

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Obstructive sleep apnea (OSA) can cause adverse pregnancy-related outcomes and has been confirmed by several nationwide data studies.12 OSA is associated with hypertensive disorders in pregnancy, gestational diabetes mellitus (GDM), preterm delivery, cesarean delivery, and small for gestational age neonates during pregnancy.3 Notably, many studies have been conducted on the relationship between OSA and gestational hypertensive disorders, including preeclampsia.4 The possible pathophysiologic mechanism of OSA on preeclampsia is that intermittent hypoxia induces endothelial dysfunction and vasoconstriction.5 This mechanism was verified using a hypoxia-induced preeclampsia mouse model in which a hypoxic environment increased blood pressure and proteinuria.6
Obesity is one of the significant risk factors for pregnancy-related adverse outcomes.7 Also, obesity and hypertension are associated with OSA in the general population.89 Previous studies demonstrated that maternal obesity is strongly related to OSA during pregnancy, particularly in the third trimester.10 However, another study demonstrated that there was no significant difference in the respiratory disturbance index between normotensive and hypertensive pregnant women with similar body mass index (BMI).11 A BMI-matched study with pregnant and non-pregnant women also showed that OSA prevalence was not different between the two groups, and the suspected reason for this was most participants were not obese.12 Collectively, it remains still controversial whether OSA affect the development or aggravation of hypertensive disorders in pregnancy, including preeclampsia.
However, OSA is still lacking in diagnosis and understanding in pregnant women. Previously reported prevalence of OSA in pregnant women varies according to race, body weight, and timing of the polysomnography (PSG) test. Few studies have been conducted on the association of OSA and pregnancy-related outcomes in Asians, particularly in Korea.1314 Although obesity in women of childbearing age has been increasing, Koreans still have lower BMI values compared to Western pregnant women.1516 For this reason, we assumed that the prevalence of OSA and that of obesity would be relatively low in general pregnant women and planned to evaluate OSA in overweight pregnant women during the third trimester. Weight gain during the third trimester exaggerated compared to that in the first and second trimesters, and OSA might worsen as the gestational weeks progress.7 Many studies have evaluated the association between OSA and hypertensive disorders in pregnancy, whereas the causality or chronology has not been elucidated. Usually, early-onset preeclampsia, with onset before 34 weeks, has a higher risk of fetal growth restriction, cardiovascular disease, and other maternal morbidities compared to late-onset preeclampsia.1718 OSA is aggravated during the late phase of pregnancy due to weight gain, which may cause or worsen late-onset preeclampsia, but no previous study evaluates this relationship.
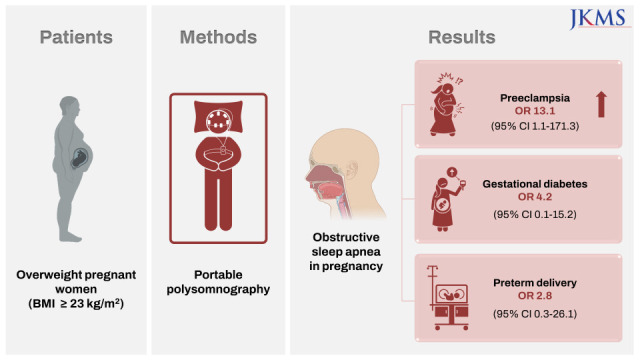
This prospective cohort study aimed to evaluate the prevalence of OSA in pregnant women who were overweight in the third trimester and to elucidate the effects of OSA on pregnancy-related complications, especially late-onset preeclampsia. We also compared the concentration of serum biomarkers related to preeclampsia and those of OSA between pregnant women with and without OSA. Some part of this study was previously published as an abstract.19
METHODS
Study Subjects
This prospective cohort study was conducted in a tertiary referral hospital from June 2017 to December 2018. Pregnant women were enrolled who met the following criteria: 1) older than 19 years, 2) gestation over 30 weeks; 3) overweight (BMI ≥ 23 kg/m2 according to the Asia-Pacific regional guidelines of the WHO guidelines)15; and 4) singleton pregnancy.
Polysomnography
Testing for OSA was performed in all participants using at-home portable PSG with WatchPAT (Itamar Medical, Caesarea, Israel). Test results were assessed by an otolaryngologist within two weeks of study enrollment. Apnea-hypopnea index (AHI), respiratory disturbance index, and oxygen saturation were reviewed as previously reported.20 OSA was defined as AHI ≥ 5 and normal control was defined as AHI < 5.
