

 PDF
PDF Citation
Citation Print
Print



CASE PRESENTATION
Dr. Donghan Lee: A 27-year-old woman was admitted to our hospital after one day of dysarthria and right arm weakness. The patient had been healthy until one day before admission and was not taking any medications. She denied tobacco use, heavy alcohol consumption, oral contraceptive use, or illicit drug use. The clinical examination was notable for a blood pressure of 215/136 mmHg, a heart rate of 91 beats per minute, a temperature of 37.3ºC, and an oxygen saturation of 98% on room air. The patient’s height was 170 cm, while her weight was 75 kg and her body mass index (BMI) was 26. An electrocardiogram showed that she was in a sinus rhythm. Her right arm motor strength was reduced, but movement against resistance was possible (modified Medical Research Council grade IV).
Laboratory results were notable for an activated partial thromboplastin time (aPTT) of 43.9 seconds (reference range: 22–33) and a serum potassium level of 3.3 mEq/L (reference range: 3.5–5.1). Blood levels of albumin, total cholesterol, low-density lipoprotein cholesterol (LDL-C), and glycated hemoglobin were normal, as were the complete blood count with differential and the results of liver function, kidney function, and thyroid function tests. Urine human chorionic gonadotropin was undetectable, and urinalysis showed 3+ protein, no blood, and no cast.
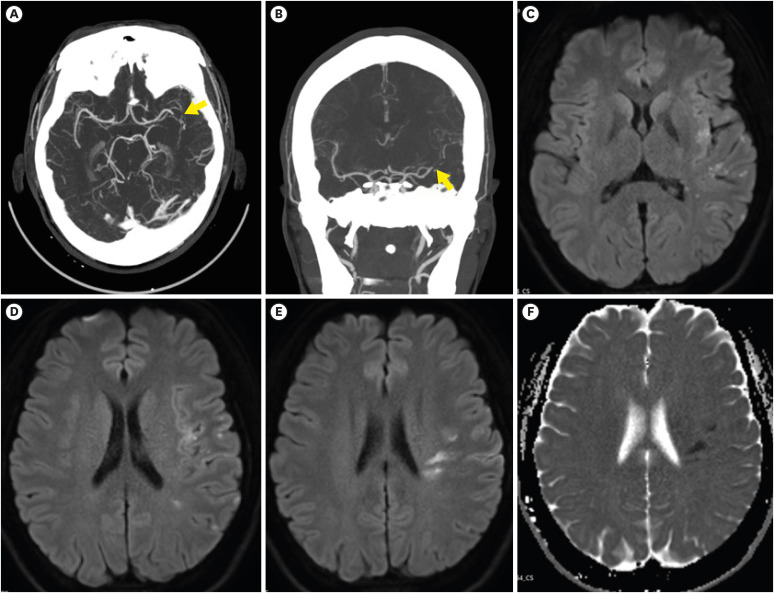
Dr. Hae-Eun Shin: Computed tomography (CT) angiography of the head and neck (Fig. 1A and B) revealed focal occlusion of the proximal M2 segment superior division of the left middle cerebral artery (MCA). Magnetic resonance imaging (MRI) of the brain was performed, and diffusion-weighted images showed multi-fragmented restricted diffusion involving the left MCA territory, including the insular cortex and the frontal and temporal lobes (Fig. 1C and F). The patient’s score on the National Institutes of Health Stroke Scale (NIHSS) was 2 (range: 0–42). The patient was not within the therapeutic window for systemic thrombolysis or endovascular intervention, so aspirin, clopidogrel, and atorvastatin were administered.
Fig. 1
Neuroimaging studies. An initial computed tomography angiography of the head shows focal occlusion (arrow) of the left middle cranial artery proximal M2 superior division (A: axial image and B: coronal image). Magnetic resonance imaging of the head was also performed, and axial diffusion-weighted images (C–E) and the apparent diffusion coefficient (F) show multiple small areas of restricted diffusion in the left MCA territory, suggestive of an acute infarction.
