

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The coronavirus disease 2019 (COVID-19) has changed the world dramatically. On one hand, time seems to stand still as the radius of activity decreases. Students are out of school, businesses are starting to work remotely, and international travel has declined. Owing to the prolonged COVID-19 outbreak and the popularization of delivery apps, food consumption is also changing significantly. Consumption trends have changed, from eating outside the house to eating at home. Therefore, we hypothesize that the pattern and incidence of enteritis may have also changed.
According to the data released by the Korea Centers for Disease Control and Prevention (KCDC), of the 29,717 fecal samples collected from diarrheal patients over three years from 2016 to 2018, pre-COVID-19, 4,436 (14.9%) were with confirmed pathogens. The confirmed pathogen was pathogenic Escherichia coli in 1,395 cases (31.4%), Salmonella in 1,065 cases (24.0%), and Campylobacter in 391 cases (8.8%).12 In the United States, it is estimated that Campylobacter infections was 19.5 infections per 100,000 persons, 15% of which are hospitalized.3 The mortality rate is reported to be less than 0.1%.4 Although the number of Campylobacter enteritis cases in South Korea is not high, it has shown an increasing trend.5 Recently, there has been a report on changes in gastrointestinal infections after COVID-19 in South Korea based on KCDC data, but there are limitations on the subject and period, and analysis by age has not been performed.5 The purpose of this study was to evaluate the change in the trend of enteritis before COVID-19 (2016–2019) and at the present time of COVID-19 in South Korea by age, sex, and region, focusing on Campylobacter.
METHODS
Health Insurance Review and Assessment (HIRA) database
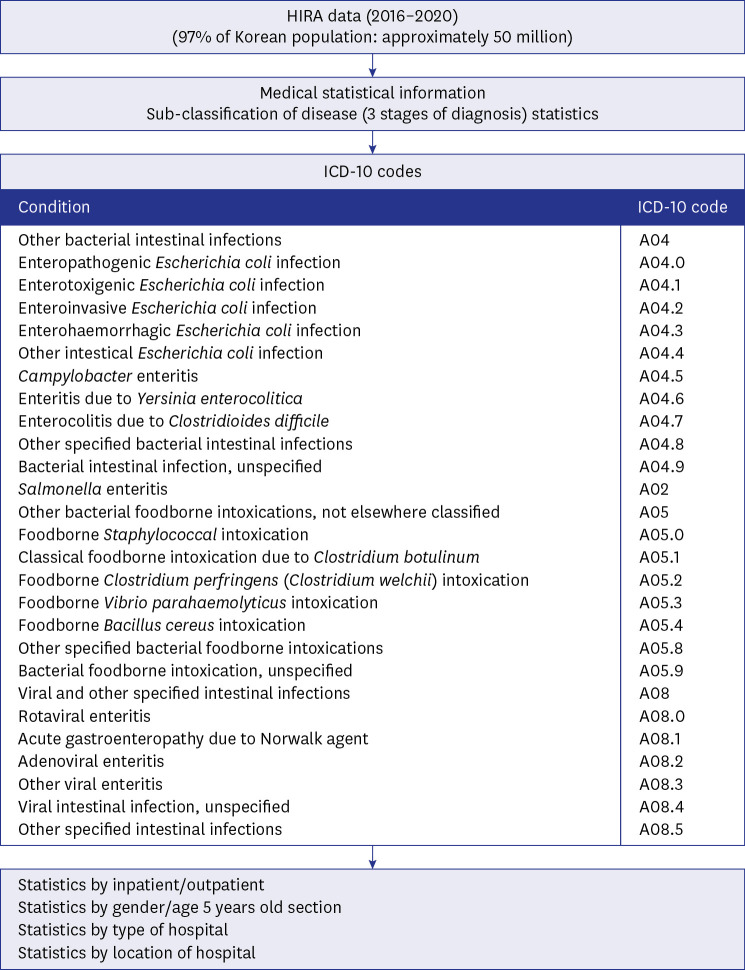
We used the HIRA database with data collected from 2016 to 2020. HIRA is a government agency that oversees all health services in Korea. In Korea, there is the National Health Insurance Program that is universally applicable to the population. The HIRA service covers 97.0% of the Korean population (approximately 50 million). The remaining 3% of the population is covered by the Medical Assistance Program. Almost all Koreans were of Korean descent. HIRA disease statistics were collected based on the hospital and pharmacy medical costs. We used the online public database provided by HIRA to show the number of patients with specific diseases each year from 2016 to 2020 according to diagnosis (International Classification of Diseases [ICD] code), age group, and sex (Fig. 1). Gastroenteritis diagnosis is based on a physician-certified diagnosis using ICD-10 codes, consisting of other bacterial intestinal infections (A04), enteropathogenic E. coli infection (A04.0), enterotoxigenic E. coli infection (A04.1), enteroinvasive E. coli infection (A04.2), enterohaemorrhagic E. coli infection (A04.3), other intestinal E. coli