

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Meningiomas are the most common primary intracranial tumors in adults, accounting for about 36% [1]. Most meningiomas are benign, and have favorable outcomes with treatment using “wait and scan” or “stereotactic radiosurgery,” or “surgical resection” [2]. Anaplastic meningioma (World Health Organization [WHO] grade 3) consists of 1%–2% of all meningiomas and presents a particularly aggressive clinical course and a poor survival outcome [234567]. In United States, population based study showed 5-year survival rate of patients with anaplastic meningiomas was 41.4% and factors associated with increased risk of death were older age, high comorbidity score, and subtotal resection [1]. According to the study from Korea Central Cancer Registry, in patients with anaplastic meningioma, 1-year, 2-year, and 5-year relative survival rates were 89.2%, 79.4%, and 68.9%, respectively [8].
The prognostic factors in patients with anaplastic meningioma are unclear and controversial. Several retrospective studies have reported the importance of gross total resection (GTR) and its association with better survival outcomes. There has been a consensus in the literature that adjuvant irradiation is essential regardless of the extent of resection in patients with anaplastic meningioma [57910]. However, due to the rarity of the anaplastic meningioma itself, there are few studies that have proven its prognostic value statistically [23461011].
The purpose of the present study was to analyze the prognostic factors influencing survival outcomes. Moreover, we analyzed the progression patterns in patients with anaplastic meningioma and determine the clinical efficacy of stereotactic radiosurgery and chemotherapy after the recurrence of anaplastic meningioma. To our knowledge, this study involved largest cohort of anaplastic meningioma among the clinical studies from a single institute. In this regard, we expected that this study can deliver a practical nuance to the multi-disciplinary team involved neuro-oncology beyond the statistical results in this rare tumor.
MATERIALS AND METHODS
This retrospective study was approved by the Institutional Review Board of Asan Medical Center (IRB no. 2021-0487). The need for informed consent was waived due to the retrospective nature of the study. Based on prospectively collected adult brain tumor database, 76 consecutive patients were diagnosed with malignant meningioma or anaplastic meningioma after surgical resection from 1995 to 2020. Among these patients, a total of 48 patients were enrolled in this study; we excluded 18 patients who did not meet the criteria of 2016 WHO classification for anaplastic meningioma, 5 patients without available clinical radiological data, 3 patients with a follow-up duration shorter than 12 months, one patient with intracranial metastasis of spinal meningioma, and one patient with neurofibromatosis.
Prior to 2000, WHO classification had ambiguous criteria for grading meningioma. Based on the studies from Mayo Clinic published in the late 1990s [12], the 2000 WHO classification presented a more objective criteria in meningioma grading [13]. And for WHO grade 3 meningioma, the revised 4th edition of WHO classification still applies this criteria as it is [1415]. The biggest part that changed the diagnostic criteria for anaplastic or malignant meningioma around 2000 is the brain invasion. Brain invasion was considered as a solid criterion for malignant meningioma before 2000, but current WHO criteria for anaplastic meningioma excludes brain invasion. According to the diagnostic criteria for anaplastic meningioma in the 2000s, 18 cases diagnosed with malignant meningioma by brain invasion before 2000 were excluded from this study. In 2022, the 5th edition of the WHO classification of central nervous system tumors was published. According to this, it is emphasized that the criteria defining anaplastic meningioma should be applied regardless of the underlying subtype. And, several molecular biomarkers are also associated with classification and grading of meningioma [1617]. In this study, there were two cases of rhabdoid subtype and none of the papillary subtype. In the two cases diagnosed as rhabdoid subtypes, mitotic indices were 12 and 9 per 10 high-power field, respectively, and were included in this study. Evaluation for TERT promoter mutation, homozygous deletion of CDKN2A/B and H3K-27me3 loss of nuclear expression were not carried routinely in the patients included in this study.
