

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Vestibular schwannomas (VS), also known as acoustic neuroma, are benign tumors of schwann cells that mostly originate from the superior vestibular nerve [1]. Many studies in the literature have reported that the incidence of VS ranges from 0.6 to 1.9 per 100,000 population [2345]. The incidence of VS has also been shown to be increasing, mostly because of technological advancements in detection methods, such as magnetic resonance imaging [34]. Classically, VS are found within the internal acoustic meatus, and when the tumors grow, they tend to expand into the cerebellopontine angle, with various symptoms resulting from mass effect. Treatment modalities include observation with serial imaging, stereotactic radiosurgery, or stereotactic radiotherapy and microsurgery. The choice of treatment is dependent on patient age, underlying diseases, clinical symptoms, and tumor size.
In certain situations, it is impossible to eradicate VS completely because the position of the tumor involves vital structures, such as facial nerves, other cranial nerves, or brain stems, which often lead to postoperative complications. Facial nerve weakness after VS resection is one of the most common complications following tumor removal, along with cerebrospinal fluid (CSF) leak, meningitis, and other cranial nerve deficits, or even death.
We recorded demographic data, clinical presentations, imaging data, facial nerve outcomes, and surgical complications among patients who underwent total and subtotal resection and compared results of patients having small to medium size VS with those with large VS and who underwent surgery in the same institution.
MATERIALS AND METHODS
Patient population
A retrospective study was conducted of patients who were surgically treated for VS between October 2008 and September 2020 at Rajavithi Hospital, Bangkok, Thailand. This study was approved by the Institutional Review Board of Rajavithi Hospital (approval no. 64057). Informed consent was waived due to the retrospective data collection. Of the total 72 patients who underwent surgery, 24 were excluded from this study: 17 of these were not included because they had undergone partial resection; 4 had no preoperative or postoperative data; 2 had preoperative facial nerve palsy; and 1 had bilateral VS. Information relevant to the study was recorded, including age, sex, clinical presentation, duration of symptoms, imaging data, tumor size, presence of hydrocephalus, and type of resection. Type of resection was classified by subjective intraoperative impression correlated with first postoperative imaging. More than 5% of residual tumors were defined as partial resection, 2%–5% were classified as subtotal resection (STR) and less than 2% were considered gross total resection (GTR) or near total resection (NTR) [6]. The tumor size was measured as the largest single preoperative tumor diameter including the intracanalicular portion of the lesion. Definition of cystic VS was a cyst component that is more than 50% of total volume [7]. Facial nerve outcomes at 1 month, 1 year follow-up and surgical complications were observed only in those who underwent total and subtotal resection. Postoperative facial nerve function was classified according to the House-Brackmann (HB) facial grading scale as good (HB grade I–III) or poor (HB grade IV–VI). In all operations, the retrosigmoid approach was used, with the patient in the parkbench or sitting position, and continuous facial nerve monitoring was performed in most cases. The patients were divided into two groups: Group A consisted of patients with VS ≥3 cm, and Group B comprised patients with VS <3 cm [89].
RESULTS
The records were reviewed of 48 patients, all of whom had undergone the retrosigmoid approach; 30 patients (62.5%) had tumor size ≥3 cm (Group A), and 18 patients (37.5%) had tumor size <3 cm (Group B). The subjects ranged in age from 21 to 72 years, with a mean age of 52.8 years, and females accounted for 72.9% of the total number of patients studied.