infection (A04.4), Campylobacter enteritis (A04.5), enteritis due to Yersinia enterocolitica (A04.6), enterocolitis due to Clostridioides difficile (A04.7), other specified bacterial intestinal infections (A04.8), bacterial intestinal infection, unspecified (A04.9), Salmonella enteritis (A02.0), other bacterial foodborne intoxications not elsewhere classified (A05), foodborne Staphylococcal intoxication (A05.0), classical foodborne intoxication due to Clostridium botulinum (A05.1), foodborne Clostridium perfringens (Clostridium welchii) intoxication (A05.2), foodborne Vibrio parahaemolyticus intoxication (A05.3), foodborne Bacillus cereus intoxication (A05.4), other specified bacterial foodborne intoxications (A05.8), bacterial foodborne intoxication, unspecified (A05.9), viral and other specified intestinal infections (A08), rotaviral enteritis (A08.0), acute gastroenteropathy due to Norwalk agent (A08.1), adenoviral enteritis (A08.2), other viral enteritis (A08.3), viral intestinal infection, unspecified (A08.4), other specified intestinal infections (A08.5).
Definition of bacterial enteritis in HIRA
Among the ICD-10 codes, bacterial intestinal infection was defined as “A04 + A020 + A05 − A04.7”, and viral intestinal infection was defined as “A08.”
Among bacterial intestinal infection, A04.7 was excluded because it was a nosocomial infection and was not suitable for the results covered in this study.
Definition of viral enteritis in HIRA
Viral enteritis was defined as viral and other specified intestinal infection (A08).
Prevalence of enteritis
Prevalence was calculated as the number of patients in a specific year divided by the population in a specific year. The population on resident registration was used for the population in a specific year, and data were obtained from the KOrean Statistical Information Service (KOSIS).
Age and male-to-female ratio of Campylobacter enteritis
To compare with the population classification of previous studies, we classified age groups as < 5, 5–9, 10–14, 15–44, 45–64, ≥ 65. In addition, the male-to-female ratio was determined according to populational statistics in the corresponding year.
Regional classification
The total number of administrative districts in Korea is 17, consisting of seven large cities, including one capital and six metropolitan areas, as well as ten local provinces. Seven cities were classified as urban areas, and the other regions made up of 10 local provinces were classified as rural areas.
Characteristics of Campylobacter enteritis
The prevalence in each age group was compared to the prevalence in the ‘five years and younger’ group. In the sex comparison, the prevalence was compared to that of males. In the regional comparison, prevalence was compared to that of urban areas.
Mean length of stay
The mean length of stay was calculated as the total length of stay in a specific year divided by the number of patients in a specific year. The patients were classified by inpatients and outpatients.