DIFFERENTIAL DIAGNOSIS
Dr. Jung Hee Koh: This patient was younger than 50 years of age and presented with ischemic stroke and hypertension. For differential diagnosis, a comprehensive stroke evaluation and analysis for a secondary cause of hypertension were initiated. The use of oral contraceptives containing estrogen, pregnancy, and migraine with aura are risk factors unique to young women.1 Particularly among younger stroke patients, there is a greater prevalence of patent foramen ovale and inherited and acquired thrombophilias.1 Inherited thrombophilias (including Factor V Leiden mutations and prothrombin G20210A gene mutations) are rare among Asians.2 Thrombophilias in Asian individuals are mainly due to activated protein C (APC) dysfunction, whereas the major cause in Caucasians is an APC-resistant anticoagulant system.3 Antiphospholipid syndrome (APS) is an autoimmune disease defined by thrombotic or obstetrical events that occur in patients with persistent antiphospholipid (aPL) antibodies.4 APS accounts for 10–20% of strokes in young patients.5 APS is often associated with systemic lupus erythematosus (SLE), and individuals with SLE have a twofold higher risk of ischemic stroke compared to the general population.6
Hyperhomocysteinemia also causes abnormal blood clotting and can result from a genetic mutation, as well as deficiencies of folate and vitamins B6 and B12.1 Several rare conditions affecting the arteries (such as Fabry disease, reversible cerebral vasoconstriction syndrome, Moyamoya disease, Takayasu’s arteritis, and fibromuscular dysplasia) are other causes of stroke in younger adults.1
Howook Jeon: As this patient was obese (BMI > 25 kg/m2), severe hypertension (> 180/110 mmHg) was noted despite her young age (< 30 years) and persisted. Renal parenchymal disease and renovascular disease are common causes of secondary hypertension.7 Primary aldosteronism, Cushing Syndrome, and pheochromocytoma are other causes of secondary hypertension in the young population.
PATHOLOGICAL FINDINGS
Dr. Donghan Lee: Initial laboratory tests revealed a prolonged aPTT with a normal prothrombin time. Common causes of isolated aPTT include the presence of lupus anticoagulant, heparin administration, and deficiencies of specific coagulation factors.8 In this patient, the presence of lupus anticoagulant was confirmed when aPTT shortened after addition of 2.24-fold phospholipid. Further testing revealed elevated levels of anticardiolipin IgG and anti-β2-glycoprotein 1 IgG. Taken together, these results constitute “triple positive” aPL findings, the most likely explanation of this patient’s prolonged aPTT. To meet the laboratory criteria for APS, either lupus anticoagulant, anticardiolipin, or β2-glycoprotein 1 antibodies should be present at least 12 weeks after initial measurement.9
An anti-nuclear antibodies (ANAs) test was positive at a titer of 1:400 with a speckled pattern. The complement 3 (C3) level was 85 mg/dL (reference range: 90–180), while the C4 level was within the normal range. The 24-hour urine protein level was 0.588 g/day. Tests for anti-double stranded DNA, anti-Smith, anti-Ro, and anti-RNP antibodies were negative. The patient reported non-pruritic macular rashes on both cheeks associated with photosensitivity, which persisted for several weeks.
An abdominal CT with intravenous contrast media was carried out to assess stenosis of the renal arteries or adenomas or hyperplasia of the adrenal glands. A 7-mm hypodense nodule was found in the left adrenal gland. The plasma aldosterone-to-renin ratio was 3.69 (reference range: 0–30). The 24-hour urinary free cortisol excretion level was 62.7 μg/day (reference range: 13.8–75.3); the 24-hour urine free metanephrine was 55 μg/day (reference range: < 320), while the plasma fractionated metanephrine was 0.08 nmol/L (reference range: < 0.33). During the work-up, intravenous perdipine was administered as an anti-hypertensive agent.