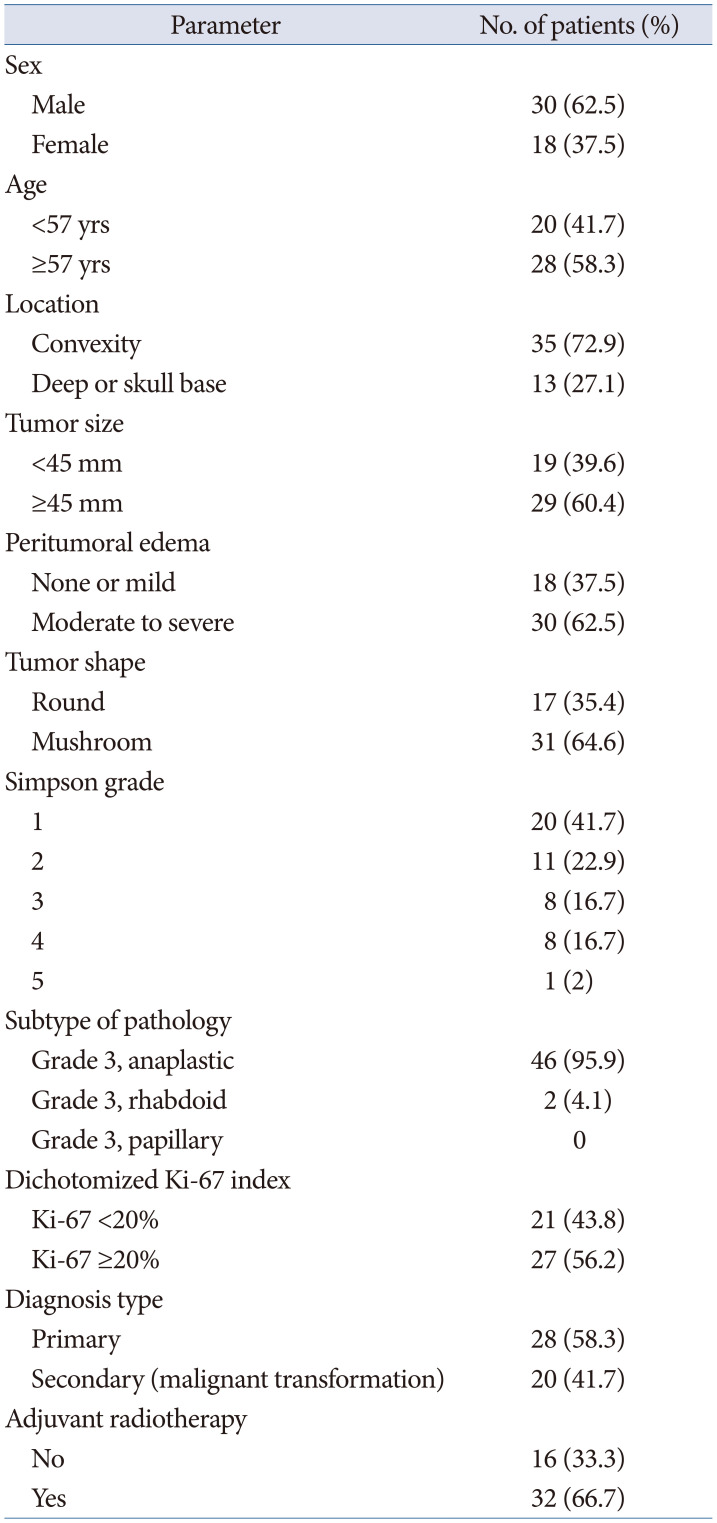
Baseline characteristics of clinico-radiologic data were retrospectively collected and are summarized in Table 1. The mean and median follow-up durations were 42 months and 30 months, respectively (range, 4–140 months). Thirty patients (62.5%) were male and 18 (37.5%) were female, with a median age of 57 years (range, 32–77 years). Twenty-eight patients (58.3%) were initially diagnosed with anaplastic meningioma and 20 (41.7%) were secondary anaplastic meningioma from atypical or benign meningioma. We analyzed radiologic data in the following way: location (superficial location vs. deep location), tumor size (<45 mm vs. ≥45 mm), peri-tumoral edema (none or mild vs. moderate to severe), tumor shape (round vs. mushroom). The locations of tumors were divided into superficial location (including convexity and parasagittal location) and deep location (including falcine, skull base, and intraventricular location). Tumor size was defined as the largest tumor diameter on gadolinium-enhanced T1-weighted MRI. Peri-tumoral edema was estimated by the longest distance from the margin of the tumor on fluid-attenuated inversion recovery images or T2 weighted images. The edema index (EI) was defined as the ratio of edema diameter to tumor diameter. The grading of edema severity according to EI was performed as follows: no edema or negligible edema (EI<0.1); mild edema (0.1<EI<1.0); moderate edema (1.0<EI<2.0); severe edema (EI>2), and then the patients were divided into two groups: one with minimal to mild edema (EI<1.0) and the other with moderate to severe edema (EI>1.0) [18]. The shape of the tumor was classified as one of round and mushroom shape. Mushroom-shaped tumors were defined as having a prominent pannus extending over the cerebral surface from the globoid portion of the tumor [19]. The degree of resection was preferentially determined by a review of postoperative and follow-up MRI studies or CT scanning. GTR was defined when no residual tumor was seen on contrast T1-weighted or T2-weighted images or on contrast CT images; otherwise, cases were defined as a subtotal resection. The Simpson grading scale which considered the gold standard for defining the surgical extent of resection was collected through surgical records and was dichotomized for statistical analysis (Simpson grade 1 or 2 vs. Simpson grade 3 or 4 or 5).