Statistical analysis
The ratio analysis of viral enteritis and bacterial enteritis is presented as mean and standard deviation with 95% confidence interval under the assumption of a normal distribution. The decrease in the prevalence of viral enteritis with increasing age was analyzed using analysis of variance (ANOVA), and Levene statistics were used for homogeneity of variances. Prevalence is presented as the number per 100,000. An independent samples t-test was used to compare the numbers of enteritis cases, and a Mann-Whitney U test was used to compare the rate of change in the number of patients compared to the previous year. An ANOVA test was conducted when the categories were above two. Statistical analyses were performed using SPSS for Windows (version 19.0; IBM Co., Armonk, NY, USA). Statistical significance was considered to exist when the P value was less than 0.05.
RESULTS
Epidemiology of bacterial and viral enteritis
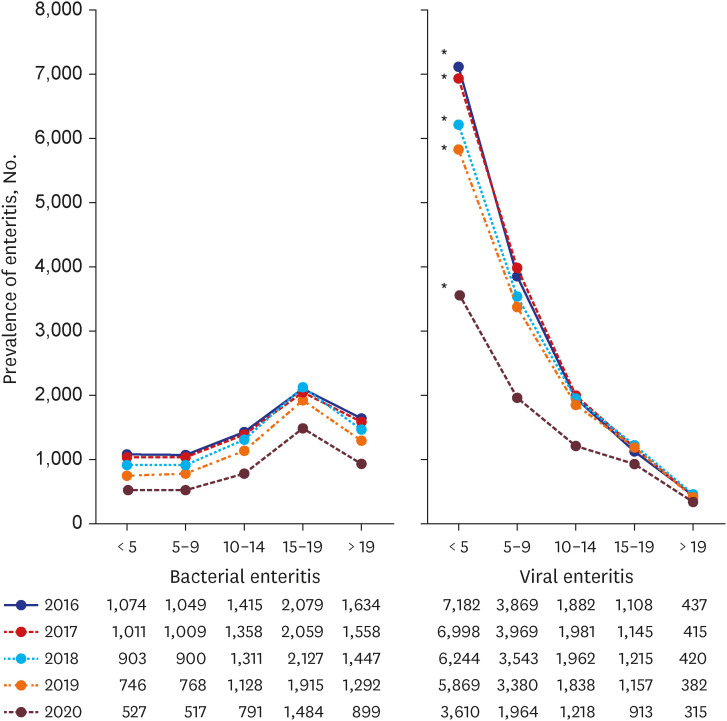
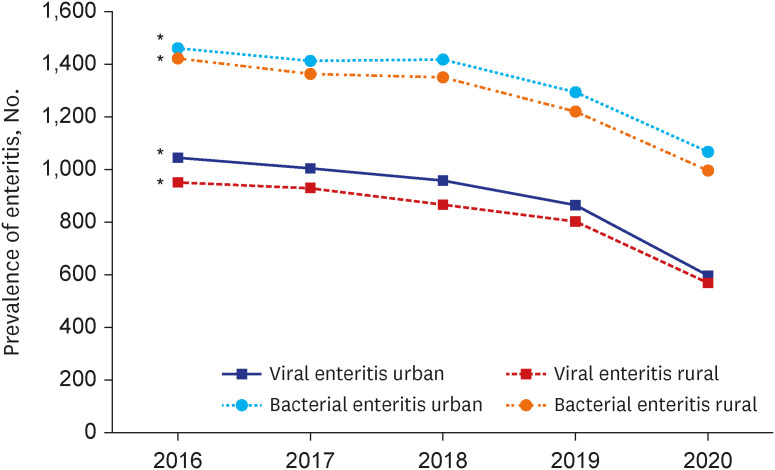
In all age groups, from 2016 to 2020, both bacterial and viral enteritis decreased (P < 0.001) (Fig. 2, Supplementary Fig. 1). The rate of decrease in viral enteritis was higher than that in bacterial enteritis in 2020. In the age group under 5 years, viral enteritis was reported 7.048 + 0.468 times more than that of bacterial enteritis (Fig. 2). The prevalence of viral enteritis decreased with increasing age (P < 0.001). Bacterial enteritis peaks at the age of 15–19 years, and a higher prevalence has been reported in adults than in children under 15 years of age.
