

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Uveitis, characterized by inflammation of the uveal tissues including the iris, choroid and retina, is a major vision-threatening ocular disorder.1 Pediatric uveitis is less common than adult uveitis and accounts for 2–14% of cases of uveitis.23 Although the incidence of uveitis is known to be lower in children than in adults, uveitis in children has a relatively severe disease course and is accompanied with higher ocular comorbidities that affect the quality of life.456 Difficulties in examination and diagnosis; limited therapeutic options in children; ocular complications attributed to chronic inflammation such as glaucoma and cataract; extended disease burden over a lifetime; and increased risk of amblyopia are possible challenging factors specific to pediatric uveitis. Although previous studies based on the patients who visit the referral centers have been reported,7 there is a lack of studies concerning the epidemiology and incidence of pediatric uveitis in Korea.
Although uveitis can occur as a purely isolated ocular inflammation without any specific cause, it may also arise as a co-manifestation of many other medical disorders, especially systemic immune-mediated inflammatory diseases. Systemic autoimmune diseases associated with uveitis include psoriatic arthritis, spondyloarthritis, inflammatory bowel disease, juvenile idiopathic arthritis (JIA), and Behçet’s disease.8 Uveitis in the pediatric population exhibits a different spectrum of systemic association compared to that observed of adult uveitis.4 Kawasaki disease and JIA, which are not common in adults, are casually associated with uveitis in children.4910 Systemically associated pediatric uveitis should be detected in the early stage of the disease to ensure proper treatment and better prognosis. However, since systemic inflammatory signs may not be prominent in the acute stage of uveitis, recognizing the association with systemic diseases may be challenging. Thus, it is important to understand the epidemiological characteristics of pediatric uveitis and the frequency of systemic autoimmune diseases that can cause uveitis in children.
In this study, we aimed to evaluate and report the nationwide incidence and prevalence of pediatric uveitis in South Korea based on period, age, anatomic type, and systemic associations using a nationwide, population-based data source.
METHODS
Data source
A single-payer, mandatory health insurance system is implemented in South Korea and is regulated by the National Health Insurance Service (NHIS). All healthcare providers should submit medical claims to the NHIS for review and reimbursement, along with information such as demographics, diagnostic codes based on the International Classification of Diseases (ICD)-10 codes, procedure codes, prescription records, and healthcare facilities. Thus, the NHIS claims system serves as a centralized database structure providing nationwide population-based data.
Study variables
In this study, we included all individuals younger than 19 years of age at the first episode of noninfectious uveitis. At least three claims of diagnostic codes of uveitis (Supplementary Table 1) on separate days from ophthalmologists with at least once claim of prescription codes of steroid and immunosuppressive agents (Supplementary Table 2) in 2002–2018 were considered for the operational definition of uveitis. Since we confined our target disease to noninfectious uveitis, patients with any diagnosis code of infectious uveitis (Supplementary Table 1) were excluded. In order to minimize misdiagnoses, uveitis claims combined with claims of conjunctivitis, keratitis, and blepharitis on the same day, and uveitis claims within 30 days of ocular trauma were regarded as invalid claims (Supplementary Table 3). Additionally, uveitis claims within 90 days following any intraocular procedure were excluded.
All uveitis cases were classified as anterior or non-anterior uveitis (i.e., intermediate, posterior or pan-uveitis) in accordance with the ICD-10 codes. If the diagnostic code indicated intermediate or posterior uveitis in patients initially diagnosed with anterior uveitis, the case was categorized as non-anterior uveitis.
Demographic characteristics, including age and sex, were collected separately. Patients with noninfectious uveitis were classified as having an associated systemic condition if they presented with any of the following diagnoses during the study period: JIA, spondyloarthropathy, Behçet’s disease, Kawasaki disease, sarcoidosis, systemic lupus erythematosus, and multiple sclerosis. Noninfectious uveitis without these conditions were classified as idiopathic uveitis.
Study outcomes and statistical analysis
Incidence rate
In order to exclude recurrent cases, we washed out the first 3 years (2002–2004) for newly detected cases; the study only included the incident uveitis cases after January 1, 2005. Time of the first incident case was defined as the date of the first diagnosis by an ophthalmologist for uveitis. A Poisson distribution was used to calculate the incidence per 100,000 person-years. Four-year and overall incidences were calculated using 95% confidence intervals (CIs). The incidence based on age and sex was also calculated using 95% CIs.