Clinical presentation and imaging data
Group A
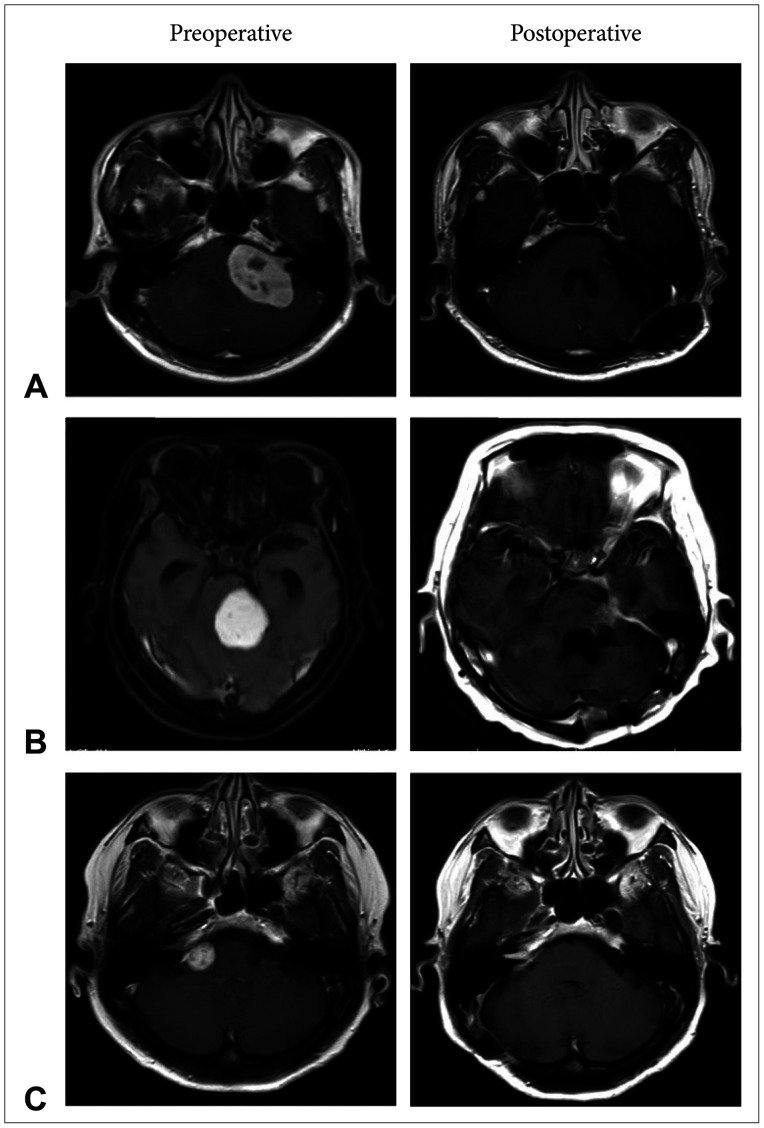
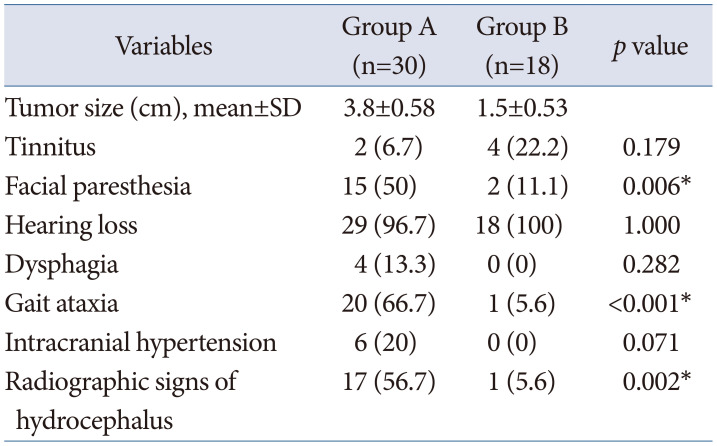
Patients’ mean age was 51.4 years (range 21–71 years) (Fig. 1A and B). There were more women (70%) than men (30%), and the left side was involved in 22 cases (73.3%) and the right side in 8 (26.7%). The mean duration of symptoms was 10.1 months (range 1–24 months), and the mean tumor size was 3.8 cm (range 3.0–5.3 cm) (Table 1). Preoperative imaging showed cystic VS in 10 patients (33.3%) and solid VS in 20 (66.7%). Nearly all patients had hearing dysfunction; 20 (66.7%) had gait ataxia; 15 (50%) had decreased facial sensation; 6 (20%) had signs of intracranial hypertension; 4 (13.3%) had dysphagia; and 2 (6.7%) had tinnitus. Radiographic signs of hydrocephalus were observed in 17 patients (56.7%): 16 (53.3%) had obstructive hydrocephalus; 1 (3.3%) had communicated hydrocephalus. Five patients (16.7%) had ventriculoperitoneal shunts inserted previously at another institute. After surgery, 10 patients (33.3%) had improvement in hydrocephalus, only 2 patients (6.7%) had undergone postoperative shunt placement.