Clinical parameters
We prospectively collected data from pregnant women, including age, body weight, height, BMI, parity, history of spontaneous abortion, mode of delivery, and gestational complications (GDM, preeclampsia, or preterm delivery). Preeclampsia was diagnosed when a pregnant woman developed a blood pressure > 140/90 mmHg and proteinuria > 300 mg in a 24-hour urine collection after 20 weeks’ gestation.21 The Berlin questionnaire was administered at study enrollment and consists of three categories related to risk of sleep apnea. Scoring can be classified into high risk or low risk groups according to the patient’s symptoms. Clinical information about the infants was collected, such as body weight at birth, Apgar scores at one and five minutes, and perinatal complications.
Blood test
The patient’s whole blood was collected at the time of enrollment. Blood samples were centrifuged, and separated serum were stored at −80ºC until analysis of enzyme-linked immunosorbent assay (ELISA). We measured serum markers related to preeclampsia,22 such as serum soluble fms-like tyrosine kinase-1 (sFlt-1; MBS262972-96T, MyBiosource, San Diego, CA, USA), endoglin (DNDG00, R&D Systems, Minneapolis, MN, USA), and placental growth factor (PlGF; LS-F1231, LSBio, Seattle, WA, USA). Biomarkers of OSA were evaluated, including interleukin (IL)-6 (D6050, R&D Systems), myeloid-related protein (MRP)8/14 (439707, Biolegend, San Diego, CA, USA), and tumor necrosis factor (TNF)-α (DTA00D, R&D Systems).23
Statistical analysis
Data were presented as median with interquartile range. Continuous variables were analyzed using the Mann-Whitney test and categorical variables were tested by Fisher’s exact test, respectively. Logistic regression models were used for calculating odds ratio (ORs) and 95% confidence intervals (CIs) to determine the association between OSA and pregnancy-related complications. Models were adjusted for BMI, maternal age, parity, and history of spontaneous abortion. Stata software v16.0 (StataCorp LP, College Station, TX, USA) was used.
RESULTS
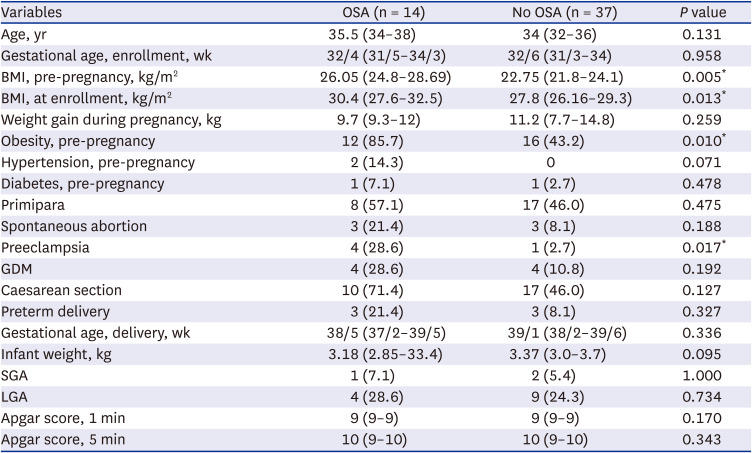
Of a total of 137 pregnant women were screened, 51 (37.2%) were enrolled in the study and completed a PSG, while 80 women (58.4%) refused to participate in the study and six (4.4%) were dropped from the study due to various reasons. The mean age of participants was 34.5 years (27–44 years), and the mean gestational age was 32/6 weeks (range of 30/1–37/2 weeks). Of these, the number of primipara was 25 (49%) and that of multipara was 26 (51%). Eight patients were diagnosed as having GDM (15.7%), five had preeclampsia (9.8%), and six experienced preterm delivery (11.8%). Five patients were diagnosed with preeclampsia after study enrollment. Among them, three patients already had pregnancy-induced hypertension. Two patients had previously been diagnosed with hypertension before pregnancy, one of whom developed preeclampsia. Two patients had overt diabetes before pregnancy, and diabetes persisted during pregnancy. After PSG, 14 of the pregnant women (27.5%) were diagnosed OSA. The demographics between pregnant women with (OSA group) and without OSA (control group) are presented in Table 1. The BMI was higher in the OSA group before pregnancy (P = 0.005) and at enrollment (P = 0.013) compared to the control group. Preeclampsia was more frequently observed in the OSA group compared to the control group (P = 0.017).
