

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
In December 2019, the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection was reported in Wuhan, China.1 Clinical manifestations that can occur due to SARS-CoV-2 infection range from asymptomatic infection to respiratory failure, septic shock, and multiorgan failure.23 As a significant number of bacterial co-infections were reported in influenza virus infections,45 empirical antibacterials have been commonly prescribed in the early studies of SARS-CoV-2 infection treatment.67 In general, empiric use of antibacterial agents is not recommended without evidence or suspicion for bacterial co-infection from several national coronavirus disease 2019 (COVID-19) management guidelines based on previous studies reporting that bacterial co-infection is uncommon in COVID-19.89 However, there have been some difficulties in adopting the results of previous studies to determine empirical antibiotic treatment in COVID-19. First, the rates of bacterial co-infection in COVID-19 patients varied from 2.7–52.6% according to hospital settings and regional differences.10111213141516 Second, microbiological testing for bacterial co-infection was conducted in less than half of the study population in most of the studies, which can lead to a substantial bias.1013171819 The purpose of this study was to answer two clinical questions for hospitalized COVID-19 patients: 1) the frequency of bacterial co-infection and 2) the clinical effect of empirical antimicrobial therapy. We assessed the rate of bacterial co-infection for hospitalized patients with COVID-19 in a single tertiary hospital in South Korea where testing for bacterial co-infection was conducted in the majority of patients. In addition, association between empirical antimicrobial therapy and mortality was evaluated.
METHODS
Study participants and study design
This retrospective study included all adult patients with COVID-19 who were hospitalized at a tertiary hospital (Asan Medical Center, Seoul, Korea) in South Korea between February 2020 and December 2021. Diagnosis of SARS-CoV-2 infection was confirmed by polymerase chain reaction (PCR) testing in all patients. Patients for whom bacterial sputum culture was not performed were excluded. Data on baseline demographics, comorbidities, laboratory findings, microbiological tests, radiological tests, management, and outcomes were collected by reviewing electronic health records. First, we measured the incidence of bacterial co-infection by reviewing the results of microbiological tests. In addition, we evaluated whether there was a difference in the frequency and composition of bacterial co-infection according to the history of antibacterial exposure prior to hospitalization. Second, effect of empiric antibacterial therapy on mortality was assessed by comparing 30-day mortality and in-hospital mortality between patients who received empirical antibacterials and those who did not.
Definitions
Empirical antibacterial therapy was defined as the administration of antibacterials without microbiological evidence of bacterial infection during hospitalization for COVID-19 treatment. Prior antibacterial exposure was defined as a patient exposed to antibacterial drugs within 30 days before admission. If the patient was diagnosed with COVID-19 during hospitalization, prior antibacterial exposure was defined as the history of antibacterial exposure within 30 days prior to the COVID-19 diagnosis.
Microbiological data
Microbiological tests included bacterial sputum cultures, blood cultures, pneumococcal urinary antigen testing, Legionella urinary antigen testing, sputum Legionella pneumophilia PCR, and sputum multiplex PCR for Mycoplasma pneumoniae and Chlamydia pneumoniae. We excluded positive results for fungal or viral co-infections and sputum culture reporting as mixed growth or normal flora. Corynebacterium sp. And staphylococci other than Staphylococcus aureus were excluded from blood cultures. Bacterial co-infection was defined as positive results from microbiological tests collected within two days (48 hours) of hospitalization. Those collected more than two days after admission were regarded as secondary infections.20
Statistical analysis
Categorical and continuous variables are presented as frequencies with percentages and medians with interquartile range, respectively. Categorical data were compared using the χ2 test and continuous variables were analyzed using a t-test. To assess the association between empiric antibacterial therapy and clinical outcomes (30-day mortality and in-hospital mortality), a univariate and multivariate logistic regression model was used. To minimize the heterogeneity between patients with or without receiving empirical antibiotic therapy, a propensity score (PS)-matched patient cohort was created and adjusted for potential confounders including age, sex, mode of SARS-CoV-2 infection, diabetes, hypertension, cardiovascular disease, chronic kidney disease, chronic lung disease, chronic liver disease, solid cancer, hematologic malignancy, rheumatic disease, obesity, smoking, pregnancy, leukocytosis (white blood cell > 10,000), elevated creatinine (> 1.5), elevated C-reactive protein (> 7.5), and National Institutes of Health severity. After calculating the predicted probabilities, each individual in the empiric antibacterial therapy group was matched with those in the no empiric antibacterial therapy group at a 1:2 ratio using the PSs. The PS-matched pairs were created using calipers of width equal to 0.1 of the standard deviation of the logit of the PS. We applied greedy nearest neighbour matching, where each treated unit is sequentially matched with the nearest control units, without replacement and in the descending order of the PS. We employed the standardized difference of means to assess the differences in baseline characteristics. Model discrimination was assessed with C-statistics, and model calibration was assessed with the Hosmer-Lemeshow statistics in the PS model to predict the receiving empiric antibacterial therapy. Odds ratios and the corresponding confidence intervals for positive SARS-CoV-2 test results were calculated by conditional logistic regression in the matched samples after adjusting covariates. We performed subgroup analyses defined by age (≤ 60 years vs. > 60 years), sex, and COVID-19 severity. We also assessed the presence of interactions between these subgroups. In addition, we conducted a sensitivity analysis for the study cohort after excluding patients for whom microbiological evidence of bacterial co-infection was identified. P values less than 0.05 were considered statistically significant. Statistical analyses were conducted using R, version 4.0.4 (R Project for Statistical Computing, Vienna, Austria).