Statistical analysis
Statistical analyses were performed with the Statistical Package for the Social Sciences version 21.0 (IBM Corp., Armonk, NY, USA). The means of numeric variables and the distributions of categorical variables between subgroups were compared with independent-samples t-tests and χ2 test, respectively. Progression-free survival (PFS) was calculated from the date of initial surgery diagnosed as anaplastic or malignant meningioma to the date of recurrence, progression, death or last radiologic follow-up, whereas overall survival (OS) was calculated from the date of surgery to the date of death. Data for patients who were alive were classified as censored at the time of the last follow-up. PFS and OS were analyzed by Kaplan-Meier curves, and comparisons between groups were performed using the log-rank tests. A Cox proportional hazards model was used to adjust for covariates which showed p<0.2 on univariate test. Simpson grade contains subjective elements based on the intraoperative visual assessment, so we included only extent of resection based on the postoperative image in the multivariate analysis.
RESULTS
Treatment summary
GTR was performed in 36 patients (75.0%) and Simpson grade 1 or 2 resection was achieved 31 patients (64.6%). Thirty-two patients (66.7%) received external beam radiation as an adjuvant therapy after tumor resection with confirmed WHO grade 3 meningioma. Of the 28 patients diagnosed with primary anaplastic meningioma, 26 patients (92.8%) received adjuvant radiotherapy. In patients with secondary anaplastic meningioma, only 30% of patients (6 patients out of 20) received adjuvant radiotherapy. Adjuvant chemotherapy was performed in two patients with secondary anaplastic meningioma.
Analysis of survival
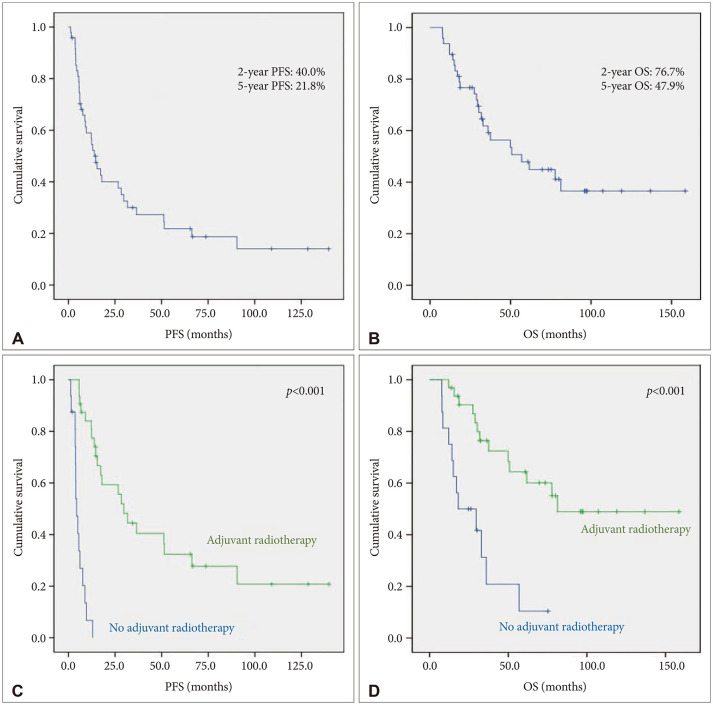
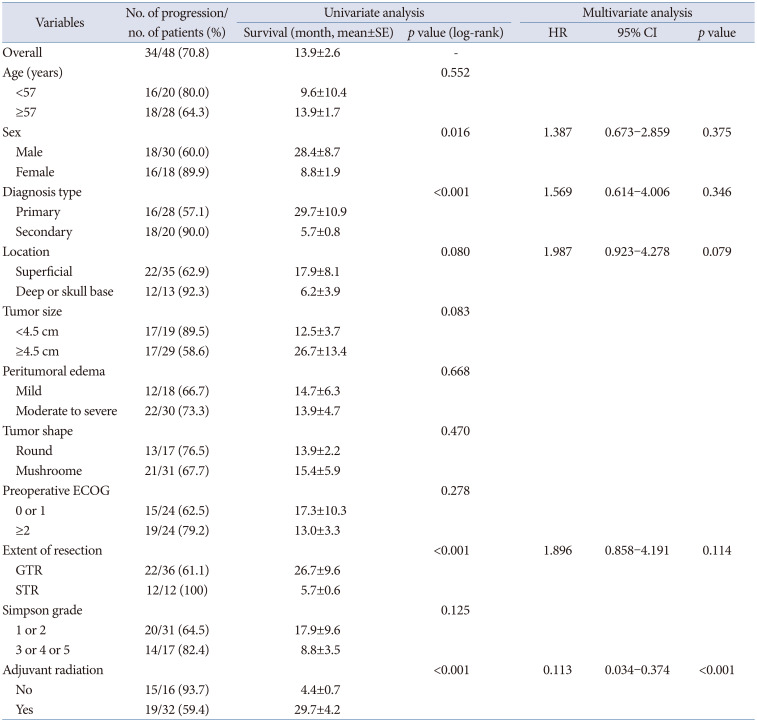
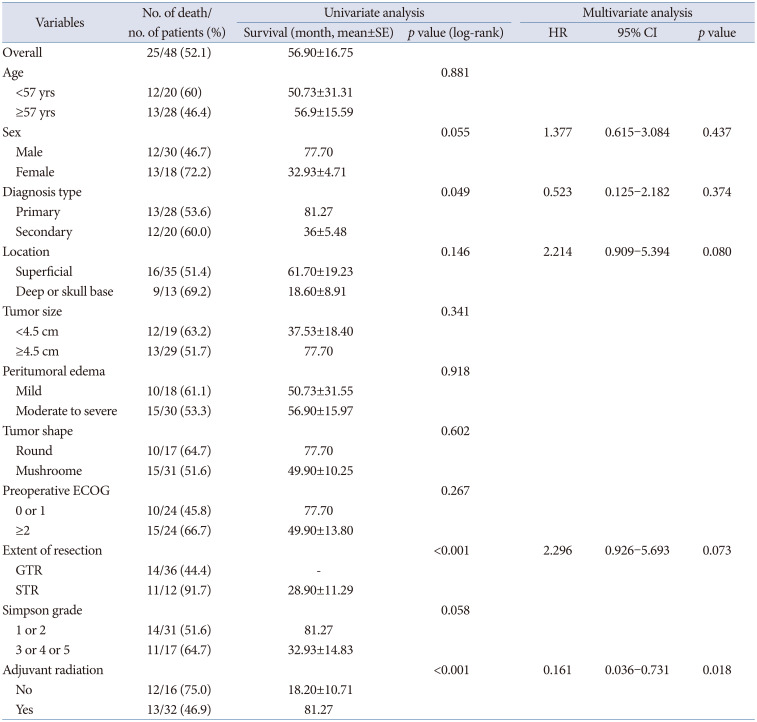
In terms of PFS rates, we analyzed the correlation between risk factors and survival rate (Table 2). The median PFS of the entire population was 13.9 months (95% confidence interval [CI]=8.8 through 19.1). Estimated PFS rates at 1, 2, 5, and 10 years were 59.0%, 40.0%, 21.8%, and 20.8%, respectively (Fig. 1). Male, primary anaplastic meningioma, GTR, and adjuvant radiotherapy were associated with longer PFS upon univariate analysis . However, as seen in Table 2, adjuvant radiotherapy (p<0.001, hazard ratio [HR] 0.113, 95% CI=0.034–0.374) was shown to be only prognostic factor for a better PFS in the multivariate analysis. On the other hand, superficial tumor location (p=0.079) and GTR (p=0.114) failed to show significance in a multivariate analysis.
