

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Bioresorbable vascular scaffold (BVS) was developed as an alternative to metallic drug-eluting stent (DES) with the aim of providing transient vessel support combined with drug delivery capacity but without the long-term limitations of metallic DES.1 Although DES has been a predominant device for coronary revascularization, previous studies consistently reported that DES is related with annual 2–3% of late stent-related events up to 15 years with no plateau.2 Initial reports using everolimus-eluting BVS (AbsorbTM, Abbott Vascular, Santa Clara, CA, USA) showed favorable clinical event rates up to 5 years of follow-up34 and those studies showed BVS could be completely resorbed within 3 years after implantation.5
In contrast, previous randomized trials and meta-analyses showed significantly higher risk of device thrombosis and device-oriented composite outcomes, especially target vessel myocardial infarction (TVMI) in patients treated with BVS than with DES at mid-term follow-up.6789 Furthermore, BVS failed to show superior vasomotor reactivity and had significantly higher late luminal loss than DES.6 Based on these safety concerns of Absorb BVS, the manufacturer withdrew BVS from the market. Subsequent analysis revealed that both earlier (≤ 1 year) and late (> 1 year) adverse events of BVS were mainly associated with suboptimal procedural results including scaffold under-sizing, malapposition and inappropriate selection of target lesion with small reference diameter (< 2.25–2.75 mm).10111213 However, whether technical refinement such as pre-dilation, sizing and post-dilation technique or use of intravascular imaging can improve clinical outcomes in patients receiving BVS remains uncertain.
In this regard, the current study sought to evaluate safety and efficacy of BVS implanted by meticulous device optimization with a low threshold for intravascular imaging compared with 2nd generation DES in a broad spectrum of patients.
METHODS
Study design and patient-pooled population
The current study is patient-level pooled analysis of 2 independent registries. First, the REal World Advanced Experience of BioResorbable ScaffolD by SMart Angioplasty Research Team (SMART-REWARD) registry is a multicenter, prospective registry that was designed to evaluate the efficacy and safety of BVS with minimal exclusion criteria. From October 2015 through December 2017, a total of 390 patients treated with Absorb and Absorb GT1 (Abbott Vascular) for coronary artery disease were enrolled from 19 centers in Korea. Exclusion criteria included cardiogenic shock, cardiopulmonary resuscitation, and patients with a life expectancy < 2 years. Although SMART-REWARD intended to enroll 1,000 patients, subject enrollment was discontinued after withdrawal of BVS from the market. Among the enrolled population, 13 patients lost to follow up were excluded from the analysis.
Second, the Prognostic Perspective of Invasive Hyperemic and Non-Hyperemic Physiologic Indices Measured After Percutaneous Coronary Intervention (PERSPECTIVE-PCI) registry is a multicenter, prospective registry that was designed to evaluate the prognostic implications of post-PCI physiologic indexes.1415 From May 2013 through December 2019, a total of 675 patients were enrolled from 5 centers in Korea. Exclusion criteria included post-PCI thrombosis in myocardial infarction flow grade < 3, left ventricular ejection fraction < 30%, culprit lesions for acute coronary syndrome, graft vessels, collateral flow feeder, in-stent restenosis as target lesion, primary myocardial or valvular heart disease, cardiogenic shock, cardiopulmonary resuscitation, and patients with a life expectancy < 2 years. Forty-nine patients were excluded from the analysis due to overlapped patients with SMART-REWARD registry (n = 12), patients treated by drug-coated balloon (n = 26), or plain-old balloon angioplasty (n = 11).
