

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
On a global scale, the World Health Organization recently published statistics revealing that 625,248,843 infections and 6,562,281 deaths have occurred owing to coronavirus disease 2019 (COVID-19) as of October 26, 2022.1 In its official statistics, the Korea Disease Control and Prevention Agency (KDCA) states the number of confirmed cases as 25,538,799 over four disease surges since January 2022, as of October 30, 2022.2 Concordant with the worldwide situation, the omicron variant is the dominant severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) variant in Korea, whereas subvariant BA 5 is contributing to 95% of isolated SARS-CoV-2 cases as of October 2022.3
The symptoms of COVID-19 can range from asymptomatic to severe respiratory failure. Mild-to-moderate COVID-19 can cause respiratory and systemic symptoms except for hypoxia or other hospitalization-required complications.4 Thus, patients with mild-to-moderate COVID-19 can usually recover at home, whereas those at a high risk of complications or disease progression need to be more diligent.45 For patients with increased risks of severe disease, antiviral therapy is the only option that can prevent hospitalization and disease progression and is recommended in most current guidelines for COVID-19 management.678
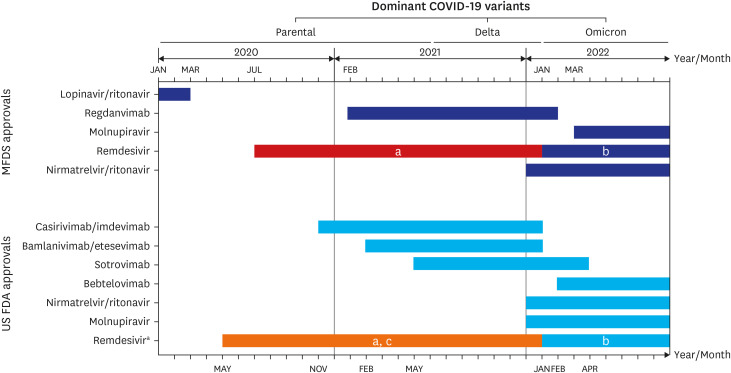
Antiviral therapies are mainly used to prevent disease progression, hospitalization, and death for patients with mild-to-moderate COVID-19. Antiviral agents can help to suppress the viral replication of SARS-CoV-2 and its related inflammatory responses, which are dominant in the early phases of COVID-19 with a mild-to-moderate degree of disease.59 Unfortunately, despite many clinical trials investigating new or repurposed antiviral agents, there is no curative therapy for COVID-19. Although several repurposed agents, such as hydroxychloroquine, favipiravir, lopinavir/ritonavir, sofosbuvir/daclatasvir, fluvoxamine, and enisamium, have entered clinical trials since they showed in vitro antiviral effects, only a few agents have been approved for the treatment of patients with COVID-19 (Fig. 1).101112
Fig. 1
The timeline of antivirals approval in Korea and the United States. There is no available monoclonal antibody for COVID-19 in Korea.
COVID-19 = coronavirus disease 2019, MFDS = Korean Ministry of Food and Drug Safety, US FDA = United States Food and Drug Administration.
aRemdesivir was approved only for the treatment of moderate to severe COVID-19 in this period.
bThe indications of remdesivir was broaden to the outpatient setting.
cDefinitive approval of remdesivir occurred in October 2020 by US FDA.
In this review article, we summarize the available antiviral therapies for patients with mild-to-moderate COVID-19 and discuss changes in therapy use in clinical practice and recommendations based on the results of domestic studies in Korea.