Twenty-five patients (52.1%) died during the follow-up period. The median OS of the entire population was 56.9 months (95% CI=24.1–89.7). Estimated OS rates at 1, 2, 5, and 10 years were 93.8%, 76.7%, 47.9%, and 36.6%, respectively. On univariate analysis, primary anaplastic meningioma, GTR, and adjuvant radiotherapy were found to be variables associated with a longer OS (Table 3). On multivariate analysis, adjuvant radiotherapy (p<0.001, HR 0.161, 95% CI=0.036–0.731) was the only variable found to be associated with a longer OS.
Progression pattern and salvage treatment
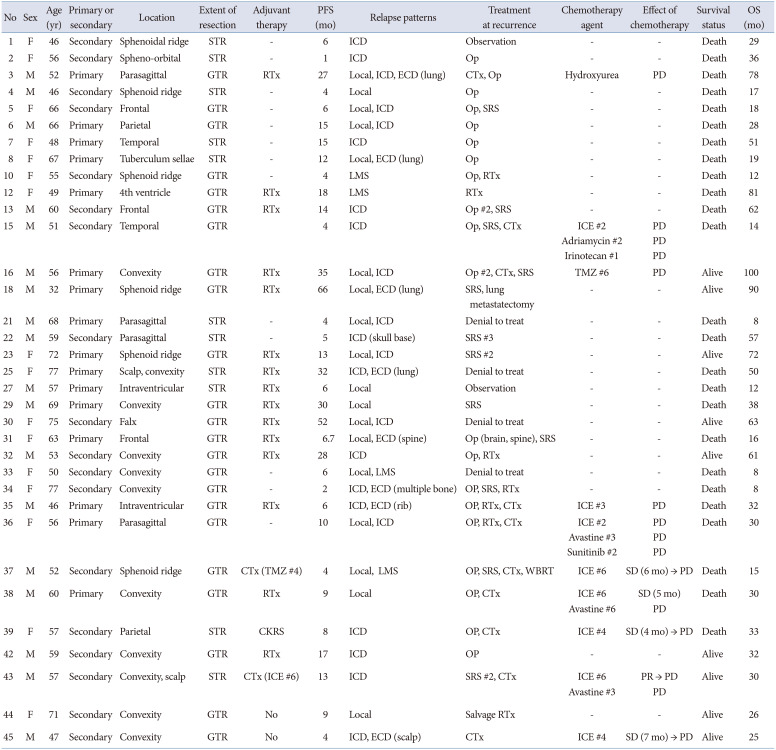
Disease progression patterns and salvage treatments at progression in all patients were summarized in Table 4. Disease progression occurred in 34 patients (70.8%). Extra-cranial dissemination was in 8 patients. Common sites for extra-cranial metastasis were lung (in 4 patients) and bone (in 3 patients). Intra-cranial dissemination was in 26 patients and leptomeningeal seeding in 4 patients.
After disease progression was confirmed, surgical resection was performed in 20 patients, and salvage radiotherapy was performed in 9 patients. Chemotherapy was performed in 9 patients. Stereotactic radiosurgery (SRS) was performed 23 times in 16 patients. Six patients received conservative care due to a poor performance status or unwillingness to undergo treatment.