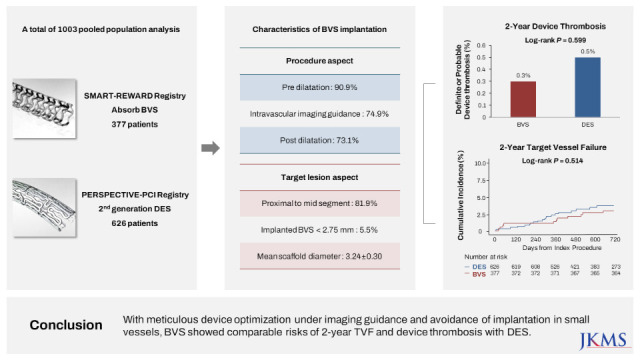
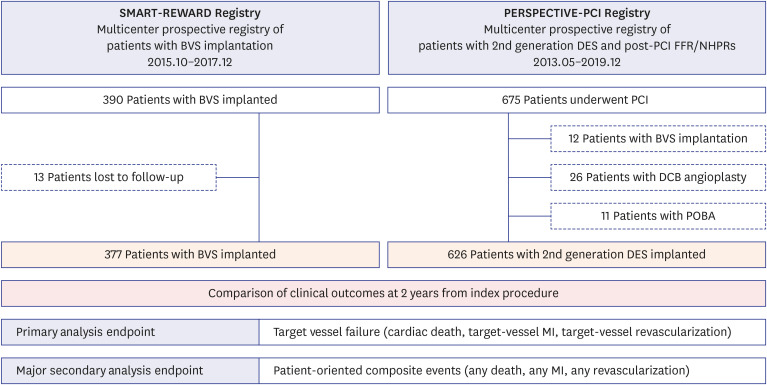
Therefore, the current study analyzed a total of 1,003 patients, with 377 patients implanted with BVS and 626 patients implanted with 2nd generation DES implanted (Fig. 1).
Fig. 1
Study flow. Study flow is presented. Two independent registries were used in current study. Among the population of the SMART-REWARD registry (390 patients), patients with unavailable follow-up data were excluded, leaving 377 patients with BVS implantation. Among the population of the PERSPECTIVE-PCI registry (675 patients), overlapped patients with SMART-REWARD registry and patients with DCB angioplasty and POBA were excluded, leaving 626 patients with 2nd generation DES implantation. A total 1,003 patients with clinical outcomes of 2 years of follow-up were pooled for analysis.
BVS = bioresorbable vascular scaffold, DCB = drug coated balloon, DES = drug-eluting stent, FFR = fractional flow reserve, MI = myocardial infarction, NHPR = non-hyperemic pressure ratio, PCI = percutaneous coronary intervention, POBA = plain old balloon angioplasty.
Procedures of BVS
All interventions were performed using standard techniques.16 A loading dose of aspirin 300 mg was given 24 hours before PCI, unless patients were already on aspirin therapy for at least 7 days. A loading dose of clopidogrel 300–600 mg, prasugrel 60 mg, or ticagrelor 180 mg was given 24 hours before PCI according to clinical presentation, unless patients were already on P2Y12 inhibitor therapy for at least 7 days.17 Unfractionated heparin or low-molecular weight heparin was used for procedural anticoagulation according to standard protocol. After the index procedure, all patients were recommended to take aspirin (at least 100 mg/day) indefinitely and a P2Y12 inhibitor at least 12 months from the index procedure.
Implantation procedures were conducted according to up-to-date manufacturer’s recommendations. Listed below are the detailed prespecified techniques recommended for BVS implantation: 1) Target lesion was pre-dilatated with adequate size of balloon comparable with reference target vessel diameter; 2) After delivery, scaffold was expanded slowly to nominal diameter by increase of 2 atmospheres (atm) every 5 seconds; 3) Post-dilatation using non-compliant (NC) balloon was left to operator discretion and the use of oversized NC balloon whose diameter exceeded scaffold diameter by 0.5 mm should be avoided; 4) The use of intravascular ultrasound or optical coherence tomography (OCT) was strongly recommended before and after scaffold implantation; 5) When kissing balloon inflation was needed in bifurcation lesions, mini-kissing balloon technique was applied; 6) In long lesions requiring 2 or more scaffolds implantation, scaffolds were overlapped with no-overlap-no-gap technique; and 7) Concurrent implantation of DES was allowed per operator discretion.
Coronary physiologic assessment and procedures of DES arm
In DES arm, detailed description of the PERSPECTIVE-PCI registry was published in previous studies.1415 Briefly, PERSPECTIVE-PCI registry mandated pre-PCI fractional flow reserve (FFR) ≤ 0.80 as a prerequisite for performing PCI. Coronary intervention was performed using current standard techniques with 2nd generation DES. Type of DES, stenting techniques, and need for post-stent balloon inflation were left to operator discretion. The use of intracoronary imaging devices was strongly recommended before and after DES implantation. After angiographically successful PCI, post-PCI FFR was measured under maximal hyperemia using intracoronary administration of nicorandil (2 mg), continuous infusion of intravenous adenosine (140 ug/kg/min), or intracoronary adenosine. Further evaluation by intracoronary imaging devices and optimization of stented segment in case of suboptimal post-PCI FFR value were left to operator discretion. In case of further optimization was performed, final post-PCI FFR was measured and reported.1415
Data collection, follow-up, and study endpoints
Demographic data, cardiovascular risk factors, and comorbidities were recorded at the time of index procedure. Coronary angiograms were reviewed and analyzed by an independent core laboratory at Samsung Medical Center. Patient follow-ups were performed at 6, 12, and 24 months by outpatient visits or telephone contacts. The median follow-up duration of the pooled analysis population was 720.0 (interquartile range: 643.0–720.0) days.
