

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
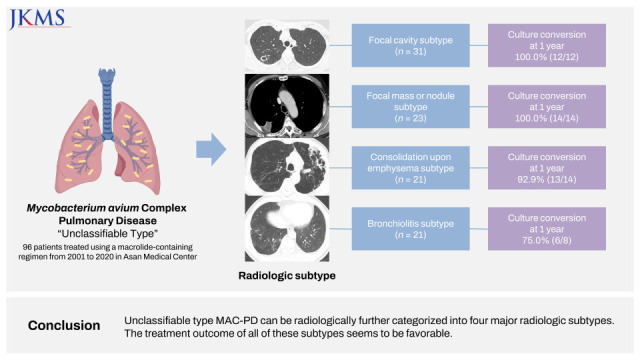
Mycobacterium avium complex (MAC) pulmonary disease (PD) can be radiologically classified into four types—fibrocavitary (FC), cavitary nodular bronchiectatic (C-NB), noncavitary nodular bronchiectatic (NC-NB), and unclassifiable types.123 Guidelines recommend that the treatment regimen and modality should be determined based on this classification.145 That is, in patients with the NC-NB type, an intermittent oral macrolid-based regimen is recommended. In contrast, in cavitary disease (FC and C-NB types), a daily oral regimen with an injectable agent is recommended.145 This difference in recommendation on the treatment modality is based on a previous study that reported different treatment outcomes according to the presence of cavitary lesions.2 In contrast, no specific recommendation is described regarding the treatment of patients with unclassifiable type MAC-PD in the guidelines, which can be attributed to the paucity of previous studies analyzing the treatment outcome of unclassifiable type MAC-PD.678
“Unclassifiable type” generally refers to MAC-PD that did not fall into any of the three main radiologic types. That is, patients were diagnosed with unclassifiable type only after their radiologic findings could not be classified into one of the other major types. Therefore, various radiologic forms can be classified as unclassifiable type, such as cases with solitary pulmonary lesion2 or consolidation,3 or in the case where the specific type could not be determined due to the presence of an underlying disease.3 However, there have been no studies that systematically analyze the radiologic subclassificaton of unclassifiable type MAC-PD. In addition, previous reports that analyzed the treatment outcome of MAC-PD excluded patients with unclassifiable type in their analysis,291011 probably due to the heterogenous radiologic findings of this type. Accordingly, there have been a few studies regarding its clinical features including the treatment outcome.678 Therefore, we aimed to investigate the radiologic subtypes and treatment outcome of unclassifiable type MAC-PD.
METHODS
Study subjects
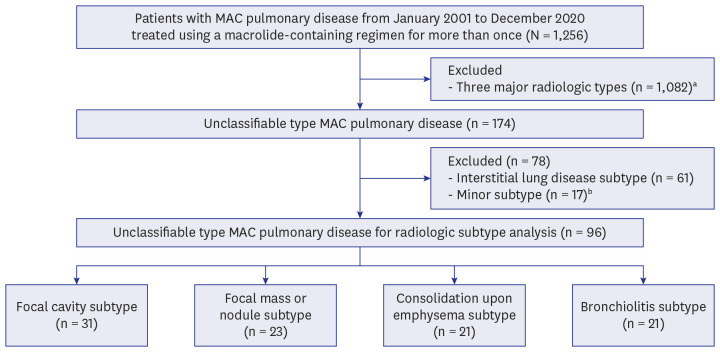
Patients were enrolled in the Asan Medical Center, which is a 2,700-bed referral hospital in Seoul, Republic of Korea. From 2001 to 2020, 1,256 patients who had MAC-PD and initiated treatment with a macrolide-containing regimen for more than once were identified. Among these, after excluding those whose computed tomography (CT) findings were classified into one of the three major types (FC, C-NB, NC-NB type), 174 patients who had other radiologic types remained. Among these patients, we first excluded those with interstitial lung disease (ILD) subtype of unclassifiable MAC-PD, which is defined as 1) patients had ILD such as usual interstitial pneumonia as an underlying disease, and 2) MAC-PD mainly occurred in the lesion already affected with ILD.12 Among the remaining patients, if the number of cases classified as a specific subtype was too small (less than 10), it was classified as one of the “minor subtypes” and further excluded. We assessed the radiologic findings of the remaining 96 patients to investigate radiologic subtypes of unclassifiable type (Fig. 1). All the patients met the microbiologic criteria of the guideline5: 1) at least two positive MAC cultures from sputum or 2) positive culture results from at least one bronchial washing or bronchoalveolar lavage, or 3) transbronchial or other lung biopsy with mycobacterial histologic features (such as granulomatous inflammation) and positive culture for MAC or biopsy showing mycobacterial histologic features and one or more sputum or bronchial specimen that are culture-positive for MAC.