Fig. 2
Annual prevalence of bacterial and viral enteritis by age group from 2016 to 2020.
*P < 0.001.
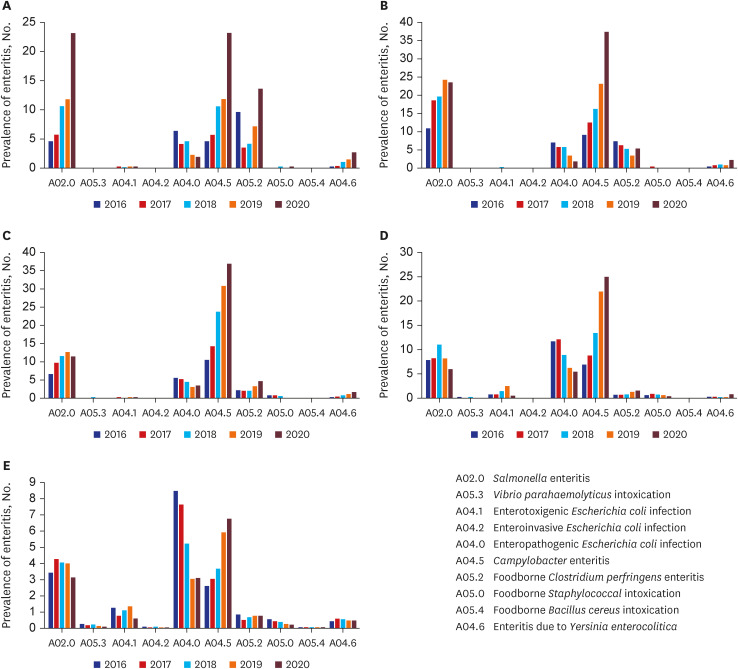
Campylobacter was the most common cause of bacterial enteritis in all the age groups from 2016 to 2020 (Supplementary Table 1). In the age group under 5 years, the prevalence of Salmonella enteritis (A02.0), Campylobacter enteritis (A04.5), and Clostridium perfringens enteritis (A05.2) was particularly prominent in 2020 (after COVID-19) (Fig. 3). The increase in the prevalence of Campylobacter enteritis (A04.5) in 2020 was also noticeable in the age group of 5–9 years. Although the rate of increase is decreasing, the only bacterial enteritis that has increased in 2020 is Campylobacter enteritis, which was also seen among 10–14 year old, 14–19 year old, and over 19 year old patients (adults) (Fig. 3). The prevalence of viral and bacterial enteritis was higher in the urban areas than in the rural areas (P < 0.001) (Fig. 4). In the case of viral enteritis, the gap in prevalence between urban and rural areas has decreased. In the case of bacterial enteritis, there was little change in prevalence between urban and rural areas.