The primary analysis endpoint was target vessel failure (TVF), a composite of cardiac death, TVMI, and clinically driven target vessel revascularization during 2 years of follow-up. The key secondary analysis endpoint, the patient-oriented composite outcome (POCO), included all-cause death, any MI (including nontarget vessel territory), and any revascularization. All clinical events were defined in Academic Research Consortium (ARC) report. All death were considered cardiac unless an undisputed noncardiac cause was present. Periprocedural MI was not accounted as a clinical event. Revascularization was considered clinically indicated in the presence of diameter stenosis ≥ 50% and if one of the following occurred: 1) recurrence of angina symptoms; 2) positive non-invasive test; 3) positive invasive physiologic test; or 4) presence of diameter stenosis ≥ 70%, even in the absence of other criteria. Other secondary endpoints included individual component of TVF and POCO, and device thrombosis, defined as definite or probable according to the ARC definitions.18
Statistical analysis
All data of pooled analysis population were analyzed on per-patient basis. Vessels with the most severe stenosis was selected as the representative vessel in patients with multivessel PCI at the time of index procedure. Additional lesion-level analysis of target lesion and procedural characteristics in patients treated with BVS was performed to compare the results of current study and previous landmark clinical trials of BVS. All discrete and categorical variables were presented as numbers and relative frequencies (percentages). Continuous variables were expressed as mean ± standard deviation or median (interquartile range) according to their distribution, checked by Kolmogorov-Smirnov test and visual inspection of Q-Q plot. The cumulative incidence of clinical events was presented as Kaplan-Meier estimate and compared using a log-rank test. Multivariable Cox proportional hazards regression was used to calculate adjusted hazard ratio (HR) and 95% confidence interval (CI) to compare the risk of clinical events between groups. The assumption of proportionality was assessed by the Schoenfeld residuals and graphically by the log-log plot. The adjusted covariables were age, hypertension, diabetes mellitus, chronic kidney disease, previous MI, acute coronary syndrome, multivessel disease, left main (LM) disease, target vessel location, ACC/AHA lesion class B2 and C, multivessel PCI. Multivariable Cox proportional hazard model was also used to identify independent predictors for TVF.
To adjust for uneven distribution of baseline characteristics according to implanted devices, an inverse probability weighted (IPW) Cox proportional hazard regression model and propensity score matching with a stratified Cox proportional hazard regression model were used for comparison of clinical outcomes in pooled analysis population. In addition, Bayesian modeling with internal validation data was conducted as an additional sensitivity analysis to assess the effect of unmeasured confounders. All probability values were two-sided, and P values < 0.05 were considered statistically significant. Statistical analyses were performed using SPSS 20.0 for Windows (SPSS-PC, Chicago, IL, USA) and R version 4.1.1 (R Foundation for Statistical Computing, Vienna, Austria).
Ethics statement
Registries protocols were approved by the Institutional Review Board of Samsung Medical Center (approval No. 2015-07-163 for the SMART-REWARD registry; approval No. 2017-10-088 for the PERSPECTIVE-PCI registry), and written informed consent was obtained from all participants. The registry protocols were in accordance with the Declaration of Helsinki. The SMART-REWARD and PERSPECTIVE-PCI are registered at Clinicaltrials.gov (NCT02601404 and NCT04265443).
RESULTS
Baseline characteristics of patients
Table 1 presents comparison of baseline patient characteristics between BVS and DES groups. Among the 1,003 pooled population, 377 patients (37.6%) were treated with BVS, and 626 patients (62.4%) were treated with DES. Compared with the DES group, BVS patients had younger age, lower proportion of hypertension, diabetes mellitus, and chronic kidney disease. Conversely, proportion of patients with acute MI was higher in the BVS group than the DES group. Regarding angiographic disease severity, patients with BVS had lower proportions of multivessel disease and LM disease than those with DES.