Group B
Patients’ mean age was 55.2 years (range 30–72 years) (Fig. 1C), 14 patients (77.8%) were female. The left side was involved in 5 cases (27.8%) and the right side in 13 (72.2%). The mean duration of symptoms was 18.3 months (range 1–108 months), and the mean tumor size was 1.5 cm (range 0.6–2.4 cm) (Table 1). Preoperative imaging showed solid VS in every cases. All patients had hearing dysfunction; 4 (22.2%) had tinnitus; 2 (11.1%) had decreased facial sensation; 1 (5.6%) had gait ataxia; but no patient had signs of intracranial hypertension or dysphagia. Radiological evidence of hydrocephalus was found in 1 case (5.6%). None of these patients had undergone preoperative or postoperative ventriculoperitoneal shunt placement.
Statistical analysis revealed significant differences in the 2 groups in terms of gait ataxia, facial paresthesia, radiographic signs of hydrocephalus (Table 1).
Facial nerve outcomes and surgical complications
Group A
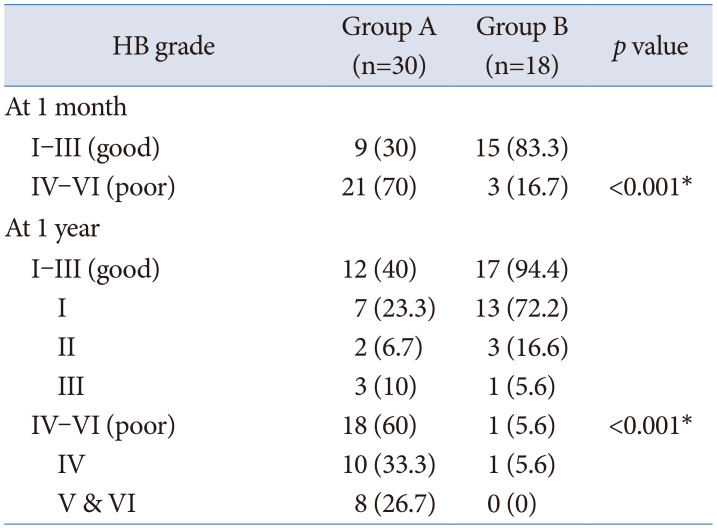
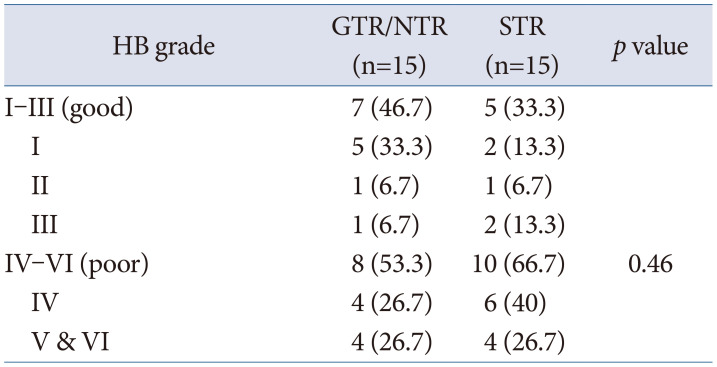
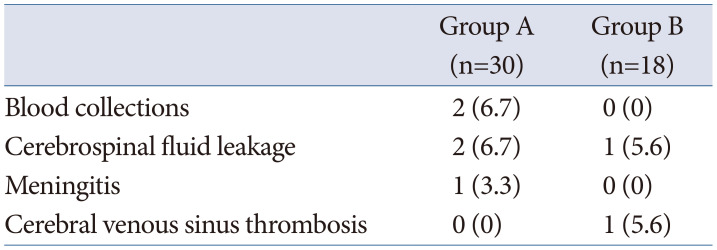
HB grade I–III (good) was found in 9 patients (30%) at 1 month and 12 patients (40%) at 1 year follow-up, and HB grade IV–VI (poor) was observed in 21 (70%) at 1 month and 18 (60%) at 1 year follow-up (Table 2). Comparing facial nerve outcome at 1 year between GTR/NTR and STR showed HB grade I–III (good) in 7 patients (46.7%) in GTR/NTR group and 5 patients (33.3%) in STR group, HB grade IV–VI (poor) was found in 8 (53.3%) and 10 (66.7%) in GTR/NTR group and STR group, respectively (Table 3). Two patients (6.7%) were discovered to have postoperative hematoma on immediate postoperative CT scan and were reoperated on with craniectomy and clot removal. Two patients (6.7%) developed CSF leaks, and one developed meningitis and epidural abscess. Both patients underwent further surgery repaired with fat graft (Table 4).