Epidemiology of Campylobacter enteritis
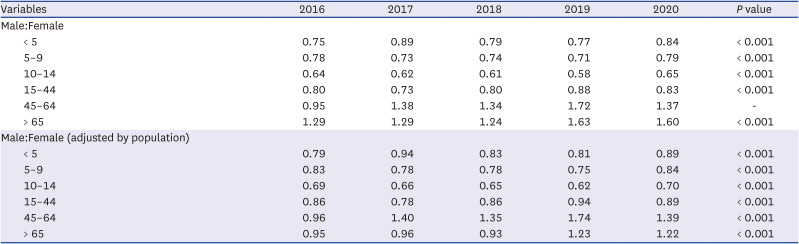
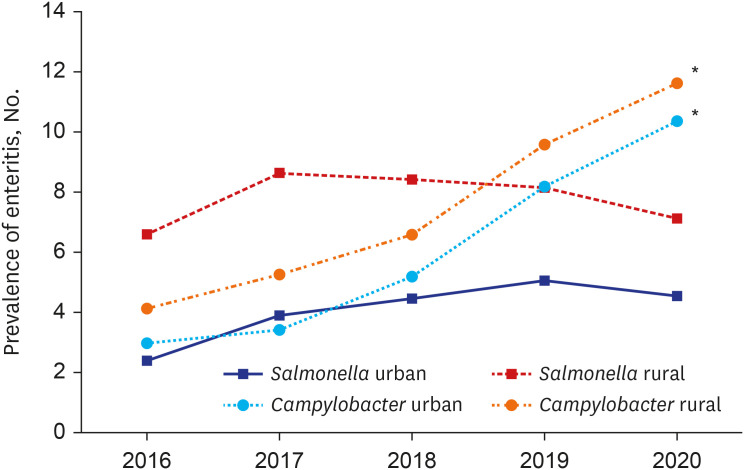
Campylobacter enteritis had the highest prevalence among 10–14 years of age. Its prevalence is low in adults. Campylobacter enteritis was more common in men than in women of all ages and more common in all age groups in the rural areas. Since 2017, the gap in the prevalence of Campylobacter enteritis between urban and rural areas has been decreasing (Table 1). The sex ratio of the Campylobacter prevalence rate was higher in men under the age of 44. However, after the age of 45, the pattern was predominantly female (except 2016 for those aged 45–65 and except 2016, 2017, and 2018 for those aged 65 and over) (Table 2). Since 2016, bacterial enteritis has been prevalent in urban areas. However, Campylobacter enteritis, a bacterial enteritis, has always shown a higher prevalence in rural areas (P < 0.001) (Fig. 5). The same trend was observed after the COVID-19 outbreak. Another type of bacterial enteritis, Salmonella enteritis, also had a higher prevalence in rural areas. However, unlike Campylobacter enteritis, Salmonella enteritis has decreased in incidence since the onset of COVID-19 (Fig. 5).
Table 1
Characteristics of Campylobacter enteritis from 2016 to 2020
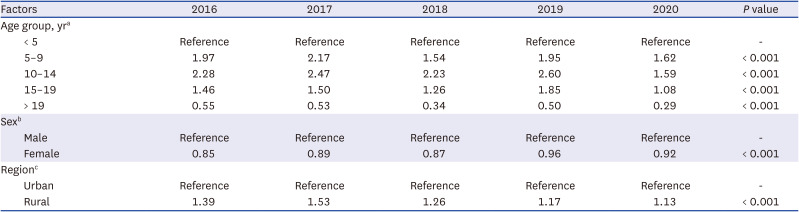
Table 2
Male-to-female ratio of Campylobacter enteritis from 2016 to 2020
Clinical severity of bacterial and viral enteritis
In bacterial enteritis (including Campylobacter enteritis, Salmonella enteritis, etc.), the mean length of stay has been increasing with each passing year (both inpatients and outpatients). After COVID-19, the growth rate was even higher (P < 0.05) (Supplementary Fig. 2). There was a difference in length of stay due to bacterial enteritis between men and women.
Patients with viral enteritis had the same or a decreased mean length of stay. The mean length of stay of both inpatients and outpatients decreased (P < 0.05) (Supplementary Fig. 3). Additionally, there was almost no gender difference in the length of stay for viral enteritis.
The mean length of hospital stay for patients with Campylobacter enteritis has increased (Supplementary Table 2). However, no significant changes were observed in outpatients. On the other hand, mean length of stay due to Salmonella enteritis, which was higher than that of Campylobacter enteritis, was on the decline (Supplementary Table 3).
For inpatients, the gap between females and males showed a positive value in the case of bacterial enteritis (female > male) and showed the same pattern in Campylobacter enteritis. The difference in the number of patients did not increase after the COVID-19 outbreak (Supplementary Table 4).