Table 1
Comparison of baseline characteristics according to implanted devices
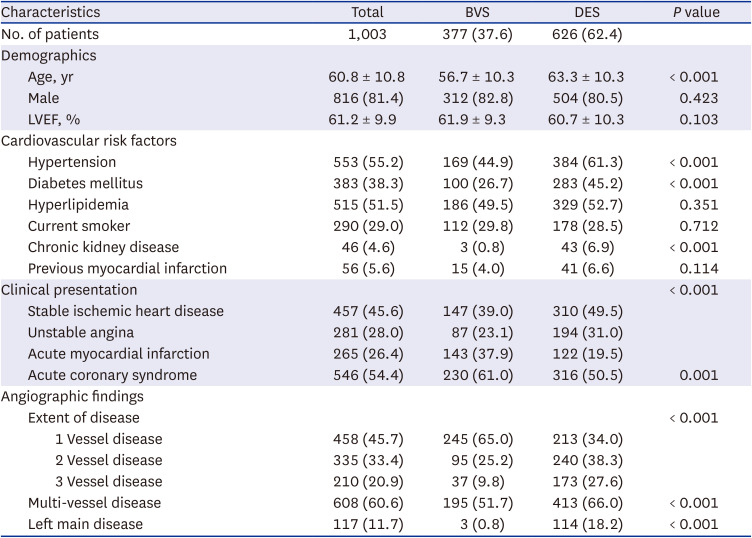
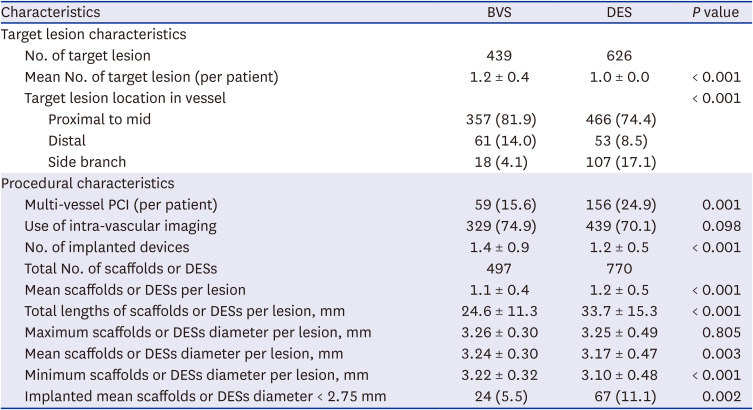
Table 2 shows target vessel and procedural characteristics. Among the target vessels, 69.4% had type B2/C lesion, which was slightly higher in the DES group. The rate of intravascular imaging device use was comparable between the 2 groups (74.0% and 70.1%, respectively for BVS and DES groups). Compared with DES patients, the diameter of implanted devices was larger and the length of implanted devices was shorter in patients with BVS.
Table 2
Comparison of target vessel characteristics according to implanted devices
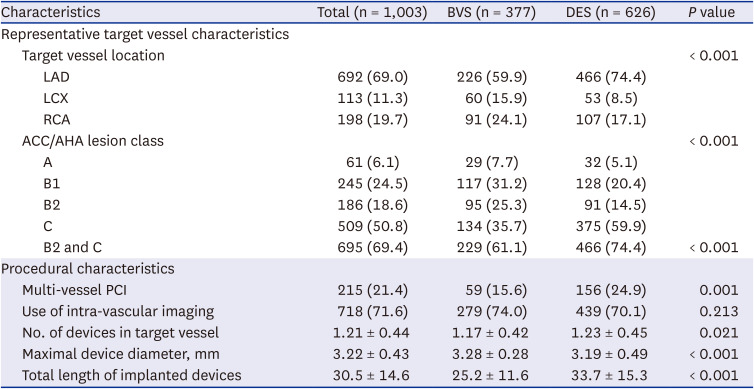
Data are expressed as number (%) or mean ± standard deviation.
BVS = bioresorbable vascular scaffold, DES = drug-eluting stent, LAD = left anterior descending artery, LCX = left circumflex artery, RCA = right coronary artery, ACC/AHA = American College of Cardiology/American Heart Association, PCI = percutaneous coronary intervention.