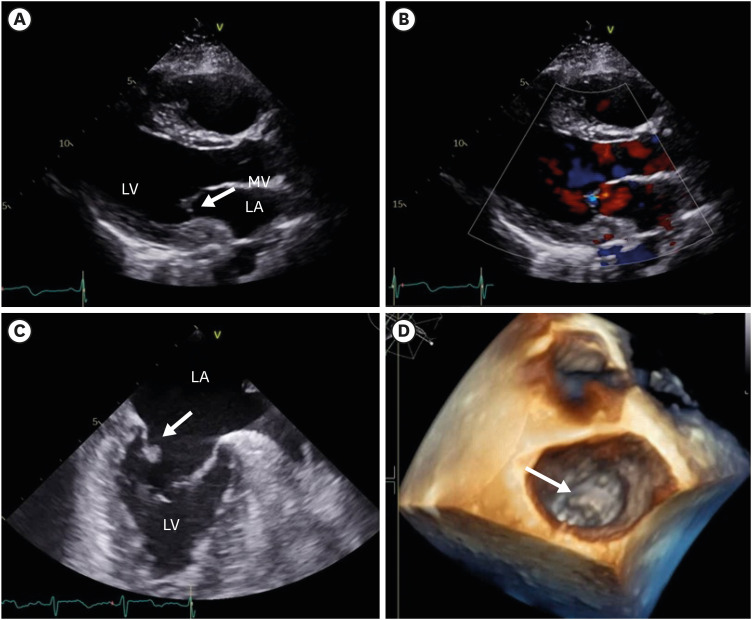
Yuran Ahn: This patient did not show arrythmia on Holter monitoring. Echocardiography is an important diagnostic tool in patients with cryptogenic embolic stroke and suspected secondary hypertension. On the sixth hospital day, a transthoracic echocardiogram showed a trivial mitral valve regurgitation (Fig. 2A and B and Supplement Video 1); however, patent foramen ovale or intracardiac thrombosis were not found. Upon transesophageal echocardiography (TEE), 0.4 × 0.6-cm vegetation was observed on the atrial side of the mitral valve posterior leaflet (Fig. 2C and D, Supplementary Videos 2 and 3). Blood cultures were obtained, but no microorganism was identified.
Fig. 2
Echocardiograms. On transthoracic echocardiography, a paraspinal long-axis view shows a normal mitral valve (A) and trivial mitral regurgitation (B). Transesophageal echocardiography in mid-esophageal 88-degree two chamber view; the arrow points to vegetation on the mitral valve posterior leaflet (C). Three-dimensional transesophageal echocardiography showing the mass on the mitral valve leaflet (D, arrow).
DIAGNOSIS
Dr. Howook Jeon: A malar rash, photosensitivity, proteinuria, a low blood level of C3, ANA at a titer of 1:400, and the presence of anti-phospholipid antibodies support the diagnosis of SLE. To date, APS had not been diagnosed because persistent aPL antibodies were not confirmed in a repeated test.
Dr. Yuran Ahn: The valvular vegetations present in the context of negative blood cultures and no clear signs of infection are suggestive of nonbacterial thrombotic endocarditis. Considering all features, this patient most likely has Libman-Sacks endocarditis associated with APS and SLE.
Dr. Jung Hee Koh: This patient presented with neuropsychiatric SLE (NPSLE) of the central nervous system. The underlying pathophysiological mechanisms were suggestive of a hypercoagulable state secondary to APS as well as cardioembolic disease secondary to Libman-Sacks endocarditis.
DISEASE MANAGEMENT
Hydroxychloroquine (HCQ) was initiated to treat SLE. HCQ is recommended for all patients with SLE, unless contraindicated.10 Observational studies have shown that HCQ is associated with increased survival, reduced disease activity, prevention of organ damage, and a reduced risk of thrombosis in patients with SLE.11 The prevention of thrombosis seems to be associated with reduction in platelet activation and increased endothelial dysfunction.12 Concerns for retinal toxicity with long-term HCQ therapy have led to the use of a daily dosage of HCQ not to exceed 5 mg/kg/real body weight, as well as special ophthalmological screening.10
Treatment for NPSLE depends on whether the underlying pathophysiological mechanism is presumed to be inflammatory or embolic/thrombotic/ischemic.10 Glucocorticoids and/or immunosuppressants can be considered in the former, while anticoagulant/antithrombotic treatment is favored in the latter.10 However, distinguishing between these two pathophysiological processes may be difficult in real-world practice, and it is possible for the two processes to coexist in the same patient.10 Acute ischemic stroke treatment is similar to that administered to patients without SLE. Patients should be carefully assessed to determine if they are eligible for fibrinolysis and/or surgical treatment.13 For secondary prevention of ischemic stroke, oral anticoagulation is indicated in patients with SLE who have suffered a previous stroke and have persistent moderate-high positive titers of anti-phospholipid antibodies. The best treatment option is antivitamin K anticoagulant (warfarin) and low-molecular weight heparin.13 Thus, this patient started warfarin with a target international normalized ratio (INR) between 2 and 3 along with low-molecular weight heparin. Because her LDL-C level was 129 mg/dL at admission, atorvastatin was also initiated.14 In addition, olmesartan was administered to decrease blood pressure and reduce the risk of stroke recurrence.