Response to salvage treatment
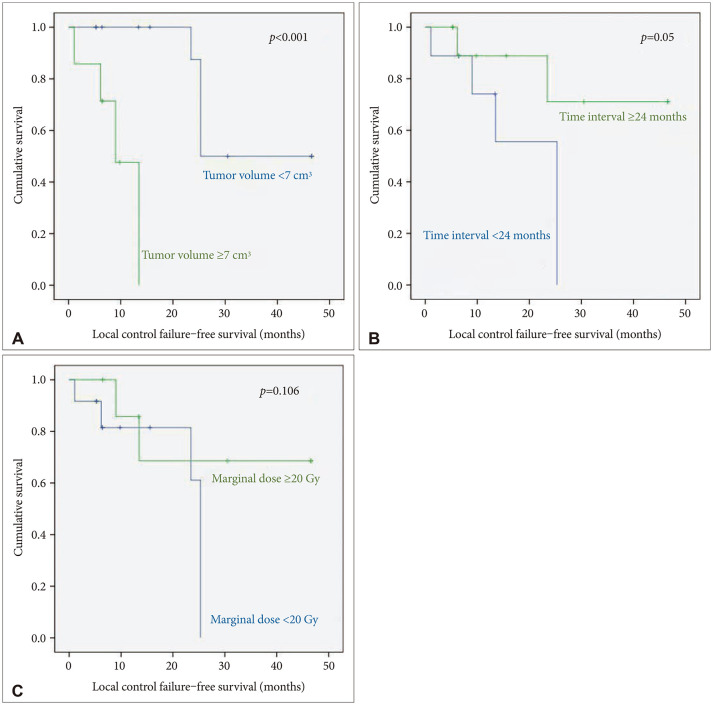
SRS using Gamma Knife was performed 12 times, and SRS using CyberKnife was performed 11 times. Tumor local control and distant failure were analyzed for 20 target lesions in 13 patients with follow-up brain MR images. The 1- and 2-year local control rates were 74.3% and 65%, respectively. In univariate analysis, small tumor volume (less than 7 cm3) and the longer interval between the diagnosis of anaplastic meningioma and SRS (more than 2 years) were found to be positive prognostic factors for local tumor control. However, in the multivariate analysis, no significant prognostic factors could be found due to the small sample size (Fig. 2). Distant failure occurred in 9 patients (69.2%) and the median time to distant failure was 5 months (range, 1–14 months).
Salvage chemotherapy were used in 10 patients, and a total of 6 chemotherapeutic agent were used. Ifosfamide, carboplatin, etoposide (ICE) was used in 8 patients. Bevacizumab was used in three patients, and hydroxyurea, temozolomide, adriamycin, irinotecan, and sunitinib were used once each (Table 4). The only chemotherapeutic agent which showed a clinical effect was ICE, but the effect was marginal. In 8 patients treated with ICE, partial response was in one and stable diseases in 4 patients, but there was no effect in the remaining 3 patients. Unfortunately, all other chemotherapeutic agents were not effective in our cohort. In all 3 patients using bevacizumab, bevacizumab did not prevent disease progression.
DISCUSSION
Anaplastic meningioma is very rare and is generally known to have a poor prognosis [111720]. In a study of 755 patients from an US national database, the 5-year OS rate in patients with anaplastic meningioma was 41.4% [11]. Our study showed a 5-year OS rate was 47.9%, similar to that from US national cancer database. However, due to its rarity, there are very few reports in the literature on the progression pattern and the response to treatment about anaplastic meningioma. Although many studies have been conducted by combining anaplastic meningioma and atypical meningioma, the clinical pattern and the response to treatment of anaplastic meningioma is clearly different from that of atypical meningioma. Our study included the largest number of patients among the articles that studied only anaplastic meningioma from a single institution. In this study, 28 patients with primary anaplastic meningioma and 20 patients with secondary anaplastic meningioma were analyzed, so the characteristics of each group could be well understood. In addition, since most patients were treated aggressively as possible as clinically permitted, the response to salvage therapeutic arms could be observed well.
Extent of resection is associated with prognosis of patients with all WHO grades of meningioma [510212223]. However, the statistical evidence for the positive effect of GTR on the prognosis in patient with anaplastic meningioma has been controversial because of the rarity of the tumors. We found that GTR was associated with significant better PFS and OS (p<0.001, p<0.001) in univariate analysis. However, multivariate analysis failed to prove the association with PFS and OS (p=0.114, p=0.073). Although our results do not ignore the positive effects of GTR on prognosis, it means that the importance of adjuvant therapy is relatively more emphasized in anaplastic meningioma compared with WHO grade 2 meningiomas.