Procedural characteristics in BVS group
Table 3 and Supplementary Table 1 summarize detailed characteristics of target lesions and procedural characteristics in BVS group. A total of 439 target lesions were treated with 497 BVSs. Most target lesions (81.9%) were located at proximal to mid segment in target vessel. Pre-dilatation and post-dilatation were performed in 399/439 (90.9%) and 321/439 (73.1%) of lesions, respectively. Intravascular imaging devices were used in 329/439 (74.9%) of lesions for optimal scaffold implantation. Mean scaffold diameter per lesion was 3.24 ± 0.30 mm and total length of scaffolds per lesion was 24.6 ± 11.3 mm. Implanted scaffolds with mean diameter < 2.75 mm were identified in only 24 (5.5%) lesions. Supplementary Table 2 shows profiles of medical treatment in the BVS group. Dual antiplatelet therapy was prescribed at discharge for all patients with BVS and 56.3% continued DAPT at 2 years of follow-up. Clopidogrel, prasugrel and ticagrelor were prescribed in 55.7%, 8.0% and 36.3% of patients at discharge, respectively. At 2 years of follow-up, prescription of prasugrel and ticagrelor were documented in only 2.0% and 3.1% patients, respectively.
Table 3
Procedural characteristics for target lesions according to implanted devices
Clinical outcomes according to implanted devices
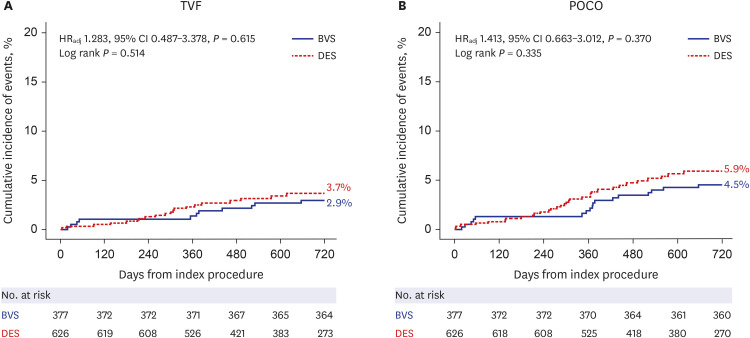
Table 4 presents comparison of clinical outcomes between the BVS and DES groups. The cumulative incidence of TVF at 2 years of follow-up was comparable between the BVS and DES groups (2.9% vs. 3.7%, adjusted HR, 1.283, 95% CI, 0.487–3.378, P = 0.615). There was also no significant difference in POCO between the 2 groups (4.5% vs. 5.9%, adjusted HR, 1.412, 95% CI, 0.663–3.012, P = 0.370) (Fig. 2). All individual components of TVF and POCO did not show any difference according to implanted devices (Supplementary Figs. 1 and 2). The cumulative incidence of definite or probable device thrombosis was also comparable between the BVS and DES groups (0.3% vs. 0.5%, adjusted HR, 2.515, 95% CI, 0.262–24.184, P = 0.424) (Table 4).
Table 4
Clinical outcomes at 2 years of follow-up according to implanted devices
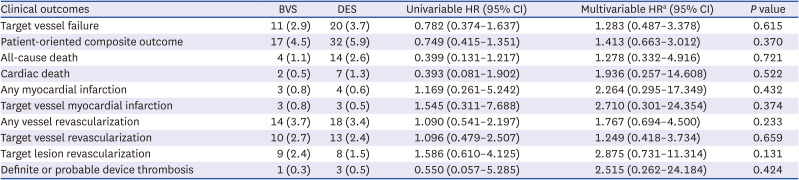
Data are expressed as number (%).
BVS = bioresorbable vascular scaffold, CI = confidence interval, DES = drug-eluting stent, HR = hazard ratio.
aAdjusted covariables were age, hypertension, diabetes mellitus, chronic kidney disease, previous myocardial infarction, acute coronary syndrome, multi-vessel disease, left main disease, target vessel location, American College of Cardiology/American Heart Association lesion class B2 and C, multi-vessel percutaneous coronary intervention.
Fig. 2
Comparison of primary and major secondary outcomes between BVS and DES. Kaplan-Meier curve is presented for 2-year cumulative incidence of (A) TVF and (B) POCO between BVS group and DES group. Multivariable Cox proportional hazard regression was used to calculate adjusted HR and 95% CI. The adjusted covariables were age, hypertension, diabetes mellitus, chronic kidney disease, previous MI, acute coronary syndrome, multivessel disease, left main disease, target vessel location, ACC/AHA lesion class B2 and C, multivessel PCI.
