimicrobial therapy is effective in alleviating urinary tract infections in patients with advanced cancer.171819 However, aside from urinary tract infections, the use of antibiotics often does not improve symptoms in terminally ill patients with suspected or known infections. Givens et al.15 reported that antimicrobial therapy for pneumonia was associated with improved survival but less comfort in patients with advanced dementia.
The Life-Sustaining Treatment Decision Act for end-of-life patients came into force in February 2018 in Korea.20 The act defines life-sustaining treatment (LST) as medical treatment by mechanical ventilation (MV), cardiopulmonary resuscitation (CPR), renal replacement therapy, chemotherapy, transfusion, extracorporeal life support, and inotropic treatments to a patient at the end of life, which merely extends the duration of the end-of-life process without curative effects. However, there has been no discussion on how to use antimicrobial agents in these patients, and no study has been conducted on the use of antimicrobial agents in terminally ill patients. Therefore, we investigated the nationwide situation of how antibiotics are prescribed to patients during the last 14 days of life to guide future actions for terminally ill patients. Furthermore, the appropriateness of the antibiotic prescriptions was evaluated.
METHODS
Study population and design
This nationwide multicenter retrospective cohort study was conducted in 13 hospitals in South Korea between November 1, 2018, and December 31, 2018. All patients older than 18 years who died at each hospital during the study period were included in the study. Eligible patients were identified by reviewing their electronic medical records to create a standardized case report form. The following information was collected: demographic characteristics, underlying comorbidities, cause of death, date of completion of LST form, microbiological testing, isolation of multidrug-resistant organisms’ class, number of antimicrobial agents in the last two weeks of life, and infectious disease (ID) consultation.
Definition
All the antimicrobial agents were included in the analysis. Patients receiving topical, ophthalmic, or otic antibiotics were excluded from the study. The amount of antimicrobial agents was measured by the days of therapy (DOT) and standardized for 1,000 patient-days. The Life-Sustaining Treatment Decision Act makes withholding and withdrawing LST possible using the legal determination form.20 This legal determination form is intended for patients with “serious chronic or acute illness nearing the end stages or likely to progress to a life-threatening state suddenly”. LST was defined as CPR, MV support, renal replacement therapy, chemotherapy, extracorporeal membrane oxygenation, transfusion, and use of inotropes. The form can be completed by any patient at any time or by the patient’s relative according to the Act. The completion of the LST form was divided into an LST form completed ≤ 14 days prior to death and an LST form completed > 14 days prior to death. ID specialists in each participating hospital assessed the antibiotic prescription as needing escalation, de-escalation, continuing, discontinuing or not assessable. Cases assessed as “Needing to continue” were considered appropriate antibiotic prescriptions, and other assessments were classified as inappropriate antibiotic prescriptions. Multidrug resistant (MDR) organisms include multidrug-resistant Acinetobacter baumannii (MRAB), vancomycin-resistant enterococci, methicillin-resistant Staphylococcus aureus, multidrug-resistant Pseudomonas aeruginosa (MRPA), and carbapenem-resistant Enterobacteriaceae (CRE).
Statistical analyses
Discrete data are presented as frequencies and percentages, and continuous variables are summarized as mean ± standard deviation or as median and interquartile range after the normality of data was tested using the Shapiro–Wilk normality test. Characteristics were compared between subgroups of appropriate versus inappropriate prescribing of antibiotics using the χ2, Fisher’s exact, two-sample t-, or Mann–Whitney U-tests, as appropriate. The factors associated with appropriate antibiotic administration were analyzed using univariable and multivariable logistic regression analyses. When the distribution of continuous data was skewed, log transformations of the data were applied for univariate analyses. The Hosmer–Lemeshow test was used for goodness of fit for the logistic regression models. Variables with a P value of < 0.10 in the univariate analysis were candidates for multivariable analysis. All analyses were performed using IBM SPSS Statistics for Windows (version 23.0; IBM Corp., Armonk, NY, USA).
Ethics statement
The study was approved by Institutional Review Board (IRB) of Kyungpook National University Chilgok Hospital (KNUCH 2019-09-008) and the local IRB of all participating hospitals. The requirement for informed consent was waived due to the observational retrospective nature of the study on deceased patients.