Group B
HB grade I–III (good) was found in 15 patients (83.3%) at 1 month and 17 patients (94.4%) at 1 year follow-up, while the remaining 3 (16.7%) and 1 (5.6%) had HB grade IV–VI (poor) at 1 month and 1 year follow-up, as shown in Table 2. One patient (5.6%) developed CSF leaks that required surgical repair, and one person (5.6%) developed sagittal sinus thrombosis on postoperative day 5; this was treated with an oral anticoagulant (Table 4). The perioperative mortality rate in both groups was 0%.
DISCUSSION
The incidence of large and giant tumors among all cases of VS has been estimated to be 14% in Western countries [5], but in developing countries they may comprise the majority [10]. Patients most typically present with hearing loss and tinnitus, which occur in 95% and >60% of cases, respectively [11]. Clinical presentations of patients with large VS differ from those of people with smaller tumors. According to the literature reviewed, patients with large VS tended to present with gait instability from compressive effects on the middle cerebellar peduncle in 64%–88% of cases, facial paresthesia from trigeminal nerve dysfunction in 34%–78% of cases, and dysphagia from lower cranial nerve dysfunction in 10%–14% of patients [101213]. Since we carried out our research in a tertiary care hospital, we found large VS in 62.5% of all treated cases. Presenting symptoms included gait imbalance at 66.7%, facial paresthesia at 50%, and intracranial hypertension at 20%; these finding were consistent with those of other studies [101213].
The main factor influencing postoperative facial nerve function was tumor size [1114]. The risk of facial nerve dysfunction in patients with VS >3 cm is 6-fold greater than in those with smaller VS [14]. Many studies have revealed rates of preservation of function of facial nerve after removal in large size of VS varying between 42% and 84% [12151617]. In other research, facial weakness after surgery was found to result in lower quality of life scores [1819]. Some studies have revealed contrasting long-term tumor control outcomes in terms of GTR and STR. The strongest predictor of recurrence was type of resection, patients undergoing STR having a nearly 11-fold greater risk of recurrence than those treated with GTR [20].
In this study, we analyzed facial nerve outcomes at 1-month and 1-year follow up and divided the results into good (HB grade I–III) and poor (HB grade IV–VI) outcomes. There were 30% and 40% of patients with large VS had good facial nerve outcomes at 1 month and 1 year follow-up in contrast with their counterparts with small to medium tumors, who had good facial nerve results. Regarding in different resection type (GTR/NTR and STR), there were no significant difference in facial nerve outcome statistically. Since the primary goal of surgery in our center is to attempt complete surgical removal of all tumors, large tumor size (mean tumor size in Group A about 3.8 cm) and we do not routinely use continuous facial nerve monitoring, we have achieved lower rates of preservation of facial nerve function than those found in some other studies. Radiosurgery is not our first option for VS treatment because there are very limited resources available and cost is also cannot be reimbursed. Therefore microsurgical resection is the first option of treatment in Thailand. With regard to primary treatment for radiosurgery in large size VS (2–4 cm), some studies have shown good tumor control rates, ranging from 87.0%–90.5%, and also acceptable preservation of neurological function [212223], even though there have been some cases of treatment failure. To obtain good tumor control and facial nerve function preservation, a combination of STR and postoperative radiosurgery might be a superior treatment option for large VS [2425] and may also result in good quality of life [25].
In the present study, there were no cases of postoperative mortality and no significant neurological complications. Two patients had postoperative hematoma that required surgery; one developed hemiparesis and the other had no neurological deficit. One case developed CSF leakage and, subsequently, epidural abscess.
There were some limitations to this study. Firstly, we did not collect data regarding recurrence or regrowth of tumors. Secondly, it was a retrospective study with data collection only from medical records.
In conclusion, patients with large-sized VS (≥3 cm) microsurgical resection had significantly poorer facial nerve outcomes than those who had VS <3 cm. As an alternative treatment for large VS, planned STR with postoperative radiosurgery might be superior in terms of neurological outcomes and may result in better quality of life in cases of large VS.
 XML Download
XML Download