BVS = bioresorbable vascular scaffold, CI = confidence interval, DES = drug-eluting stent, HR = hazard ratio, MI = myocardial infarction, PCI = percutaneous coronary intervention, POCO = patient-oriented composite outcome, TVF = target vessel failure, ACC/AHA = American College of Cardiology/American Heart Association.
Sensitivity analysis regarding clinical outcomes
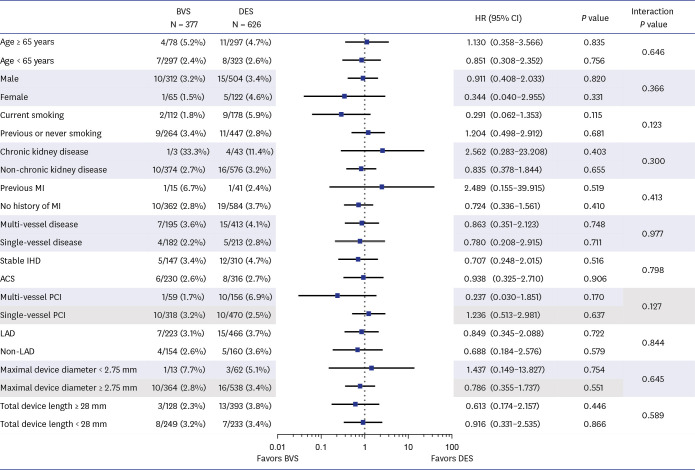
Table 5 shows the results of sensitivity analyses to adjust potential confounding effects between the 2 groups. Various sensitivity analyses consistently showed the comparable risk of clinical events between the BVS and DES groups. In addition, cumulative incidence of 2-year TVF and POCO in propensity score-matched population were also comparable between the 2 groups (log rank P = 0.686 and 0.708, respectively) (Supplementary Fig. 3). The results of the Bayesian analysis were also similar with the results from IPW adjustment and propensity score matched analysis. In addition, comparable risk of TVF between the BVS and DES group was consistently observed across various subgroups without significant interaction (Fig. 3).
Table 5
Sensitivity analysis regarding clinical outcomes according to implanted devices

CI = confidence interval, CrI = credible interval, HR = hazard ratio, IPW = inverse probability weighting, OR = odds ratio, PS = propensity score.
aPS was calculated based on multiple logistic regression model after adjusting for age, sex, hypertension, diabetes mellitus, hyperlipidemia, current smoker, chronic kidney disease, previous myocardial infarction, clinical presentation, extent of disease, multivessel disease, left main disease, target vessel location, American College of Cardiology/American Heart Association lesion class, multi-vessel percutaneous coronary intervention.
bTarget vessel failure defined as a composite of cardiac death, myocardial infarction (not clearly attributed to a nontarget vessel), or clinically indicated target vessel revascularization by percutaneous or surgical methods at 2 years.
cPatient-oriented composite outcomes included all-cause mortality, any myocardial infarction (includes nontarget vessel territory), any revascularization (includes all target and nontarget vessel, regardless of percutaneous or surgical methods).
Fig. 3
Comparison of 2-year risk of target vessel failure between BVS and DES according to subgroups. Cumulative incidence of target vessel failure at 2 years is compared between BVS group and DES group according to subgroup. The interaction P value represents the likelihood of interaction between the variable and the relative treatment effect.
ACS = acute coronary syndrome, BVS = bioresorbable vascular scaffold, CI = confidence interval, DES = drug-eluting stent, HR = hazard ratio, IHD = ischemic heart disease, MI = myocardial infarction, PCI = percutaneous coronary intervention.