RESULTS
Patient characteristics
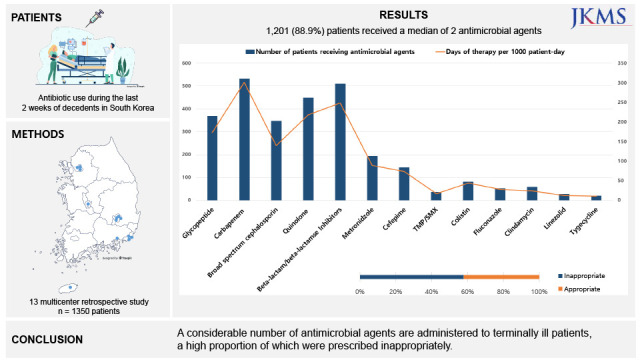
A total of 1,350 patients died at 13 hospitals between November 1, 2018, and December 31, 2018. The median age was 71.0 years, and 823 (61.0%) were male. A total of 613 patients (45.4%) had underlying malignant disease. Infectious causes accounted for 40.2% of the deaths (n = 543). At the time of death, 1,065 patients (78.5%) had LST documents, of whom 919 (86.3%) were completed at least 14 days before death. Culture studies were conducted on 1,110 patients and MDR pathogens were found in 325 patients (29.3%) (Table 1).
Table 1
Demographic characteristics of patients in the 14 days before death
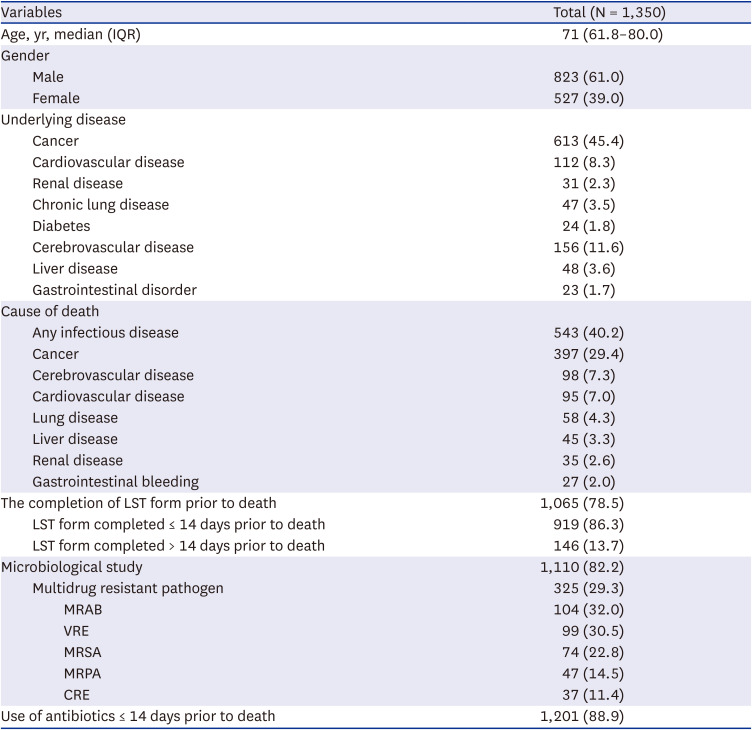
Values are presented as number (%) unless otherwise indicated.
IQR = interquartile range, LST = life-sustaining treatment, MRAB = multidrug-resistant Acinetobacter baumannii, VRE = vancomycin-resistant enterococci, MRSA = methicillin-resistant Staphylococcus aureus, MRPA = multidrug-resistant Pseudomonas aeruginosa, CRE = carbapenem-resistant Enterobacteriaceae.