The use of adjuvant radiotherapy after the surgical resection of anaplastic meningiomas is essential to their treatment [5112425]. In most of the reported series, there is a consensus that patients with anaplastic meningiomas should be treated with adjuvant radiotherapy irrespective of the extent of resection. Our findings are also consistent with those of other studies. In our multivariate analysis, adjuvant radiotherapy was found to be the only prognostic factors affecting PFS and OS (p<0.001, p=0.018). In our study, patients with secondary anaplastic meningiomas seems to have poor PFS and OS (p<0.001, p=0.049) in univariate analysis, but in multivariate analysis, diagnosis type did not affect to PFS and OS (p=0.346, p=0.374). Other groups have reported a better prognosis in patients with primary anaplastic meningioma because of the predominance of superficial location and surgical advantage for GTR [212326]. In our study, there were more incidence of superficial location (75% vs. 70%, p=0.750) and more achieved GTR cases (82.1% vs. 65%, p=0.155) in primary anaplastic glioma, but there was no statistical difference. We postulated that the cause of our statistical result was that the proportion of patients who received radiotherapy was significantly higher in primary anaplastic meningioma than in secondary anaplastic meningioma (92.8% vs. 30%, p<0.001).
There is debate about the prognosis according to sex. Cain et al. [27] reported that 3-year OS was 31% higher for women than for men, on the contrary, that the female recurrence rates were 2 times higher than the male recurrence rates [21]. In our univariate study, the poor prognosis in females may be attributed to the high rate (55.6%) of secondary anaplastic meningioma and low proportion (50%) of adjuvant radiotherapy. In multivariate analysis, sex was not a prognostic factor. It is widely known that specific radiographic findings are related to histologic grade in meningioma: tumor size [2829]; tumor location [2830]; peri-tumoral edema [283132]; irregularities in the shape of meningiomas such as “mushroom” [3334]; presence of tumor heterogeneity such as necrosis, cystic degeneration, and hemorrhage [283536]. However, our study results showed that radiological findings were not related to prognosis in anaplastic meningioma.
A significant number of patients with anaplastic meningiomas will eventually relapse despite appropriate treatment. A considerable proportion of relapsed patients had intracranial dissemination (76.4%), and leptomeningeal seeding was also present in 11.7% of relapsed patients. Therefore, it is common to show low surgical resectability at disease progression. SRS and chemotherapy could be considered as salvage treatment options. Despite the risk of radiation necrosis, it cannot be ignored that SRS has some therapeutic effect in patients with anaplastic meningioma. Helis et al. [37] reported distant control failure (49.1%) and local control failure (36.0%). In this study, 2-years local control rates was 65% and distant control failures in 69.2% cases. Although the optimal timing of radiosurgery for atypical and anaplastic meningioma remains the subject of ongoing debate [37383940], SRS should be considered in patients who cannot afford additional radiotherapy. There have been several attempts at chemotherapy for anaplastic meningioma, but most of them had poor results [241]. In this study, only ICE regimen have modest beneficial effect on anaplastic meningioma.
Also, 16.6% of all patients had extracranial metastasis. Because routine systemic workup was not performed in all patients, it is considered to be an underestimated result. Although treatment options in the presence of extracranial metastasis are quite limited, but it is necessary to consider the need for a systemic workup to evaluate extracranial dissemination in the event of disease relapse.
This study has inevitable limitations as shown in the previous reports about anaplastic meningiomas from single institution, such as a long study span, retrospective study design, which limits the statistical power. Above all, there was a lack of consideration of TERT promoter mutation, homozygous deletion of CDKN2A/B and H3K27me3 loss of nuclear expression, which are newly emerging molecular findings. We expect that future studies explore the molecular biology in anaplastic meningioma and lead to the development of effective target agents in the near future.
In conclusion, adjuvant radiotherapy is an essential treatment arm in patients with anaplastic meningiomas. SRS seems to play an important role as a salvage treatment. But chemotherapy seems to have limited efficacy. Because of the disseminated nature of the disease, further investigations to improve prognosis are needed.
 XML Download
XML Download