No specific therapy is indicated for Libman-Sacks endocarditis. In cases of significant valvular dysfunction, surgical decisions should be made according to established guidelines for valvular heart disease. For secondary prevention, anticoagulation is often indicated for atrial fibrillation, mitral stenosis, mechanical heart valves, and thromboembolic events.1516
DISCUSSION
Management of stroke prevention
Dr. Hwa Jung Kim: Why was warfarin initiated in this case? Direct-acting oral anticoagulants (DOACs) are oral direct factor Xa inhibitors and direct thrombin inhibitors that have demonstrated superiority or noninferiority to anticoagulation with vitamin K antagonists or low-molecular weight heparins in reducing risk of thromboembolic complications with similar or reduced bleeding risk.17 Recently, DOACs have been widely used to lower the risk of stroke and embolism in patients with atrial fibrillation, as well as deep vein thrombosis and pulmonary embolism treatment and prophylaxis.17
Dr. Jung Hee Koh: However, the use of DOACs is contraindicated in some patients, including those with a mechanical prosthetic valve, moderate to severe mitral stenosis, and triple positive aPL antibodies.141718 A recent randomized controlled trial of rivaroxaban versus warfarin in patients with APS with triple positive aPL antibodies was terminated early due to an excess of thromboembolic events (mostly arterial) in the rivaroxaban arm.18 Thus, rivaroxaban should not be used in patients with triple aPL positivity.1418
Persistent detection of aPL (measured on two or more occasions at least 12 weeks apart) is important to diagnose APS because transient presence of epiphenomenal aPL can lead to misdiagnosis.9 This patient presented with a triple positive aPL profile with very high titers, which is considered high risk for thrombotic events.18 Moreover, this patient was comorbid for Libman-Sack endocarditis, which is considered an aPL-associated cardiac valve disease.9 Therefore, warfarin is likely to provide good prevention from recurrent thromboembolism.
Libman-Sacks endocarditis in APS and SLE
Dr. Howook Jeon: When should Libman-Sacks endocarditis be suspected in APS or SLE patients? After diagnosis and treatment, what is the prognosis for Libman-Sacks endocarditis?
Dr. Jung Hee Koh: Libman-Sack endocarditis is a characteristic valvular abnormality seen in SLE as well as APS patients. On TEE, the prevalence of valvular abnormalities is 61% in patients with SLE compared with 9% of controls, and vegetations are present in 43% of patients with SLE compared with none of the controls.19 The presence and progression of valvular disease were not associated with SLE disease activity or treatment. In contrast, the presence of valvular abnormalities in SLE is associated with aPL; patients with SLE and aPL were three times more likely to be diagnosed with these abnormalities than SLE patients without aPL.20 TEE is superior to transthoracic echocardiography for detection of Libman-Sacks endocarditis.21 Therefore, TEE should be used in the event of a nondiagnostic transthoracic echocardiography or in a patient with suspected thromboembolic events.
As Libman-Sack endocarditis is a rare manifestation of SLE or APS, there is no consensus for the best methods of treatment and follow-up in these patients. In a recent longitudinal and cross-sectional study, patients with SLE and Libman-Sacks endocarditis complicated by embolic cerebrovascular disease were treated with conventional anti-inflammatory and anti-thrombotic therapy for six months; on the follow-up TEE, 76% of the patients experienced resolved or improved valvular vegetation or regurgitation.22 In another six-year longitudinal and cross-sectional study, 16% of patients had new or recurrent stroke, 14% had cognitive disability, and 9% died.16
PROGNOSIS
Dr. Howook Jeon: On the eighth hospital day, the patient’s symptoms of dysarthria and weakness in the right arm had improved. The NIHSS score was 0. Laboratory tests revealed that the proteinuria and hypokalemia had resolved, and the INR of prothrombin time was 2.02. The patient was discharged home. A repeated test for aPL antibodies after 12 weeks was persistently triple positive. She continues to receive warfarin and HCQ.
LEARNING POINTS
1. Physicians should consider APS in the differential diagnosis when a young female patient presents with a thromboembolic event and an isolated prolonged aPTT.
2. Identifying the presence of factors associated with a high risk for thrombotic events is critical in the management of APS. A major risk factor is a high-risk aPL profile, including the presence of lupus anticoagulant, double or triple aPL positivity, or persistently high aPL titers. Anticoagulation with a vitamin K antagonist or low-molecular weight heparin is the cornerstone of secondary prevention of stroke in APS patients with a high-risk aPL profile.
3. Libman-Sack endocarditis is a cardiac manifestation of SLE and APS, and TEE is the gold standard for diagnosis.

 XML Download
XML Download