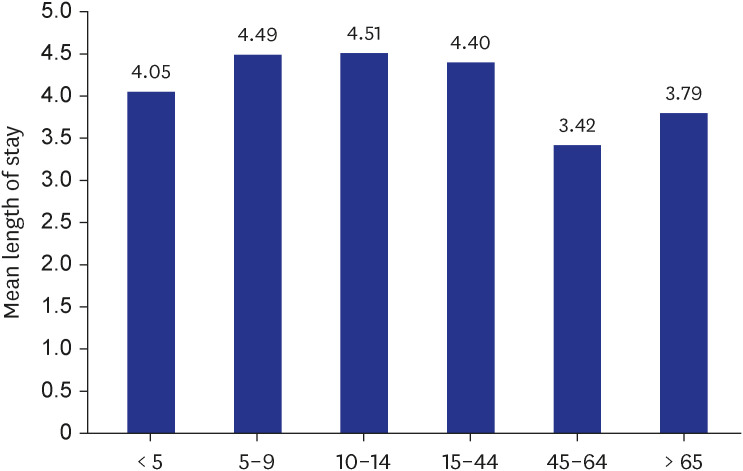
The longest mean length of stay for Campylobacter enteritis was in the 10–14 years age group, followed by the 5–9 years age group and the 15–44 years age group (Fig. 6). The 45–64 years age group showed the shortest progress. The mean length of stay for Campylobacter enteritis was longer in children and adolescents than in adults.
DISCUSSION
The current study analyzed the HIRA data for gastroenteritis in South Korea from 2016 to 2020. The number of patients with gastroenteritis has decreased annually. In particular, the absolute value of the rate of change in the number of patients with gastroenteritis increased dramatically during the COVID-19 epidemic. This phenomenon was also detected in other studies, which have reported a sharp decrease in acute gastroenteritis has been reported worldwide after COVID-19.567891011 In other words, measures such as social distancing, barrier, and hand hygiene can reduce direct person-to-person transmission as well as transmission by contaminated surfaces. This will affect the propagation of the causative agent of gastroenteritis. In detail, viral enteritis, which is common in children, has been decreasing over the years and is even more pronouncedly low in 2020. This is aligned with other results from South Korea (2013–2019, data from national surveillance network [EnterNet], 64.7% reduction in the number of virus sample reports12 and March 2018–February 2021, data from Korea Disease Control and Prevention Agency [KDCPA], 31.9% virus sample reports reduction5) and from the United States (2005–2014, data from national surveillance network [FoodNet], 27.0% reduction in monthly prevalence13). Compared with previous studies in South Korea, the period of this study was from 2016 to 2020, which is extensive and reflects the latest trends. When comparing our data to that of the KDCPA data or EnterNet, we evaluated the prevalence by applying the national age-specific gender population.
The incidence of Campylobacter enteritis is increasing. This is aligned with the results from the United States (1998–2016, data from the CDC Food Tool website)14 and Australia (1998–2013, using national surveillance data).15 Even after the outbreak of COVID-19, the incidence of Campylobacter enteritis has increased. Campylobacter is a mainly foodborne pathogen, particularly in uncooked poultry products.16
Campylobacter was isolated from over 40% of retail chickens examined, and 65% of human Campylobacter enteritis of known etiology has occurred due to chickens.17 According to a survey of 1,500 people for two weeks in September 2021 by the Rural Development Administration, after COVID-19, 12.1% of consumers ate chicken three or more times a week, 1–2 to times a week (43%), to 1–2 times a month (34.9%), and once every 3 months (less was 10%).18 In addition, ‘home cooking’ constituted 44% of the instances of chicken consumption, ‘delivery’ 30.3%, ‘home-convenient meal/baro-cooking set’ 13.2%, and ‘dining out’ 12.6%, indicating that the proportion of delivery consumption was higher than that of other livestock breeds. In a survey of 549 Korean adults for one week in October 2020, overall, respondents said that take-out and delivery services after the COVID-19 outbreak were “the same as before COVID-19 (delivery = 40.1%, take-out = 37.9%).19 However, the combined ratio of those who responded that ‘do it more after COVID-19,’ ‘started doing it after COVID-19’ was 42.3% for take-out and 39.0% for delivery, which was more than those who answered the same as before COVID-19. The reason for this situation is that government-mandated lockdown and stay-at-home orders significantly accelerated the demand for food delivery.202122 In addition, consumers purchased more fried chicken (65.3%) and pizza or burgers (50.4%) after COVID-19.19 Furthermore, purchases through the internet have increased pointedly, by 49.8%.18 In this situation, it is possible that food hygiene management has not been properly performed as compared to the time period preceding the pandemic. In other words, as more people order food for delivery and consumers cannot directly check the hygiene status and cooking process of the company due to the nature of delivery food, there is a possibility of using ingredients or foods for which the expiration date or sanitary conditions are not certain.