Fig. 1
Study flow chart of radiologic subtype analysis.
MAC = Mycobacterium avium complex.
aIncluded fibrocavitary, cavitary nodular bronchiectatic, and non-cavitary nodular bronchiectatic type.
bMinor types included the radiologic findings of non-specific infiltrative lesion in the underlying tuberculous destroyed lung (n = 6), ground glass opacity (n = 3), nodules without tree-in-bud (n = 2), non-specific infiltrative lesion in underlying bronchiolitis obliterans (n = 2), disseminated nodular lesion (n = 1), acute respiratory distress syndrome (n = 1), and other types (n = 2).
Then, among these patients, those who received standard treatment (daily or intermittent three-drug oral antibiotics comprising macrolide, ethambutol, and rifampin with or without an injectable aminoglycoside) for ≥ 1 year were selected for the treatment outcome analysis.
Radiologic evaluation
Radiologic abnormalities on chest CT at the time of treatment initiation were evaluated by two pulmonologists and one radiologist. If any discrepancies were observed, a consensual decision was taken after discussion. Radiologic findings were first classified into FC, C-NB, and NC-NB type as previously determined,12 and all the remaining findings were classified as unclassifiable type. After excluding the ILD subtype and minor subtypes, the unclassifiable type was further sub-classified after thorough review and discussion.
Microbiological examination
During the study period, expectorated sputum or samples obtained from bronchoscopy were cultured in both solid media (Ogawa medium; Korean Institute of Tuberculosis, Seoul, Korea) and liquid media (BACTEC 960 Mycobacterial Growth Indicator Tube; Becton Dickinson, Sparks, MD, USA). Acid-fast bacillus (AFB) smears were made using Ziehl–Neelsen staining. A positive sputum smear was defined as AFB counts of > 1 per 100 high power fields. At our center, positive liquid cultures and colonies on solid media were subjected to polymerase chain reaction assays using Seeplex TB detection (Seegen, Seoul, Korea) to differentiate between Mycobacterium tuberculosis complex and nontuberculous Mycobacterium (NTM). NTM species were identified using reverse-blot hybridization of rpoB (GenoType Mycobacterium CM/AS; HAIN Lifescience, Nehren, Germany).
Patients were requested to submit expectorated sputum sample at least a one-month interval after treatment initiation. Sputum culture conversion was defined as three consecutive negative sputum cultures, with the time of conversion being determined as the date of the first negative culture. Treatment outcome in terms of culture conversion after treatment initiation was compared among the groups, and was determined according to the Nontuberculous Mycobacteria-Network European Trials consensus statement.13 In earlier studies, patients with persistently positive cultures after > 1 year of treatment were considered treatment failures1415; thus, the achievement of culture conversion at 1 year after treatment initiation was assessed as the main treatment outcome in the present study, as has been reported previously.210161718 In patients whose diagnosis was made on the basis of histologic findings alone, it was impossible to determine whether the patients achieved culture conversion. In these cases, the treatment result was determined on the basis of changes in radiologic findings with treatment.
Statistical analysis
All continuous data are presented as mean ± standard deviation, whereas categorical variables are presented as frequencies and percentages. Continuous variables were compared using the Kruskal-Wallis test, whereas categorical variables were analyzed by the χ2 test. We used the SPSS (version 24.0; SPSS, Chicago, IL, USA) analytical software for statistical analysis.
RESULTS
Study subjects for the radiologic subtype
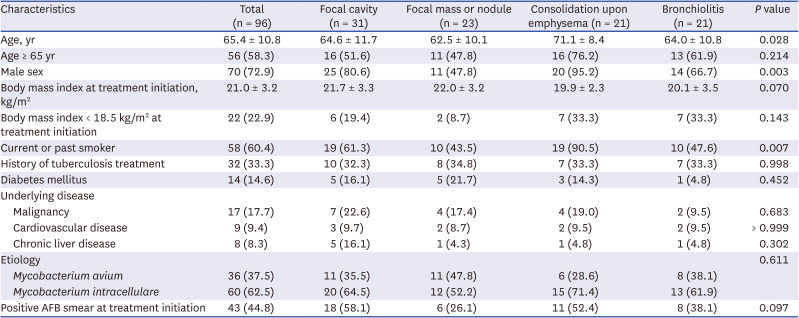
We identified 96 patients with unclassifiable type MAC-PD as eligible for participation in the radiologic subtype analysis (Fig. 1). Their mean age was 65.4 ± 10.8 years, and 72.9% of them were male. The mean body mass index at treatment initiation was 21.0 ± 3.2 kg/m2. The etiologic organisms included M. avium in 36 patients (37.5%) and M. intracellulare in 60 (62.5%) patients. Sputum AFB smear positivity was noted in 44.8% of patients (Table 1).