Characteristics of antimicrobial use in patients within 14 days before death
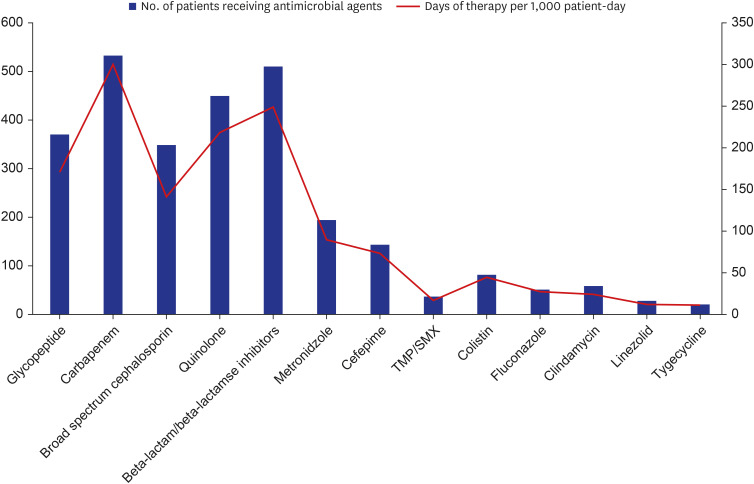
Among the 1,350 decedents, 1,201 (88.9%) patients received a median of two antimicrobial agents during the last 2 weeks of their lives, and 1,131 (83.8%) received antibiotics at the time of death. In 21,118 DOT for 14,218 patient-days, the consumption of carbapenems, β-lactam/β-lactamase inhibitors, and quinolone was 301.2, 248.8, and 218.2 DOTs per 1,000 patient-days, respectively. Of the 1,201 patients receiving antimicrobial agents, 533 received carbapenems (44.4%), followed by β-lactam/β-lactamase inhibitors (42.5%, n = 510), and quinolones (37.4%, n = 449) (Table 2 and Fig. 1).
Table 2
Characteristics of antimicrobial use in patients within 14 days before death
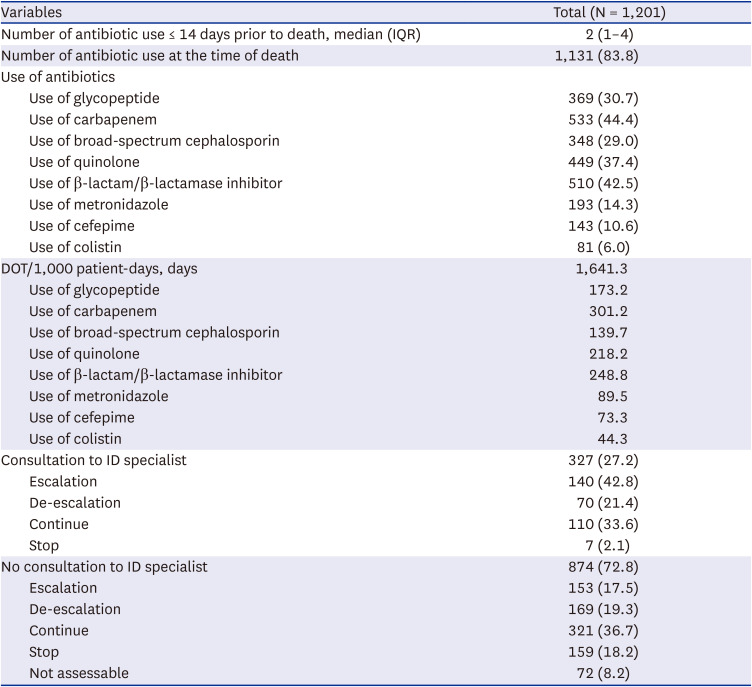
Of the 1,201 patients receiving antimicrobial agents, 327 (27.2%) were referred by ID specialists. Among the 327 patients with ID consultation, 140 (42.8%) required escalation, 70 (21.4%) needed de-escalation, 110 (33.6%) were assessed to continue and 7 (2.1%) were assessed to discontinue. Meanwhile, among 874 patients (72.8%) without any ID consultation, 153 (17.5%) were assessed as requiring escalation, 169 (19.3%) requiring de-escalation, 321 (36.7%) as continuing, 159 (18.2%) as discontinuing and 72 (8.2%) as not assessable (Table 2).