RESULTS
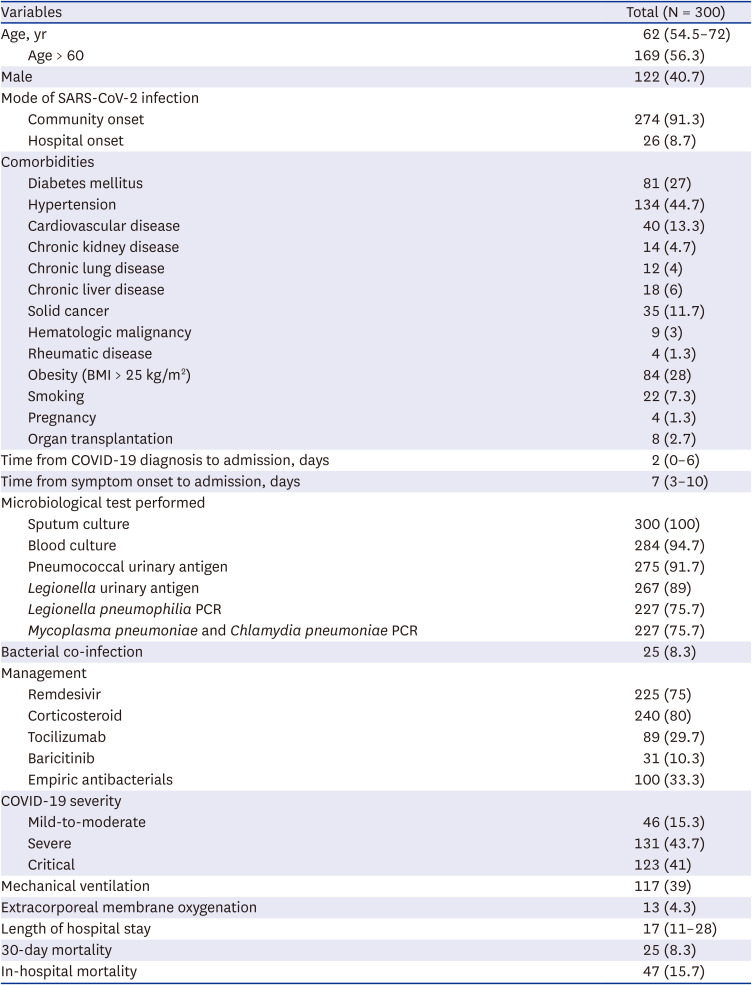
There were 367 adult patients admitted during the study period. After excluding 67 patients without sputum culture results, 300 (81.7%) patients were included in the analysis (Fig. 1). The median age was 62 years-old and 40.7% of the subjects were male. Most patients were diagnosed with community-acquired COVID-19, except for those who were newly infected with SARS-CoV-2 after two days of hospitalization for other medical reasons. Baseline characteristics and clinical outcomes of patients with COVID-19 are summarized in Table 1.