ANTIVIRAL TREATMENT OPTIONS
Remdesivir
Remdesivir, an RNA-dependent RNA polymerase inhibitor, was initially developed to treat Ebola viral infections. It was the first authorized antiviral for emergency use in patients with COVID-19 in several countries. Remdesivir has been shown to improve clinical outcomes in patients hospitalized with moderate-to-severe disease.13
In Korea, remdesivir was rolled out under emergency use authorization by the Korean Ministry of Food and Drug Safety (MFDS) on July 1, 2020.14 Despite controversy over the effectiveness of Remdesivir in reducing patient mortality based on several studies, it has been recommended for treating patients with moderate-to-severe COVID-19 who require oxygen therapy since the early stages of the COVID-19 pandemic in Korea.61115 In a domestic retrospective cohort study reported in March 2021, the proportion of patients requiring mechanical ventilation was lower (22.9% vs. 44.7%, P = 0.032) for patients on remdesivir compared to those received a placebo, and the duration of mechanical ventilation was also shorter (average, 1.97 vs. 5.37 days; P = 0.017).16 However, remdesivir was not approved for mild-to-moderate cases until January 2022 because of the lack of studies.
On January 20, 2022, MFDS broadened the use of remdesivir to patients aged ≥ 18 years with mild-to-moderate COVID-19 who are at high risk of progression to severe illness. This approval was based on the results of the GS-US-540-9012 (PINETREE) clinical trial, which was announced on December 22, 2021.17 In the clinical trial, the efficacy of Remdesivir was evaluated in non-hospitalized patients with mild-to-moderate COVID-19 at high risk of disease progression.1819 When remdesivir was administered to patients for 3 days, within 7 days from the illness onset, the risk of hospitalization or death decreased by 87% compared with that in the placebo group.18
As an advantage, considering the mechanism of action of remdesivir and its safety profile, the clinical role of this agent is unlikely to be influenced by spike protein mutations, such as those in the omicron variant and its subvariants. Remdesivir can thus be a useful therapeutic option for reducing hospitalization and severe illness regardless of spike protein mutation status.
Ritonavir-boosted Nirmatrelvir
Nirmatrelvir/ritonavir is co-formulated with nirmatrelvir and ritonavir to achieve a therapeutic level of nirmatrelvir by CYP3A metabolism inhibition.20 In a phase 2/3 clinical trial, non-hospitalized patients at high risk of COVID-19 progression but still in the early stage of disease (within 5 days of symptom onset) had 88% reduction in hospitalization or death when treated with nirmatrelvir/ritonavir compared with the placebo group.21 Based on the data, the United States Food and Drug Administration (US FDA) approved the agent for treating mild-to-moderate COVID-19 in adult and pediatric patients (age ≥ 12 years and body weight ≥ 40 kg) on December 22, 2021.22
MFDS approved Nirmatrelvir/ritonavir for the treatment of COVID-19 patients on December 27, 2021.23 However, it has not been widely used in the clinic, and real-world data on the agent’s effectiveness is yet to be determined in Korea, despite showing favorable clinical trial results for preventing disease progression in patients with mild-to-moderate COVID-19. A domestic study conducted on patients and healthcare workers residing in long-term care facilities reported 51% reduction in the rate of severe illness or death in the Nirmatrelvir/ritonavir-administered group compared with the untreated group.24 Participants in the same study who completed three doses of COVID-19 vaccination had 71% reduction in the rate of severe illness and 65% reduction in the risk of death compared with vaccine naïve participants.24
There are limitations in prescribing nirmatrelvir/ritonavir. Nirmatrelvir/ritonavir can increase the toxicity of many medications, such as anti-arrhythmic agents, including amiodarone, rifampin, statins, or rivaroxaban, because ritonavir is a well-known CYP3A inhibitor.22 Accordingly, clinicians should consult with an experienced pharmacist before prescribing nirmatrelvir/ritonavir to a patient taking other medications. Clinicians should also not prescribe Nirmatrelvir/ritonavir for patients with severe renal (estimated glomerular filtration rate < 30 mL/min) or liver dysfunction (Child-Pugh class C).22 These two limitations present significant hurdles to the appropriate use of nirmatrelvir/ritonavir in patients in Korea.