Prevalence
Prevalent cases were defined as those with clinic visits per calendar year. Our definition of prevalent cases considered uveitis as a purely episodic disease rather than a chronic disease. To include all patients with uveitis based on this definition, this study included patients diagnosed with pediatric uveitis from 2002 to 2018. The annual prevalence was estimated according to the total number of cases per year and the total population who qualified for NHIS on the 1st of January of each year.
The incidence rates and prevalence were analyzed from the 2010 Korean Population Census data provided by the Korean Statistical Information Service.11 Descriptive characteristics are presented as mean ± standard deviation, median (interquartile range), numbers, or frequencies in percentages (%). The χ2 test was used to determine the differences in the proportion of categorical variables, and analysis of variance was used to evaluate the differences between the means of continuous variables. Statistical analyses were performed using SAS software version 9.4 (SAS Inc., Cary, NC, USA) and R version 4.0.0 (R Foundation for Statistical Computing, Vienna, Austria; http://www.r-project.org). Statistical significance was set at P < 0.05.
Ethics statement
The study protocol was approved by the Institutional Review Board of Seoul National University Hospital (IRB No. E-2001-003-1090). The need for informed consent was waived by the board because the data originated from de-identified secondary data released by the NHIS for research purposes.
RESULTS
A total of 10,862,616 patients over 128,688,078 person-years were evaluated from 2005 to 2016. The number of eligible pediatric patients with uveitis was 5,972 (3,530 boys [59%] and 2,442 girls [41%]). Overall, we identified 5,368 cases of anterior uveitis and 604 cases of non-anterior uveitis during the study period; 51.4% (3,069 cases) of pediatric noninfectious uveitis cases revealed a recurrent or chronic disease course.
Incidence
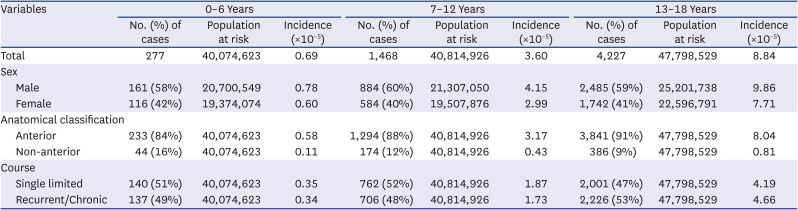
The overall incidence of pediatric noninfectious uveitis in South Korea was 4.64 (95% CI, 4.52–4.76) per 100,000 person-years. The annual incidence rates of pediatric uveitis ranged from 3.30 to 6.35 per 100,000 person-years during the study period. The incidence rate gradually increased from 3.32 in 2005 to 6.35 in 2009 and subsequently decreased to 3.99 and 3.30 in 2014 and 2016, respectively (Table 1 and Fig. 1). The incidence of pediatric uveitis increased with age; the lowest incidence was shown in children aged 0–6 years (0.69 per 100,000 person-years), whereas the highest incidence was shown in those aged 13–18 years (8.84 per 100,000 person-years) (Table 2). Overall, 89.9% (5,368 cases) of pediatric noninfectious uveitis patients had anterior uveitis with an incidence of 4.17 per 100,000. The incidence of recurrent or chronic uveitis cases was 2.38 per 100,000 person-years; among them, 85.5% (2,624 cases) involved anterior uveitis with an incidence of 2.04 per 100,000.