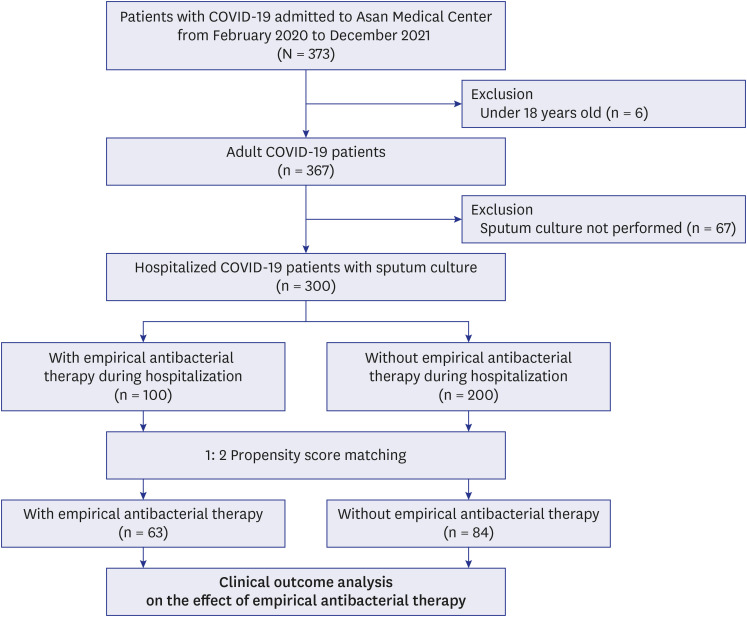
Table 1
Baseline characteristics, management, and outcomes of patients with COVID-19
Bacterial co-infection in patients with COVID-19
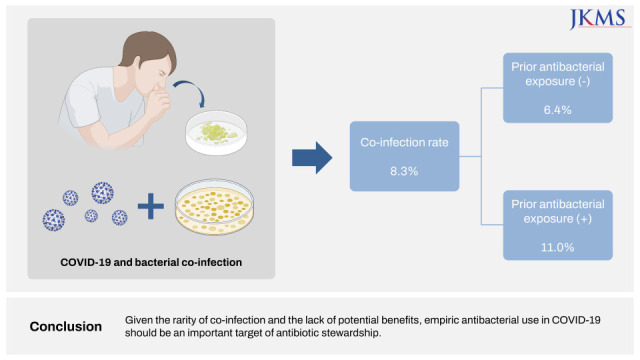
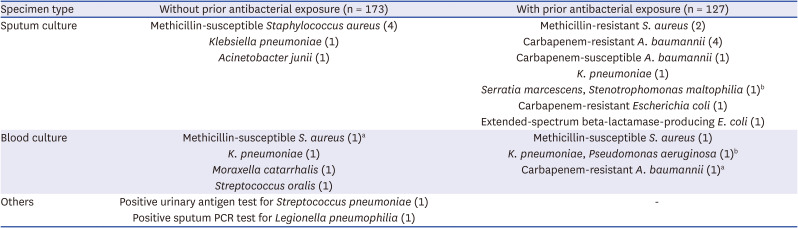
The crude rate of bacterial co-infection was 8.3% (25/300): 6.4% (11/173) of patients without antibacterial exposure before admission and 11.0% (14/127) of patients with prior antibacterial exposure (P = 0.218). As shown in Table 2, pathogens isolated in the group without prior antibacterial exposure were responsible for community-onset infections, such as methicillin-susceptible S. aureus, Klebsiella pneumoniae, Moraxella catarrhalis, Streptococcus oralis, Streptococcus pneumoniae, and L. pneumophilia. Those isolated in the antibacterial-exposed group were responsible for healthcare-associated infections or multi-resistant organisms, such as methicillin-resistant S. aureus, Acinetobacter baumannii, Pseudomonas aeruginosa, Stenotrophomonas maltophilia, and Carbapenem-resistant Escherichia coli.
Table 2
Cause of microbiologically confirmed respiratory and bloodstream infections
Baseline characteristics between patients with or without bacterial co-infection are summarized in Supplementary Table 1. The co-infection rate was higher in intensive care unit (ICU) patients, although statistical significance was not found.
Empirical antibacterial therapy in patients with COVID-19
Empirical antibacterials were prescribed in 33.3% (100/300) of patients. The clinical characteristics of patients group according to whether or not receiving empiric antibacterial therapy are summarized in Table 3. Empirical antibacterial therapy was significantly associated with in-hospital mortality in unadjusted analysis, but there this association was not significant in the multivariate analysis. Empirical antibacterial therapy was not significantly associated with 30-day mortality in unadjusted and multivariate analyses (Table 4). In the PS-matching analyses, empiric antibacterial therapy was not related to an increase or decrease in 30 day-mortality or in-hospital mortality (Table 4). In the subgroup analyses, no significant association was observed between empirical antibacterial treatment and mortality, regardless of age group, sex, and COVID-19 severity (all P for interactions > 0.05) (Table 5). The results of sensitivity analysis performed in the cohort excluding patients with bacterial co-infection also showed robustness as no significant association between empirical antibacterial therapy and mortality was observed.