In this study, the prevalence of Campylobacter enteritis was highest in the 10–14 years old group over the years from 2016 to 2020, and highest in the 5–9 years old group in 2020. This was different from the results seen in the Australian study (age distribution was tri-modal, highest in < 5 years old, follow by 20–40 year old and over 65 year old)15 and other studies (age distribution was bimodal, highest in < 5 years old, follow by 15–45 years old).2324 However, the prevalence in the children was similar. In addition, despite the decrease in the overall prevalence of bacterial enteritis, the prevalence of Campylobacter enteritis is increasing among all age groups, and it is thought to be important in terms of health hygiene and disease management, especially in those under five years of age, which show the highest increase rate. This result is thought to be due to changes in disease epidemiology according to the westernization of lifestyle.2526
The incidence of Campylobacter enteritis has been reported to be higher in males. This was consistent with the results reported by Green et al.27 However, in this study, analysis by age group showed that Campylobacter enteritis was higher in women over 45 years of age. This is a different result from the Western seven-country data meta-analysis. Racial and genetic differences may be the reason for this, as well as hormonal changes, such as menopause, in women over the age of 45.28
The risk of Campylobacter enteritis was 1.23-fold higher in rural areas than in urban areas. This result is similar to that of a Canadian study (2005–2007, 1.89-fold higher in rural areas)17 but different from a Scottish study (1978–1982, 1.07-fold higher in urban areas).29 These differences are presumed to be due to geographical and weather differences.3031
The number of patients with viral enteritis has been decreasing, and the mean length of hospital stay has been decreasing or maintaining the same duration. The marked decrease in viral enteritis since COVID-19 is consistent with reports of a significant decrease in hospital visits for mild illnesses.32 However, the number of patients with bacterial enteritis and the mean length of stay have both been increasing. This phenomenon seems to be related to reports of increased antibiotic resistance in bacterial enteritis.33 The mean length of stay for Salmonella enteritis decreased with each passing year, but the mean length of stay for Campylobacter enteritis increased. In this regard, Guillain-Barré syndrome can develop in patients with Campylobacter infection, which can also lead to myocarditis.34 Furthermore, reports of antibiotic-resistance in bacteria are on the rise; therefore, the increase in the number of patients with Campylobacter, as well as the increase in the mean length of stay, which reflects the severity, is a major medical problem.35
Campylobacter enteritis appears to be more severe in vulnerable subjects, with a longer mean length of stay reported in female, pediatric, and adolescent patients. This also needs to be addressed.
Nevertheless, since HIRA data uses the disease code as per the doctor’s diagnosis, there is a chance of missing the actual pathogen or even misdiagnosis. This is a common problem in studies using ICD-19 codes.36 To evaluate the post-COVID-19 trend, there is a limitation that, for now, only data for 2020 can be viewed, and data for 2021 cannot be evaluated.
In conclusion, although bacterial and viral enteritis have decreased in COVID-19, we confirmed that Campylobacter enteritis has increased in all age groups and rural areas compared to urban areas. Recognizing that the trend of Campylobacter enteritis before and after COVID-19 is changing may be helpful for public health measures and food hygiene guidelines. Long-term follow-up studies of epidemiological changes in Campylobacter enteritis after COVID-19 are needed.
 XML Download
XML Download