Comparison of characteristics between inappropriate antibiotic prescriptions and appropriate antibiotic prescriptions
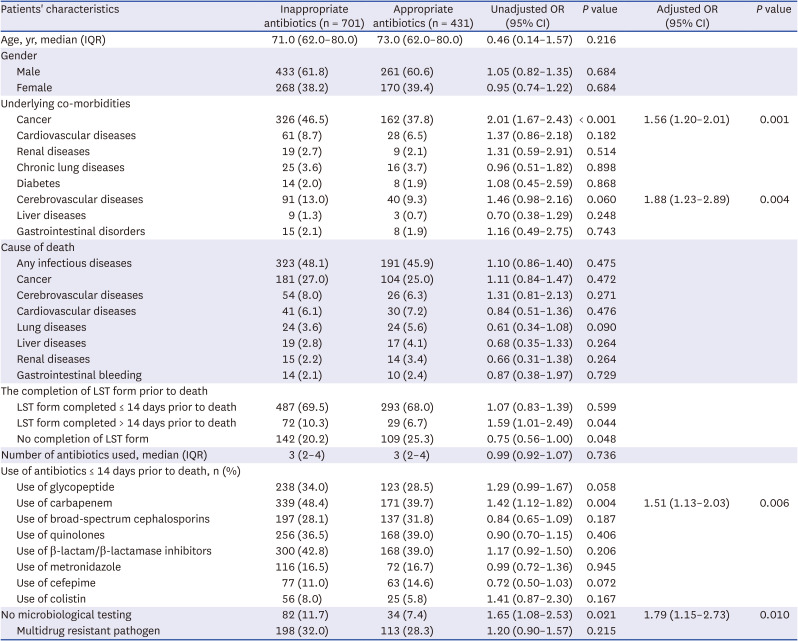
When categorized as either inappropriate (escalation, de-escalation, or discontinuing) or appropriate (i.e., continued), 701 (63.6%) antibiotic prescriptions were assessed as inappropriate, and 401 (36.4%) antibiotic prescriptions were assessed as appropriate. Table 3 describes the characteristics of the patients who were prescribed both inappropriate and appropriate antibiotics. There were no differences between the two groups regarding age, sex, cause of death, or isolation of MDR pathogens. Underlying cancer (P < 0.001), completion of LST form > 14 days prior to death (P = 0.044), no completion of LST form prior to death (P = 0.048), use of carbapenem (P = 0.004), and no microbiological testing (P = 0.021) were significantly more frequent in the inappropriate antibiotic prescribing group. Multivariable analysis showed that underlying cancer (odds ratio [OR], 1.56; 95% confidence interval [CI], 1.20–2.01; P = 0.047), underlying cerebrovascular disease (OR, 1.88; 95% CI, 1.23–2.89; P = 0.004), carbapenem use (OR, 1.51; 95% CI, 1.13–2.03; P = 0.006), and no microbiological testing (OR, 1.79; 95% CI, 1.15–2.73; P = 0.010) were independent predictors of inappropriate antibiotic prescriptions. The goodness of fit of the final logistic regression model appeared to be satisfactory (Hosmer-Lemeshow statistic, χ2 = 2.701, P = 0.259).
Table 3
Comparison of characteristics between inappropriate antibiotic prescriptions and appropriate antibiotic prescriptions (N = 1,132)
DISCUSSION
This nationwide cohort study showed that a high proportion of patients (88.9%) were treated with a median two antimicrobial agents in the last 2 weeks of life. A high consumption of broad-spectrum antimicrobial agents, especially carbapenems, was observed. Carbapenem was prescribed to approximately half of the patients (44.4%) in the highest amount (301.2 DOT per 1,000 patient-days). Only a small proportion of the patients (27.2%) were referred by ID specialists. We also found that a 63.6% of antibiotic prescriptions were inappropriate. Predictors of inappropriate antibiotic prescriptions were underlying cancer, underlying cerebrovascular disease, carbapenem use, and no microbiological testing.
Previous studies have shown that antimicrobial agents are commonly prescribed in terminally ill patients and that the proportion of antimicrobial use varies according to the study period and country.26921 The rate of antimicrobial agents prescribed in our study was 88.9%, similar to that observed in previous studies. In a Korean cohort of deceased patients treated in acute care hospitals (75.6% with solid tumors), 87.5% received antibiotic therapy lasting > 24 hours.9 Likewise, a US cohort study at a cancer centre showed that 1,070 (83%) received at least one antimicrobial agent among the 1,295 patients during the last 30 days of life.21 In a Japanese study, 136 (52.3%) of 260 hospitalized patients with an advanced illness also received antimicrobial therapy during the last 14 days of their life.2 A retrospective review of antimicrobial use in 137 Australian deceased patients in 2015 found that 62.7% had received antimicrobial therapy at the end-of-life.6 Intriguingly, our study showed that carbapenem was the most frequently prescribed antibiotic to patients during the last 14 days of life, with 9.4% of MRAB, 4.2% of MRPA and 3.3% of CRE isolated. Carbapenem use was also an independent predictor of inappropriate antibiotics prescriptions in terminally ill patients. Although we did not analyse the effect of the expression of resistant bacteria related to the use of individual antibiotics, excessive consumption of carbapenem has been an important predisposing factor that contributes to the worsening rates of infections caused by MRAB,22 MRPA,23 and CRE.24 More studies are needed to evaluate the adequacy of carbapenem use in patients during the last 14 days of life.