Table 1
Comparison of demographic characteristics between pregnant women with obstructive sleep apnea and controls
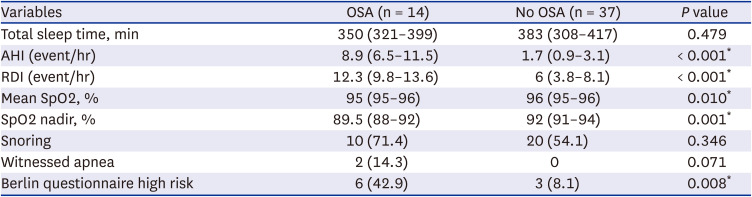
Fourteen women with OSA were categorized according to severity of AHI, which were comprised of 12 cases of mild (5 ≤ AHI < 15), one of moderate (15 ≤ AHI < 30), and another of severe OSA (AHI ≥ 30) (Fig. 1A). In all subjects, AHI was well correlated with BMI at enrollment (r = 0.515, P < 0.001, Fig. 1B), whereas the correlation between AHI and age was not significant (r = 0.177, P = 0.215, Fig. 1C). Sleep parameters, including respiratory disturbance index, mean oxygen saturation (SpO2), and SpO2 nadir, were significantly different between the OSA and control groups (Table 2). Using the Berlin questionnaire for evaluating high risk of OSA, nine pregnant women (17.6%) were at high risk, and six of them were diagnosed with OSA by portable PSG. The remaining eight OSA patients at low risk according to the Berlin questionnaire had no subjective symptoms such as snoring, witnessed apnea, or fatigue.
Fig. 1
OSA evaluated by portable polysomnography in pregnant women. (A) The percentage of OSA patients according to AHI. (B) Correlation analysis between AHI and BMI at enrollment. (C) Correlation analysis between AHI and age at enrollment.
AHI = apnea-hypopnea index, BMI = body mass index, OSA = obstructive sleep apnea.
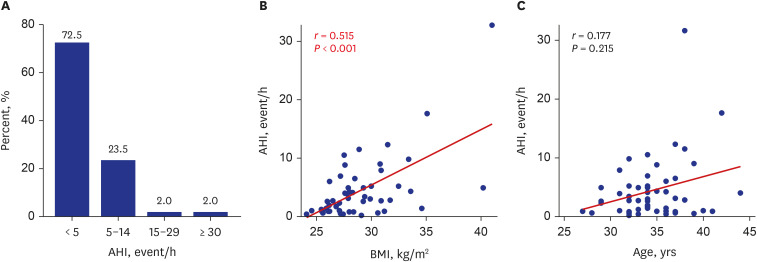
Table 2
Polysomnographic sleep characteristics and Berlin questionnaire results between pregnant women with obstructive sleep apnea and controls
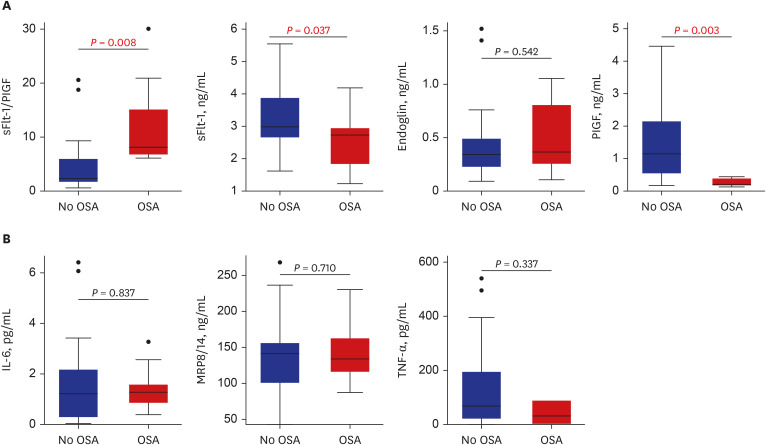
Additionally, we analyzed serum markers related to preeclampsia and OSA (Fig. 2A and B). The serum sFlt-1/PlGF ratio, the clinically used serological marker for predicting preeclampsia,22 was significantly elevated in the OSA group compared to the control group (12.0 ± 8.7 vs. 5.3 ± 6.5, P < 0.008). The ratio of sFlt-1/PlGF was higher in the four patients with preeclampsia than in those without preeclampsia (16.8 ± 10.8 vs. 5.7 ± 5.8, P < 0.019). Other proinflammatory markers, such as IL-6, MRP8/14, and TNF-α, were not different between the two groups (Fig. 2B).