Table 1
Clinical characteristics of 96 patients with unclassifiable type Mycobacterium avium complex pulmonary disease according to radiological subtype
Radiologic subtype of unclassifiable type
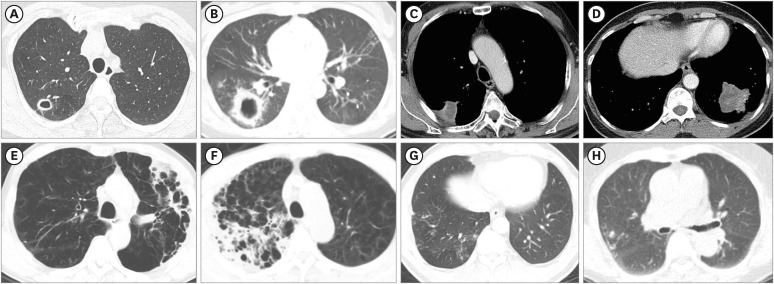
We classified the radiologic subtype of the 96 patients into four major subtypes. The typical CT findings of each of the four subtypes are shown in Fig. 2. First, if CT revealed a cavity lesion with or without adjacent satellite nodular lesions in a single lobe, without notable abnormal findings in all other remaining lobes, the patients were classified as having the focal cavity subtype (Fig. 2A and B). Second, the focal mass or nodule subtype was determined in the case of isolated consolidative lesion restricted to one lobe without affecting the other five lobes (Fig. 2C and D). Third, we defined the consolidation upon emphysema subtype as the identification of newly developed consolidative lesion(s) in the intervening normal lung parenchyma within underlying severe emphysema (Fig. 2E and F). Fourth, the patient was diagnosed as having bronchiolitis subtype if isolated or multifocal centrilobular nodules with tree-in-bud appearance were noted with or without focal bronchiectasis. This subtype was diagnosed only in the case where the right middle and lingular segments were not involved in the MAC-PD (Fig. 2G and H).
Fig. 2
Representative chest CT images of the four major radiologic subtypes of the unclassifiable type in the present study. (A) Chest CT of 53-year-old women showing an approximately 2-cm-sized thin-walled focal cavitary lesion in the right upper lobe. (B) Irregular-shaped thick-walled cavitary lesion of 4.2 × 3.7 cm in size was noted in the right lower lobe with adjacent multiple small nodular and branching linear-shaped parenchymal opacities in the chest CT of 35-year-old women. (C) CT scan of a 55-year-old man showing a focal consolidative nodular lesion with internal necrotic changes in the right upper lobe. (D) Irregular-shaped consolidative mass lesion in the left lower lobe was seen in the chest CT of 50-year-old women. (E) Newly developed infiltrative consolidation was noted in the left upper lobe in a 73-year-old male patient who had underlying diffuse centrilobular emphysema. (F) Chest CT scan of a 75-year-old male patient with centrilobular emphysema as a underlying disease showed consolidative infiltration in the right upper lobe. (G) Centrilobular nodules with tree-in-bud appearance was noted with focal bronchiectatic changes in the right lower lobe in the chest CT scan of a 62-year-old male patient. (H) Chest CT scan of a 79-year-old female patient showed a segmentally distributed centrilobular nodule with the tree-in-bud sign was seen in right upper lobe.
CT = computed tomography.
Among the four major subtypes of the unclassifiable type, the most common radiologic subtype was the focal cavity (n = 31, 32.3%), followed by the focal mass or nodule (n = 23, 24.0%), consolidation upon emphysema (n = 21, 21.9%), and bronchiolitis (n = 21, 21.9%) subtypes. The median size of cavity in focal cavity subtype was 3.0 cm (interquartile range [IQR], 1.9–3.8). The median number of involved lobes was 1 (IQR, 1–2) and 1 (IQR, 1–2) in the patients with the consolidation upon emphysema subtype and those with the bronchiolitis subtype, respectively. As shown in Table 1, there were no statistically significant differences in baseline characteristics between the four subtypes, except for age, sex, and smoking history.