Table 1
Incidence rate of pediatric noninfectious uveitis by period in 2005–2016
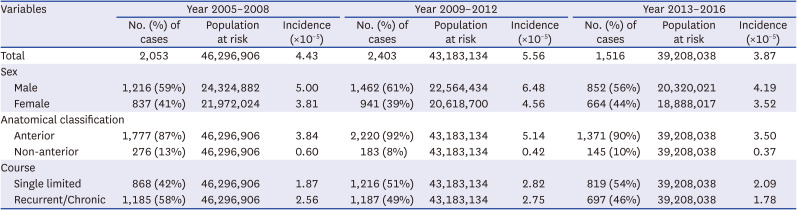
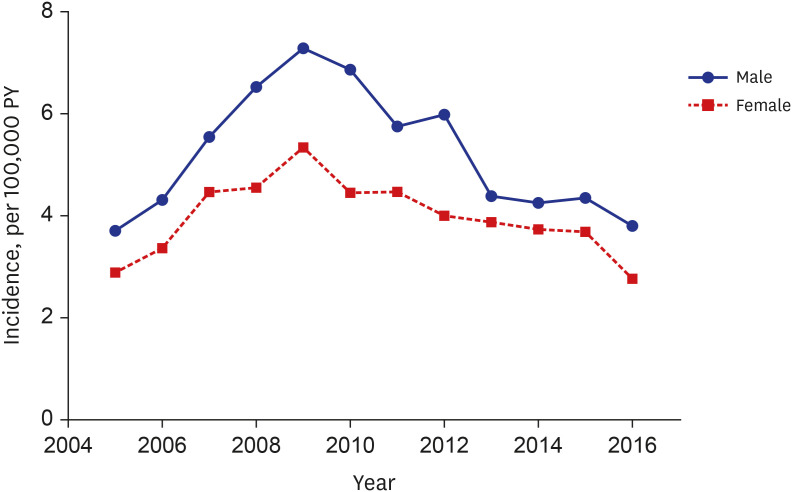
Table 2
Incidence rate of pediatric noninfectious uveitis by age group in 2005–2016
Prevalence
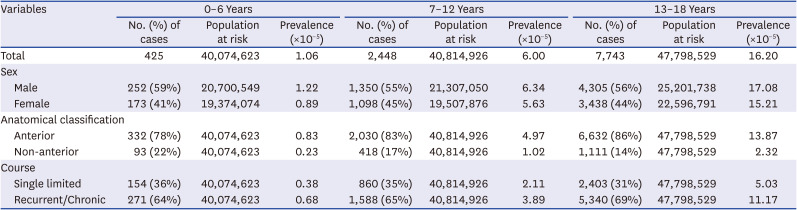
The prevalence of pediatric noninfectious uveitis per 100,000 persons in 2005–2016 was 8.25 (95% CI, 8.09–8.41). The prevalence for boys and girls was 8.79 per 100,000 and 7.66 per 100,000 persons for the given study period, respectively. The prevalence was consistently higher in male than in female participants in all age groups, with a male-to-female ratio of 1.12 to 1.37. Overall, 84.7% (8,994 cases) of pediatric noninfectious uveitis cases had anterior uveitis with a prevalence of 6.99 per 100,000. The prevalence tended to increase with age; the lowest prevalence was found among children aged 0–6 years (1.06 per 100,000), while the highest prevalence was found in those aged 13–18 years (16.20 per 100,000) (Table 3).
Table 3
Annual prevalence of pediatric noninfectious uveitis by age group
Systemic associations
Considering the prevalent cases, 8.7% (926 cases) of pediatric noninfectious uveitis cases were associated with JIA. The prevalence of JIA-associated uveitis was 0.72 per 100,000 (95% CI, 0.67–0.77). The prevalence for the male and female pediatric population was 0.78 per 100,000 and 0.66 per 100,000, respectively. However, 2,696 cases (25.4%) were associated with other systemic conditions, such as ankylosing spondylitis, Behçet’s disease, Kawasaki disease, etc. JIA was the most common systemic association of noninfectious uveitis in the younger age group (0–12 years), with 11.4% (327 cases) of noninfectious uveitis cases and a prevalence of 0.40 per 100,000. The most common systemic comorbidity of noninfectious uveitis was ankylosing spondylitis in the older age group (13–18 years), with 14.6% (1,127 cases) of cases and a prevalence of 2.36 per 100,000 (Table 4).
Table 4
Systemic associations of pediatric noninfectious uveitis

The proportion of systemic associations was higher in the recurrent or chronic cases; JIA-related uveitis was 11.2% (803 cases) of recurrent or chronic noninfectious uveitis cases with a prevalence of 0.62 per 100,000 (Table 5).