Notably, only 27.2% of the patients were referred to ID specialists in our study, and a considerable portion of the antibiotic was prescribed inappropriately (62.0%). A German study showed that prospective audit and feedback with ID specialists reduced absolute antimicrobial consumption and the proportion of broad-spectrum antimicrobial use.25 Another study suggested that the ASP was not the sole factor affecting antimicrobial use, but consultation with the ID service also had an impact on the reduction of carbapenem use, leading to favorable outcomes in terms of length of hospital stay and infection-related mortality.23 A study of 459 terminally ill patients in Singapore revealed that cessation of antibiotics after ASP interventions was not associated with an increase in 7-day or 30-day mortality.26 In the study, the ASP team, consisting of clinical pharmacists and ID physicians, audited patients prescribed broad-spectrum intravenous antibiotics, including carbapenem, piperacillin-tazobactam, and fluoroquinolones.26 A comprehensive ASP with additional consultation by ID specialists could be burdensome. However, consultation with an ID specialist in addition to an ASP may be necessary to induce the optimal use of antibiotics in patients during the last 14 days of life.
In our study, inappropriate use of antibiotics was found to be more significant in patients with underlying cancer, underlying cerebrovascular disease, use of carbapenem, and no microbiological testing. Although antimicrobial use is considered inappropriate, symptom relief may be achievable with antimicrobial therapy in terminally ill patients. Clinical evidence showing the effect of antimicrobial agents in the end-of-life period is variable and often inconsistent in relation to symptom relief or increased survival depending on the underlying disease. Among 225 patients with advanced dementia and pneumonia, antimicrobial therapy has been reported to be associated with improved survival but less comfort.15 A Japanese study also showed that only 22.8% of patients achieved symptom relief among 136 patients receiving antimicrobial therapy.2 In contrast, antibiotic treatment decreased discomfort in a previous study including 559 palliative non-cancer patients with pneumonia, even when death was imminent.14 IDSA and SHEA included very limited advice on the use of antibiotics at the end of life of patients, but recommended that antimicrobial agents be withheld if prolonging survival is not a primary goal.11 Further research is needed to investigate the impact of antimicrobial use on comfort achievement at the end of life.
Our study had a few limitations. First, it is difficult to assess whether a patient experiences temporary deterioration due to infection or death. As some patients might have had underlying indications for antimicrobial therapy, it was difficult to determine whether our findings were strictly associated with inappropriate or unnecessary antimicrobial use. Second, detailed patient characteristics in terms of comorbidities were lacking, and assessment of the stage of illness was not performed. The definition of terminal illness may not be clear due to patient characteristics, but this study was conducted for all patients who died during the study because the goal was to investigate the last antibiotic usage pattern irrespective of disease status. Third, the antibiotic usage appropriateness was assessed by physicians at each participating hospital; therefore, there may be differences in this evaluation depending on the evaluator. Additionally, we did not investigate the appropriateness of the dose based on renal function or therapeutic drug monitoring. However, we attempted to overcome these limitations by involving an ID specialist. Fourth, this study is retrospective and epidemiologic in nature and cannot confirm or disprove causality. Finally, our data do not allow us to explore additional factors, including physician perceptions, attitudes, and opinions of patients and family caregivers regarding the decisions about antimicrobial therapy at the end of life. Approximately 30% of physicians intended to continue antimicrobial administration for patients even after this was deemed medically futile, or when comfort was elected as the main goal of care.27
In conclusion, our study showed that excessive quantities of antibiotics, especially carbapenem, were administered to patients with serious chronic or acute illnesses near their end of life. In addition, a high proportion of antibiotics were administered without consulting an ID specialist, with more than half of the antibiotic prescriptions being assessed as inappropriate. Therefore, consultation with an ID specialist, in addition to an ASP, may be necessary to induce the optimal use of antibiotics.
 XML Download
XML Download