Study subjects for treatment outcome analysis
Among 96 patients with the unclassifiable type, the number of patients who received standard treatment for ≥ 1 year was 48 (50.0%) patients. Fig. 3 presents the detailed reasons for exclusion in the remaining patients who received non-standard treatment or whose treatment duration was < 1 year. Table 2 shows the clinical characteristics of the 48 patients whose treatment duration was ≥ 1 year. Statistically significant differences in sex, body mass index, and smoking history were noted among these patients. Among the 48 patients involved in the treatment outcome analysis, treatment was maintained with three-drug intermittent or daily oral regimen in 30 patients (62.5%), whereas the remaining 18 (37.5%) patients received regimen composed of oral drugs as well as injectable aminoglycosides. No significant difference in terms of treatment modality was noted among the four subtypes (Table 3).
Fig. 3
Study flow chart of treatment outcome analysis.
EMB = ethambutol, MAC = Mycobacterium avium complex, RIF = rifampin.
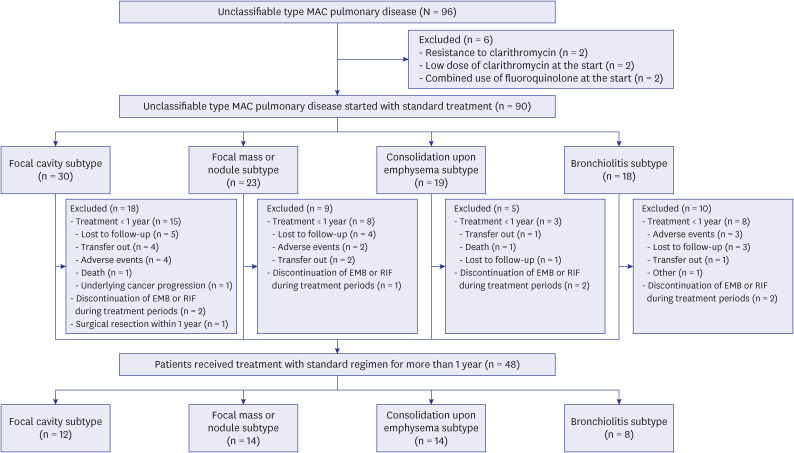
Table 2
Clinical characteristics of 48 patients with unclassifiable type Mycobacterium avium complex pulmonary disease received standard treatment for ≥ 1 year
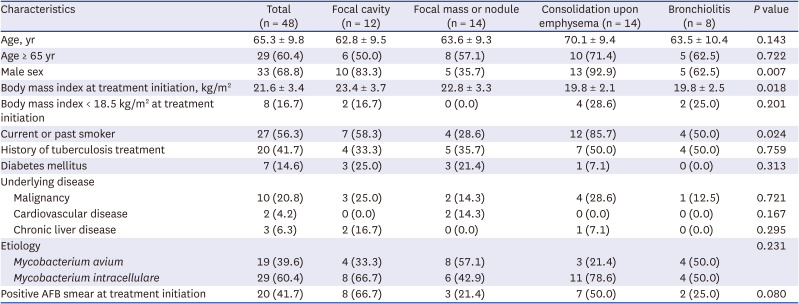
Table 3
Treatment regimen and outcome of 48 patients with unclassifiable type Mycobacterium avium complex pulmonary disease according to radiological subtype

Treatment outcome of unclassifiable type
As shown in Table 3, the overall 1-year culture conversion rate of the 48 patients was 93.8%. Notably, all patients in the focal cavity subtype and focal mass or nodule subtype categories achieved culture conversion at 1 year. In addition, the treatment responses of the patients with the remaining two subtypes were also successful; the 1-year culture conversion rate reaching 92.9% in the consolidation upon emphysema subtype and 75.0% in bronchiolitis subtype.
The univariate and multivariate analyses of the factors that affected treatment outcomes in 48 patients is presented in Supplementary Table 1, which showed that none of the variables were significantly related to the treatment outcome.