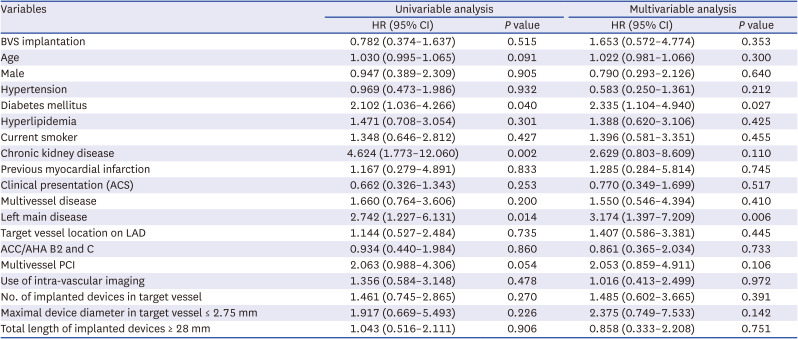
In multivariable analysis in original pooled population, the independent predictors for TVF were diabetes mellitus and LM disease, but not BVS implantation (HR, 1.653, 95% CI, 0.572–4.774, P = 0.353) (Table 6).
Table 6
Independent predictors for target vessel failure
DISCUSSION
The current study evaluated the safety and efficacy of BVS in all-comers patients from multicenter prospective registry. Key findings are as follows. First, compared with previous studies, BVS procedure in the current study was performed mostly in proximal to mid segment of vessel using ≥ 2.75 mm BVS with adequate scaffold optimization protocols guided by intravascular imaging. Second, regarding clinical outcomes after BVS implantation, there was no significant difference in mid-term risks of TVF or POCO between the BVS and DES groups. Third, the risk of device thrombosis was very low in BVS group without significant difference compared with DES group. Fourth, various sensitivity analyses showed consistent results supporting the comparable risk of clinical events between the BVS and DES groups.
Since initial approval of Absorb BVS at 2011 in Europe, randomized clinical trials (RCTs) reported comparable early and mid-term clinical outcome between BVS and 2nd generation DES.819202122 Among these RCTs, ABSORB III and AIDA trials evaluated the largest number of patients with reference vessel size of 2.50 to 3.75 mm and showed that BVS was non-inferior with DES in terms of device-oriented composite outcomes at 1 and 2 years of follow-up, respectively.1923 Similarly, initial reports of ABSORB II, ABSORB Japan, and ABSORB China also supported non-inferior efficacy of BVS compared with DES.202122 However, 3 years follow-up reports of ABSORB II trial showed significantly higher risk of target lesion failure (TLF) following BVS implantation than DES (10% vs. 5%, HR, 2.17, 95% CI, 1.01–4.69, P = 0.043), mainly driven by higher incidence of TVMI and definite or probable device thrombosis in the BVS group.6 It should be noted that ABSORB II trial included reference vessel size between 2.25 mm and 3.8 mm, and mean reference vessel diameter was much lower than other trials (Supplementary Table 3).
Furthermore, 3 years follow-up reports from ABSORB III trial showed significantly higher risk of device thrombosis in the BVS group than the DES group (2.3% vs. 0.7%, P = 0.01).7 Similar results were also observed in the AIDA trial (3.5% vs. 0.9%, P < 0.001).8 Device thrombosis in BVS consistently occurred on subacute, late and very late phases of follow-up period (Supplementary Table 4). Due to these safety concerns, BVS was withdrawn from the market in September 2017 and currently, no BVSs are available for clinical use. However, 5 years of follow-up data from the ABSORB III trial revealed that excess risk of BVS than DES ended after 3 years from index procedure, suggesting the possibility of favorable long-term clinical outcome after BVS implantation.24 The 5 years of follow-up data from the AIDA and ABSORB Japan trials also showed that the risk of device thrombosis in BVS group started to decrease after 3 years from index procedure, and the incident rate of device thrombosis was even lower than DES group during time periods of 3 to 5 years.242526 These data imply that more evidence is still needed to clarify the safety and efficacy of BVS in routine clinical practice and further study would be an important touchstone for future development of newer generation BVS.