Table 3
Baseline characteristics of patients with COVID-19 according to receiving empiric antibacterial therapy
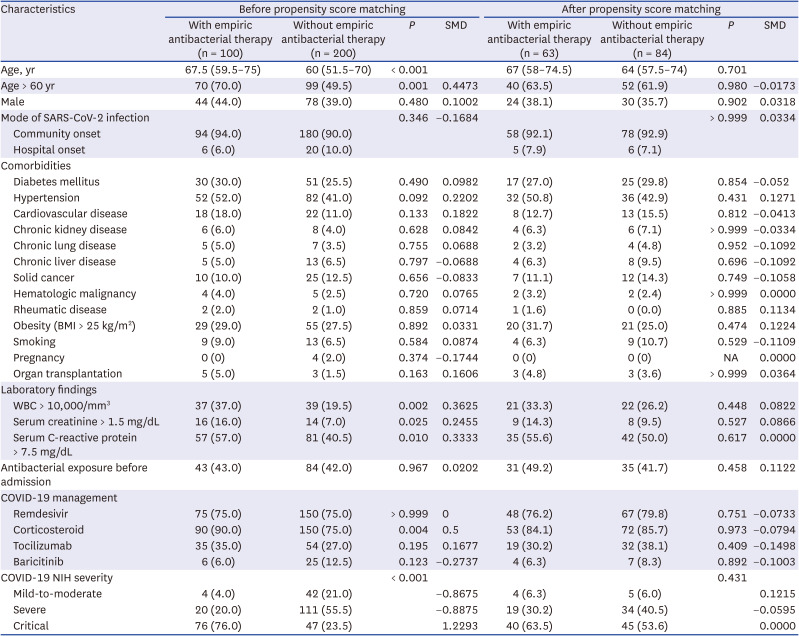
Table 4
Association between empirical antibacterial therapy and clinical outcomes

The following variables were adjusted in the multivariate analysis and propensity score-matching analysis: age, sex, mode of severe acute respiratory syndrome coronavirus 2 infection, diabetes, hypertension, cardiovascular disease, chronic kidney disease, chronic lung disease, chronic liver disease, solid cancer, hematologic malignancy, obesity, smoking, leukocytosis (white blood cell > 10,000/mm3), elevated serum creatinine (> 1.5 mg/dL), elevated serum C-reactive protein (> 7.5 mg/dL), antibiotic exposure before admission, coronavirus disease 2019 treatment (remdesivir, corticosteroid, tocilizumab, baricitinib), and National Institutes of Health severity.
OR = odd ratio, CI = confidence interval.
Table 5
Subgroup and sensitivity analyses for association between empiric antibacterial therapy and mortality
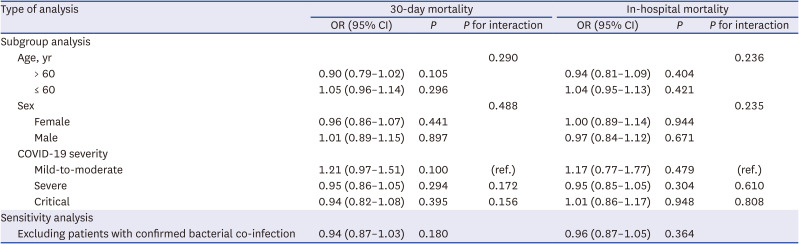
All subgroup and sensitivity analyses were adjusted for age, sex, mode of severe acute respiratory syndrome coronavirus 2 infection, diabetes, hypertension, cardiovascular disease, chronic kidney disease, chronic lung disease, chronic liver disease, solid cancer, hematologic malignancy, obesity, smoking, leukocytosis (white blood cell > 10,000/mm3), elevated serum creatinine (> 1.5 mg/dL), elevated serum C-reactive protein (> 7.5 mg/dL), antibacterial exposure before admission, COVID-19 treatment (remdesivir, corticosteroid, tocilizumab, baricitinib), and National Institutes of Health severity.