DISCUSSION
Although the unclassifiable type is categorized as one of the radiologic classifications in MAC-PD, there have been few studies on the radiologic subclassification and treatment outcome of this type thus far.678 To the best of our knowledge, this is the first study to systematically report the radiologic subtypes and treatment outcomes of the unclassifiable type through a retrospective analysis for 96 patients with unclassifiable type MAC-PD at a tertiary referral center in Republic of Korea. The key findings are as follows: 1) radiologically, the unclassifiable type can be further categorized into 4 major subtypes: focal cavity, focal mass or nodule, consolidation upon emphysema, and bronchiolitis subtypes, 2) the treatment outcome of patients who received standard treatment seemed generally favorable for all the four major subtypes, although the number of patients who were treated for ≥ 1 year was small. It should be noted that, ILD subtype of unclassifiable type was not included for the present study, as we have recently reported the clinical characteristics and treatment outcome of ILD subtype.12
The guideline defines the radiologic criteria for diagnosing NTM-PD as nodular or cavitary opacities on chest radiograph, or a high-resolution CT scan that shows bronchiectasis with multiple small nodules.5 Thus, it is unclear whether atypical CT findings of unclassifiable type MAC-PD such as focal consolidative lesion should be assessed as a manifestation of MAC-PD even if the growth of MAC was identified in respiratory specimen or tissue. Therefore, among these patients, we only included those who initiated macrolid-containing regimen for more than once for the radiologic subtype analysis in the present study. This is because, it can be considered that macrolide-based treatment could be initiated only after the diagnosis of MAC-PD was firmly established by the attending physician.
Overall, the high rate of culture conversion achievement in the 48 patients who received treatment for ≥ 1 year is a notable finding, given that the culture conversion rate at 1 year (93.8%) was significantly higher than what has been previously reported in the cavitary (FC or C-NB) or NC-NB type.2 We excluded patients who presented with radiologic types other than the unclassifiable type during the study enrollment process; therefore, we could not directly analyze the treatment outcome of patients with the unclassifiable type in comparison with those with other radiologic types. However, by using the data of participants of other studies from our center that were recently published,1619 we indirectly compared the treatment outcome according to the radiologic type. The baseline characteristics of patients with the unclassifiable, cavitary, or NC-NB type is shown in Supplementary Table 2. Supplementary Table 3 presents, after adjusting several factors that affect treatment outcome, that the treatment outcome of the unclassifiable type is significantly higher than that of the cavitary or NC-NB type. The high rate of 1-year culture conversion achievement in all 4 subtypes of the unclassifiable type could be related to the extent of the disease. Kuroishi et al.20 previously reported that sputum culture conversion after treatment was associated with the number of lobes that were involved; the number of involved lobes was significantly higher in the patients whose sputum had not converted to a negative result after treatment. Considering that the radiologic extent was confined within a single lobe in 2 subtypes (focal cavity and focal mass or nodule), and as the median number of involved lobes was 1 (IQR, 1–2) in both consolidation upon emphysema and bronchiolitis subtypes, the limited extent of disease could provide a plausible explanation of the favorable treatment outcome in the patients with the unclassifiable type.
Among the unclassifiable types, the most common radiologic subtype was focal cavity subtype. Therefore, we believe that the attending physician should be aware that MAC-PD can rarely develop as a focal cavity form, which is similar to pulmonary tuberculosis. Of 12 patients with focal cavity subtype who were treated for ≥ 1 year, an injectable aminoglycoside was administered to half of the patients; this clinical decision possibly reflects the current guidelines recommending aminoglycoside administration to patients with the cavitary type.1521 Notably, the 1-year culture conversion rate of 12 patients with the focal cavity subtype who received treatment for ≥ 1 year was 100%, and is in contrast with previous studies which reported that only 60–80% patients with cavitary disease (FC or C-NB type) achieved culture conversion at 12 months after treatment with the standard regimen.216 There could be several possible explanations for the disparate results in terms of treatment outcome: 1) the focal cavity subtype in the present study is different from the FC type because the cavity was not located in the apical lobe, associated with advanced volume loss and fibrosis.22 In addition, by definition, patients with the focal cavity subtype in the present study did not show any other abnormalities in other lobes, including bronchiectatic changes in the right middle lobe and lingular segment, as shown in the C-NB type.12 These different radiologic findings suggested that drug penetration into the cavitary lesion could relatively be preserved in the case of patients with the focal cavity subtype, as the destruction of the adjacent pulmonary parenchyma is less prominent than that in the FC or C-NB type. 2) Moreover, notable disparity is noted in the number of cavities. We recently reported that 53.3% and 38.8% of patients with MAC-PD with FC and C-NB type had ≥ 2 cavities.19 In contrast, all patients with the focal cavity subtype in the present study had one cavitary lesion. This difference of the number of cavitary lesion could constitute another plausible explanation for the favorable outcome of patients with the focal cavity subtype. Therefore, it could be concluded that, although the cavity is a classic marker of high mycobacterial burden, successful treatment outcomes could be expected in the case of focal cavitary involvement of MAC in a single lobe. However, more research is needed to ascertain the optimal regimen for this subtype.