Fig. 2
Comparison of serum markers between OSA patients and controls. (A) Preeclampsia-related markers; sFlt-1/PlGF ratio, sFlt-1, Endoglin, and PIGF. (B) Proinflammatory markers for OSA; IL-6, MRP8/14, and TNF-α.
sFlt-1= soluble fms-like tyrosine kinase-1, PlGF = placental growth factor, OSA = obstructive sleep apnea, IL = interleukin, MRP = myeloid-related protein, TNF = tumor necrosis factor.
Pregnant women with OSA had increased risk of preeclampsia, and the unadjusted OR was 14.4 (95% CI, 1.4–143.7). The OR remained high (OR, 11.1; 95% CI, 1.1–116.4) after adjusting for pre-pregnancy BMI (Table 3). We calculated adjusted ORs with adjustment for pre-pregnancy BMI, age, parity, and abortion history. OSA was strongly related to increased OR of preeclampsia (OR, 13.1; 95% CI, 1.1–168.0).
Table 3
Odds ratios and 95% confidence intervals for the association between obstructive sleep apnea and pregnancy-related outcomes

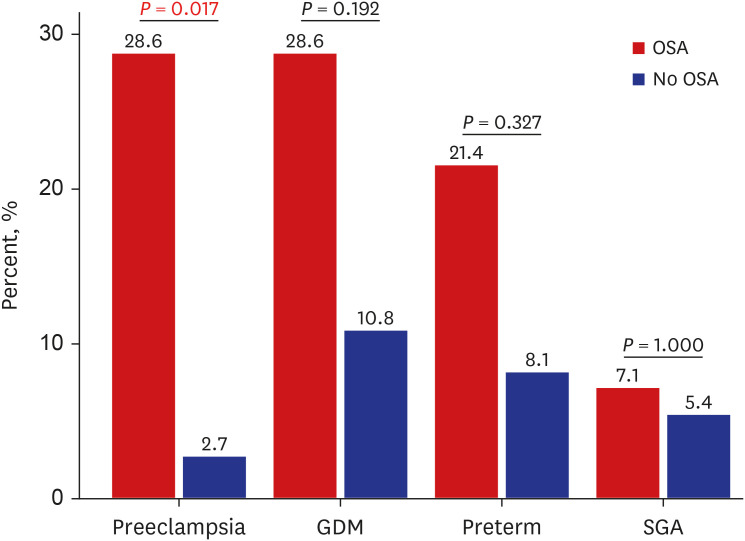
All preeclampsia patients underwent cesarean section, four patients experienced preterm delivery, three had comorbid GDM, and four were diagnosed with OSA. OSA was prevalent in patients with pregnancy-related adverse outcomes, such as preeclampsia, GDM, preterm delivery, and small for gestational age neonates (Fig. 3) Taken together, these findings indicate that OSA is associated with pregnancy-related complications, and that such complications affect one other.
DISCUSSION
This is the first study to diagnose OSA in pregnant women using portable PSG in Korea. We found that the prevalence of OSA was 27.5% in overweight (BMI ≥ 23) pregnant women over 30 weeks of gestational age. Between pregnant women with and without OSA, BMI was higher and comorbid preeclampsia was prevalent in the OSA group. When adjustment was made for pre-pregnancy BMI, age, parity, and abortion history, OSA was related to increasing risk of preeclampsia. According to previous studies, OSA increased the odds of preeclampsia (OR, 2.5; 95% CI, 2.2–2.9), as shown in a nationwide database in the USA,2 and maternal sleep-disordered breathing was associated with gestational hypertension or preeclampsia (pooled adjusted OR, 2.34; 95% CI, 1.60–3.09) in a systematic review.24 In a study conducted with the International Classification of Diseases (ICD)-9 code in Taiwan, the same Asian country, the odds ratio of OSA for preeclampsia was 1.6.25 The possible reason for the difference from our study (OR, 13.1) is that the PSG was performed at a different time. The previous study defined OSA patients with two or more OSA diagnosis after PSG within one year prior to index delivery. However, since this study was conducted with women over 30 weeks pregnant, factors that may affect the occurrence of OSA, such as weight gain during pregnancy, may have been reflected.