OR = odd ratio, CI = confidence interval, COVID-19 = coronavirus disease 2019.
DISCUSSION
In this observational study at a tertiary hospital where the majority of patients received microbiological testing, the crude rate for bacterial co-infection was low in patients with COVID-19. Although co-infection rates did not differ according to the history of previous exposure to antibacterials, the isolates in the unexposed group are mostly responsible for community-acquired infections, whereas multidrug-resistant or difficult-to-treat pathogens were predominantly detected in the antibacterials-exposed group. Empiric antibacterial therapy in patients without bacterial co-infection was not associated with lower mortality.
In the previous studies, the rate of bacterial co-infection in COVID-19 patients varied from 2.7–52.6%.10111213141516 One meta-analysis study published in 2020 found bacterial coinfection in 4.9% of COVID-19 patients on hospital admission and 16.0% on ICU admission.21 In another meta-analysis study, 7% of hospitalized COVID-19 patients had bacterial co-infection, a number that increased to 14% in studies that only included ICU patients.22 These findings may suggest the differences in the co-infection rates according to the severity of COVID-19, such as between ICU and non-ICU settings. Although there was no statistical significance, a higher co-infection frequency was observed in ICU patients in our study. In previous work in South Korea, coinfection with respiratory pathogens was detected in 8.8% of patients with COVID-19, which was also consistent with the results of our study.23
In most studies, sputum culture was performed in less than 30% of all study subjects confirmed to have SARS-CoV-2, which enabled an investigation regarding the rate of bacterial co-infection.1013171819 There is a possibility that fewer tests were performed because aerosol can be generated when securing the sputum specimen. Although the sputum collection is not considered as an aerosol-generating procedure in general, sputum induction or saline instillation via open circuit could generate contagious aerosol.24 Also, sputum may not have been discharged in the early stages of the disease, making it difficult to collect. Low rates of microbiological testing can lead to overestimation or underestimation, limiting the assessment of bacterial co-infection with COVID-19 in patients. On the other hand, in our study, of the 367 adult patients admitted during the study period, 300 (81.7%) had sputum culture results that were included in the analysis. The strength of this study was that sputum culture was performed within 48 hours of hospitalization in more than 80% of the study subjects, and the co-infection incidence was analyzed based on the results. In addition, unlike previous studies, we verified antibacterial exposure one month before the patient sample was secured.
Although the use of empirical antibacterials in patients with COVID-19 is not recommended, it occurs in a significant proportion. In the nationwide survey in South Korea, about 35% of patients with COVID-19 received empirical antibacterial therapy.25 However, the use of empirical antibacterials did not improve clinical outcomes including mortality and length of hospital stay in a retrospective study conducted at a single tertiary center in South Korea, which was consistent with the results of this study.26 Considering the low rate of bacterial co-infection and potential harm of antibacterial use such as inducing antimicrobial resistance and antibacterial drug-related toxicities, empiric use of antibacterials should be restricted in patients with COVID-19 unless the microbiological evidence or clinical suspicion of bacterial infection is evident.27 On the other hand, despite the low rate, since the bacterial co-infection is an important risk factor for COVID-19 mortality, microbiological tests such as sputum culture and blood culture should be performed for all hospitalized COVID-19 patients.1528 In particular, an early diagnosis strategy for bacterial co-infection for the appropriate use of antibacterials should be implemented.29
This study has some limitations. First, this study could have selection bias because of the nature of the single center retrospective study. Despite careful adjustments, our analyses might have missed some residual confounders, and a future prospective study is needed to reduce confounding variables. Second, in the case of patients transferred from other hospitals, antibacterials administered previously may decrease the diagnostic yield and the number of reported positive bacterial cultures. Finally, since the bacterial co-infection was evaluated based solely on microbiological tests, it is difficult to distinguish whether the positive results of the microbiological test are the result of colonization or true infection.
In this study which included only patients underwent microbiological testing, bacterial co-infection was infrequent, and the results varied depending on previous exposure to antibacterials. Considering the lack of benefit of empiric antibacterial therapy in the patients without microbiological evidence of bacterial co-infection as well as the potential risk for colonization of multi-resistant bacteria by prior antibiotic exposure, the use of antibacterials in patients with COVID-19 should be cautious. These findings reaffirmed that bacterial co-infection with COVID-19 is rare and potentiated various guidelines against the empiric use of antibacterial agents in patients COVID-19.
 XML Download
XML Download