Molnupiravir
Molnupiravir is a prodrug of a nucleoside analog inhibiting viral RNA-dependent RNA polymerase that was initially developed against influenza.2526 A phase 2a clinical trial of molnupiravir showed an acceleration of SARS-CoV-2 RNA clearance and virus elimination in COVID-19 patients.27 In a phase 3 trial, molnupiravir further reduced hospitalization or death by 30% in mild to moderate COVID-19 patients compared with those in the placebo group.28
Molnupiravir was conditionally approved on March 23, 2022, in Korea for the treatment of adults (age ≥ 18 years) with mild-to-moderate COVID-19 within 5 days of symptom onset and at high risk of severe illness.29 Its use was only approved in circumstances in which both nirmatrelvir/ritonavir and remdesivir cannot be used.29 This is concordant with the recommendations and management guidelines for COVID-19 in Korea and the US.78
In Korea, a domestic animal study showed that combination therapy with nirmatrelvir (20 mg/kg) and molnupiravir (20 mg/kg) in lethally infected mice improved survival rates up to 80% compared with nirmatrelvir (36%, P < 0.001) or molnupiravir (43%, P < 0.001) administered alone.30 Additionally, another domestic study reported that molnupiravir could reduce the hospitalization risk for all adults, adults with underlying diseases, and elderly patients by 25%, 8%, and 4%, respectively, with 30% efficacy in a model-based cost-effectiveness analysis.31 However, accurate global data regarding the effectiveness of molnupiravir has yet to be analyzed or applied in the context of Korea.
Molnupiravir is not free of concerns owing to the possibility of DNA mutations or that it may enhance the development of new viral variants because of its mechanism of action.3233 Although the US FDA has since concluded that the drug has low genotoxicity and is approved for emergency use, domestic guidelines do not recommend molnupiravir treatment during pregnancy or for pediatric patients under 18 years and recommend avoiding conception or breastfeeding within 4 days after discontinuation of molnupiravir.34 Further, men of reproductive age and potential should be counseled to avoid conception for at least 3 months.835
Monoclonal antibodies
Several neutralizing antibodies that directly block the coronavirus spike protein have been developed and used to treat asymptomatic-to-mild non-hospitalized patients to prevent disease progression.8 Unfortunately, recent data indicate that the spike protein mutations of the omicron variant markedly reduce its susceptibility to most of the currently authorized monoclonal antibodies.836
In Korea, regdanvimab was approved for emergency use in February 2021 and was the only monoclonal antibody available in Korea.37 It was shown that regdanvimab effectively reduced hospitalization and severe disease progression in patients with mild-to-moderate COVID-19 wild-type, beta, or delta variant.38 However, several studies reported its low affinity in vitro to the surface antigen of the Delta variant.38394041 Additionally, the omicron variant and its subvariants have markedly reduced in vitro susceptibility to regdanvimab.36 Accordingly, the emergency use authorization and distribution of regdanvimab were paused in Korea on February 21, 2022.42
In Korea, where omicron B5 is the dominant variant of SARS-CoV-2, no monoclonal antibodies are currently recommended to treat patients with COVID-19, regardless of severity.
CONCLUSIONS
As of November 2022, the available approved antiviral agents for the treatment of mild-to-moderate SARS-CoV-2 infection in Korea include nirmatrelvir/ritonavir, molnupiravir, and remdesivir. No monoclonal antibody is currently recommended for use in patients with COVID-19.
Although nirmatrelvir/ritonavir is the most recommended antiviral agent for asymptomatic high-risk COVID-19 patients and those with mild symptoms in the early phases of SARS-CoV-2 infection in the domestic guidelines, remdesivir is the most used agent to consider for the treatment of mild-to-moderate disease in Korea.
Based on reports of the mutation sites of SARS-CoV-2, the current antivirals are expected to remain effective against the variants, including omicron, and will continue to be an important therapeutic option for treating patients and controlling further exacerbation of the pandemic.
 XML Download
XML Download