Several possible mechanisms of device thrombosis of BVS were suggested in retrospective case analysis explored with OCT. In both the acute and subacute phases, malapposition, geographic mismatch and underexpansion of scaffold were revealed as major mechanical causes of device thrombosis.11 In addition to malapposition and underexpansion of scaffold, scaffold discontinuity and uncovered strut were investigated as main etiologies of late or very late device thrombosis.112728 Although the exact mechanism of scaffold discontinuity had not been clarified, it could be device-related inherent late resorption process or procedure-related scaffold fractures.2930 Uncovered strut was strongly affected by strut thickness, and endothelization of strut was influenced by flow dynamics and shear stress.31 More importantly, previous studies showed that BVS implantation in small reference vessels (< 2.25–2.75 mm) were significantly associated with smaller BVS expansion32 and increased risk of device thrombosis and TLF.7
In contrast with previous RCTs, the 2-year rate of definite or probable device thrombosis was only 0.3% in SMART-REWARD registry. Considering the possible mechanisms of BVS failure in previous studies, some important differences in procedural factors should be noted. In the current registry, meticulous prespecified implantation techniques were used and resulted in higher proportion of intravascular imaging guidance (74.9%), pre-dilatation (90.9%) and post-dilatation (73.1%) with high inflation pressure. Proportion of patients undergoing intravascular imaging guided-PCI in the SMART-REWARD registry was much higher than that in the majority of previous RCTs (ABSORB III, 11.2%; AIDA, not reported; and ABSORB China, 0.4%, respectively). In addition, 81.9% of target lesions were in proximal to mid segment of target vessel and only 5.5% of target lesions were treated with BVS size of less than 2.75 mm. These lesion characteristics led to relatively larger mean or maximal scaffold diameter (3.24 ± 0.30 mm or 3.26 ± 0.30 mm) compared with previous RCTs (Supplementary Table 2). All these scaffold optimization techniques with larger size of implanted BVS could explain the relatively lower incidence of device-oriented composite outcomes, including device thrombosis in the current registry.
The DES group of PERSPECTIVE-PCI registry was composed of patients treated under meticulous procedural optimization techniques guided by post-PCI FFR and intravascular imaging.1415 Those efforts of procedural optimization translated into relatively lower risk of TVF and POCO in the PERSPECTIVE-PCI registry. Although various types of DES were used in this registry, contemporary evidence supports comparable clinical outcomes across various types of 2nd generation DES.33 Even with this DES group serving as comparator group, BVS showed comparable risk of 2-year TVF, POCO and individual components of TVF and POCO. Although there were significant differences in baseline patient and lesion characteristics between the 2 groups, comparable risk of TVF was consistently observed in multiple sensitivity analyses with adjustment of measured or unmeasured confounders. In addition, clinical outcomes were not different between the 2 groups across various subgroups, and BVS implantation was not an independent predictor for 2-year TVF in multivariable analysis. All these sensitivity analyses support the comparable efficacy between BVS and DES in the current analysis. In this study, not only everolimus-eluting stent but also various 2nd generation DESs were used as comparator against BVS. However, because performance of 2nd generation DESs were not significantly different, it might have little effect on our study result.3435
It should be noted that the cumulative incidence of 2-year TVF and TVMI in the BVS group was relatively lower in the current study (2.9% and 0.8%, respectively) than AIDA (11.7% and 5.5%, respectively) or ABSORB Japan trial (11.1% and 5.0%, respectively).836 Although direct comparison among the studies would be limited, these differences might be explained by more frequent use of scaffold optimization techniques including intravascular imaging guidance and use of relatively larger size of scaffold which was mostly implanted at proximal to mid segments in ≥ 2.75 mm reference vessels. These results imply that appropriate selection of target lesion and meticulous procedural optimization are essential factors to prevent BVS-related adverse clinical events. In this regard, future research for safety and efficacy of next-generation BVS with thinner struts should commence with appropriate target lesion selection, using relatively larger size of BVS, and strict adherence to implantation techniques.
Some limitations of the study should be acknowledged. First, since this was non-randomized observational study, inherent limitation of selection bias should be considered. Second, neither patient nor physician could be blinded for the implanted devices. Third, current study evaluated 2 years of follow-up data, therefore, longer term safety and efficacy of BVS were not evaluated. Fourth, both BVS and DES groups were treated by high adoption rates of intravascular image-guided PCI, which may limit the generalizability of the results to other countries with limited adoption rates of intravascular imaging devices. Fifth, net clinical outcomes could not be evaluated, because, bleeding events had not been investigated as an individual endpoint in the PERSPECTIVE-PCI registry.
In all-comers patient population, BVS showed comparable risks of 2-year TVF and POCO with 2nd generation DES. BVS showed minimal risk of device thrombosis at 2-year follow up which was comparable with that of DES. The current study supports mid-term safety and efficacy of BVS in real-world practice. Use of meticulous device optimization technique utilizing intravascular imaging guidance and avoidance of BVS implantation in small vessels are suggested as possible procedural methods to reduce device thrombosis and adverse clinical events in patients receiving BVS implantation.
 XML Download
XML Download