Pamidi et al.10 reported that pregnant women diagnosed with OSA had increased risk of small for gestational age neonates. Contrarily, an Australian population-based study found that OSA was associated with large for gestational age infants (OR, 1.27; 95% CI, 1.04–1.55).26 The relationship between OSA and GDM in pregnant women has varied in several studies.1242627 In the present study, other pregnancy-associated disorders were also related to OSA but did not reach statistical significance. A recent long-term cohort study with nulliparous found that OSA (AHI ≥ 5) during pregnancy was associated with an increased risk of hypertension at 2–7 years after delivery.28 Taken together, OSA in pregnancy is strongly related with adverse outcomes for both mother and fetus in the short and long term.
We performed portable PSG to evaluate OSA in pregnant women. The criterion standard for diagnosing OSA is level 1 attended PSG,29 whereas it is very difficult for pregnant women in the third trimester to be tested with full PSG in a sleep laboratory. Some of the previous studies used at-home portable PSG for convenience of the subjects who are pregnant.1030 Portable PSG based on peripheral arterial tonometry was validated, and respiratory indexes of portable PSG were well correlated with those of level 1 PSG.2031 PSG is reimbursed by the National Health Insurance for the general population,32 but there are no standard for the PSG test in pregnant women.
We additionally evaluated the risk of OSA using the Berlin questionnaire. In this study cohort, 6 out of 14 OSA patients (42.9%) were identified as high-risk in the Berlin questionnaire, and most of the confirmed OSA cases were mild (12/14, 85.7%). The sensitivity of Berlin questionnaire was reported to be 61.3% in Korean population, and this questionnaire is useful for screening for moderate to severe OSA.33 An accuracy of subjective symptom screening for sleep disordered breathing through administration of a questionnaire has been debated, especially in patients with asymptomatic or mild OSA. Objective measurement of OSA using PSG was strongly associated with small for gestational age infants, while subjective symptoms evaluated by a sleep questionnaire were not related to the outcome.10 Even in asymptomatic or mild OSA patients, there was increased risk of worse pregnancy-related outcomes. Therefore, objective PSG testing is required for pregnant women who are overweight or at high risk of hypertensive disorders in pregnancy.
Considering that the association between obesity and preeclampsia is stronger in late-onset preeclampsia.10 We enrolled our study population after 30 weeks gestational and who had regular visits until delivery. Therefore, some cases with early-onset preeclampsia or severe hypertension requiring hospitalization were not included. There is little information on the relationship between the causes and effects of OSA and preeclampsia, but it is well known that OSA causes hypertension in the general population.834 Serum analysis revealed that the sFlt-1/PlGF ratio was higher in OSA patients compared to pregnant women without OSA. In OSA patients without preeclampsia, the mean level of sFlt-1/PlGF was elevated over the normal controls. This finding suggests that OSA-induced intermittent hypoxia might play a part in the pathogenesis of preeclampsia. The sFlt-1/PlGF ratio was determined by a laboratory-based ELISA in this study.22 This value may differ from the electrochemiluminescence immunoassay, which is measured with automated device used in clinical practice.35
The present study has some limitations. First, more than half of the pregnant women asked to participate declined because they were reluctant to join clinical studies, being subject to a selection bias in which pregnant women with more severe sleep apnea are selected. Due to the relatively small number of sample size, no significant results were drawn for other pregnancy-associated outcomes, and any subgroup analyses were possible including pre-pregnancy obesity, hypertension, diabetes, or other metabolic diseases. Second, we prescribed a portable PSG instead of an attended level 1 PSG, limiting comprehensive information regarding whole sleep quality. Lastly, there were a few patients with hypertension or diabetes before pregnancy, but the numbers were too small to evaluate the actual impact.
However, to our knowledge, it has never been investigated in Korean pregnant women. The novelty of the present study is that we performed a comprehensive survey of PSG and questionnaires in this prospective cohort. We also checked the levels of serum markers related to preeclampsia including sFlt-1, PlGF, and endoglin and biomarkers of OSA (IL-6, MRP8/14, and TNF-α) according to the presence or absence of OSA. High BMIs were associated with OSA in the third trimester of pregnancy. We confirmed that OSA was a significant and independent risk factor for preeclampsia and was associated with preterm delivery. Collectively, our data suggest that OSA work-up is considered as mandatory for pregnant women who are overweight or have hypertensive disorder of pregnancy. These results also imply that management of OSA in pregnant women may prevent late-onset preeclampsia. Further mechanistic studies about the relationship between OSA and preeclampsia are warranted.
 XML Download
XML Download