It is known that NTM-PD can rarely present as a solitary pulmonary nodule or in a focal consolidative form,7823 which is the second most common subtype in the present study. Although the treatment outcome of this subtype was successful in previous studies and in the present study, invasive procedures such as percutaneous needle biopsy (PCNB) were frequently required for proper diagnosis; 56.5% (13/23) of the patients with this subtype in the present study were diagnosed on the basis of histologic findings obtained via PCNB, along with positive cultures from biopsy specimens. Conversely, the diagnosis of almost all patients in the other three subtypes was based on positive MAC cultures from sputum or bronchial specimens alone. Given that the focal mass or nodule subtype is the second most common subtype of unclassifiable type MAC-PD in our study patients, it should be emphasized that when the finding of chronic granulomatous inflammation was revealed on histology after biopsy, it should not be treated as a disease caused by M. tuberculosis without additional testing, even in tuberculosis-endemic countries. In this case, further examination, including rapid molecular test and/or AFB culture, should be performed, considering that histological resemblance between the disease caused by M. tuberculosis and NTM as well as the incidence of NTM-PD are rapidly increasing globally.
Structurally damaging lung diseases, such as bronchiectasis, cystic fibrosis, pneumoconiosis, and chronic obstructive pulmonary disease (COPD) is well known to increase susceptibility to NTM-PD.4242526 The classic phenotype of MAC-PD developed in COPD is the FC form, of which radiologic findings were characterized by upper lobe fibrosis, volume loss and cavitation with surrounding pleural thickening.2227 In contrast, we showed that MAC-PD could also develop in the form of infiltrative consolidative lesion(s) within intervening lung parenchyma around emphysema. An injectable aminoglycoside was added in 57.1% (8/14) patients and, therefore, this subtype was likely to be considered as a severe form by the attending physician and would be identified as requiring an aminoglycoside-containing regimen. Nevertheless, the majority (92.9%, 13/14) of patients achieved culture conversion at 1 year, and this is a higher success rate compared with that of the FC type. The successful treatment outcome in the consolidation upon emphysema subtype could be explained by the limited number of involved lobes and the absence of cavitary lesions.
The radiologic finding of centrilobular nodules sized < 1 cm with tree-in-bud signs is suggestive of inflammation mainly in the bronchioles and bronchus, which is commonly found in the CT of patients with NTM-PD.282930 In contrast to pulmonary tuberculosis, it is well known that these findings of nodules are typically associated with bronchiectasis in NTM-PD.2931 The present study suggested that, MAC-PD can also uncommonly present the focal bronchiolitis form characterized by isolated or multifocal small centrilobular nodules with a tree-in-bud appearance without involving bronchiectatic changes in the right middle lobe or lingular segment. These findings imply that the possibility of MAC-PD should be included in the differential diagnosis in the case of tree-in-bud opacities without bronchiectsis.32
Our study has some limitations, the most significant one was that it was conducted at a single referral center and it had a retrospective design. In addition, even considering that the unclassifiable type of MAC-PD seemed to be a rare disease entity, the number of patients with each subtype was small to analyze. Moreover, the treatment modality in each group was determined solely by each attending physician without a pre-established protocol. This approach was adopted because the optimal regimen for the treatment of unclassifiable type MAC-PD is unclear, especially on whether to include an injectable aminoglycoside to the regimen or to prescribe the drugs as an intermittent or daily administration regimen, which is in contrast to the established treatment modality in the FC, C-NB, and NC-NB types.145 Finally, only 48 patients received treatment for ≥ 1 year, and the regimen was nonuniform among the subtypes. Therefore, cautious interpretation of the treatment outcome, optimal treatment modality, and factors that affect the treatment outcome is needed.
In conclusion, unclassifiable type MAC-PD can be further subcategorized into four major subtypes on the basis of radiologic findings. The treatment outcome of these patients with oral macrolide-based three-drug antibiotics with or without injectable agents seemed favorable.
 XML Download
XML Download