Table 5
Systemic associations of recurrent/chronic pediatric noninfectious uveitis

DISCUSSION
In the present nationwide population-based study, we provided the prevalence and incidence rates of pediatric uveitis and associated systemic autoimmune diseases in South Korea. Ideally, epidemiologic investigations of rare diseases, such as pediatric uveitis, should be population-based studies to achieve accuracy of epidemiological data without the possibility of referral bias for a selected population.12 To the best of our knowledge, this is the first population-based study investigating the largest population of pediatric uveitis patients in South Korea. During the period from 2005 to 2016, the overall incidence and prevalence of pediatric noninfectious uveitis were 4.64 per 100,000 person-years and 8.25 per 100,000 persons, respectively.
Our study demonstrated that the incidence and prevalence of pediatric uveitis were higher in the 13–18 years age group than in the 0–6 years age group. The increase in the detection rate by age was also observed not only in other epidemiologic studies concerning pediatric uveitis,131415 but also in the epidemiologic study of all-age uveitis conducted in Korea.12 This could be attributed to the challenges in reporting symptoms and performing comprehensive eye examinations in younger patients.
It is difficult to perform a direct comparison between the countries owing to the paucity of epidemiologic data concerning pediatric uveitis and the disparity in the medical system used by each country and survey period. However, a methodologically similar study based in Finland reported a similar overall incidence (4.3 per 100,000 person-years). Ninety percent of these patients presented with anterior uveitis, which was similar to our result: 89.9% of our patients presented with anterior uveitis.16
While the previous epidemiologic study conducted in Korea had investigated nationwide trends using the Sample Cohort published by the NHIS,12 our study is meaningful in that it captured all individuals, not simply a sample cohort. In addition, we analyzed the uveitis pattern with respect to age of children in more detail, and in particular, elucidated the relationship between pediatric uveitis and JIA.
Previous studies reported JIA to be the most common systemic association of pediatric uveitis171819; 47% of pediatric patients with uveitis were identified as having JIA-related uveitis in a study based in the United Kingdom.4 A claims database in the United States demonstrated a prevalence of pediatric noninfectious uveitis of 29 per 100,000 persons, of which 26.2% were associated with JIA.20 The overall JIA prevalence is reportedly higher in North America and Europe than in Asia21 and the percentage of patients with JIA-associated uveitis cases in different geographic areas varies significantly.17 Unlike previous reports based on Caucasian children, the incidence of uveitis in JIA is lower in Asians than in Caucasians.22 Previous studies in Japan and Tunisia estimated that JIA-associated pediatric uveitis was absent or had a prevalence rate of 6.25% of evaluated cases of pediatric uveitis, respectively.2324 A Canadian JIA cohort study also demonstrated that JIA patients of European origin had a higher risk of developing uveitis than those of non-European origin.25 These results suggested that ethnicity is a risk factor for JIA-associated uveitis. In the present study, 8.7% of pediatric noninfectious uveitis cases were associated with JIA, which is similar to the reported value among Asian populations, thereby supporting our assumption that the systemic cause of pediatric uveitis varies according to ethnicity. The large variation in the methods and design used in the studies and varying medical systems between countries render direct comparison challenging; thus, comparisons between epidemiologic studies could only be achieved in a limited way.
Our study had several limitations. The study identified pediatric uveitis cases based on the ICD-10 diagnosis system and thus could not individually confirm the diagnosis of uveitis by ophthalmic examination, resulting in certain events of missed diagnosis and/or misdiagnosis. Thus, misclassification could have occurred owing to the study methods that classify patients as having only anterior uveitis and non-anterior uveitis. In particular, pediatric patients with evidence of uveitis in both anterior and posterior locations were not classified as having panuveitis; the patients were categorized as having non-anterior uveitis according to our study methods. Furthermore, since the current study is based on insurance claims data, it is difficult to obtain detailed clinical characteristics of pediatric uveitis, such as severity, treatment response, recurrence, or laterality.
In conclusion, the nationwide incidence and prevalence of pediatric noninfectious uveitis in 2005–2016 were 4.64 per 100,000 person-years and 8.25 per 100,000 persons, respectively. Both the incidence and prevalence tended to increase with age and most of these cases involved anterior uveitis. The proportion of JIA cases among pediatric noninfectious uveitis cases was 8.7%. These population-based study findings provide a better understanding of the public health burden and aid in planning health-care strategies for pediatric patients with uveitis.
 XML Download
XML Download