

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
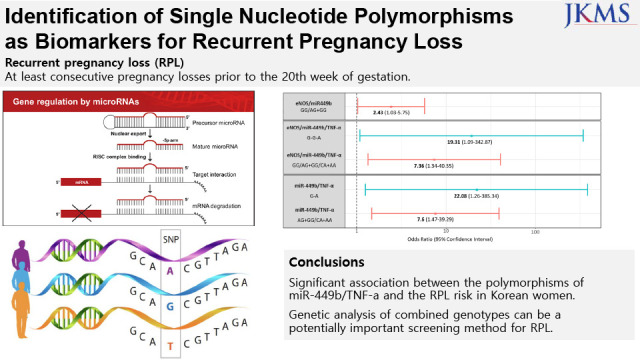
Human reproduction is a very complicated process involving genetic, anatomic, and environmental factors that lead to different outcomes due to various reasons. Even before implantation, as many as 30% of human conceptions are missed. Another 30% show a positive result for serum human chorionic gonadotropin test but fail to progress.1 The risk of miscarriage increases with a previous pregnancy loss. The probability of miscarriage after three consecutive spontaneous abortions is 30%, and the probability increases to 40–50% after four consecutive abortions.2 The risk of miscarriage also increases with maternal age and after the maternal age of 40, it increases more rapidly than before.3 Previously, recurrent pregnancy loss (RPL) was defined as three or more consecutive pregnancy loss. In present, according to the American Society for Reproductive Medicine, RPL is defined as at least two consecutive pregnancy loses prior to the 20th week of gestation, according to.4 Based on the definition, about 1–5% of all women are affected by RPL,5 and this rate is expected to grow as the average age of first-time mothers increases.
Chromosomal aneuploidy is the major cause of isolated, spontaneous pregnancy loss.6 Other causes of RPL identified so far include other genetic factors, anatomical abnormalities (maternal or fetal malformations), immunologic and endocrine disorders (antiphospholipid syndrome and hypothyroidism, among others), infections, and environmental factors. Several biomolecules such as mixed lymphocyte reaction blocking factor, anti-mullerian hormone, immunologic factors, and miRNAs78910 have been evaluated as potential biomarkers of RPL. A large number of RPLs occur due to a combination of these factors. Among the biomolecules with potential as diagnostic, therapeutic, and prognostic biomarkers of RPL, approximately 50% RPLs are believed to occur due to genetic factors as isolated pregnancy loss.1511 However, so far, there is neither a definite diagnostic test based on relevant gene panel nor a treatment for alleviating effects of these genetic factors.
MicroRNAs (miRNA) are a class of short RNA molecules regulating the gene expression.12 Recently, it has been reported that repeated abortion is related to polymorphisms of miRNAs or single nucleotide polymorphisms (SNPs).1314151617 Even though SNPs are not directly related to the RPL pathophysiology in all patients, there is significant association between the two in a significant number of patients in South Korea.13141617 One study done by Rah et al.13 in 2017 showed the association between two encoding miRNA (miR-27a, miR-449b) and RPL in Korean population. The certain type of polymorphism (miR-27aA>G and miR-449bA>G) showed association to increased RPL risk. Rah et al.14 also showed that the kinase insert domain-containing receptor (KDR) gene (KDR-604T→C polymorphism) was associated with RPL. The polymorphisms in endothelial nitric oxide synthase (eNOS) gene polymorphisms (−786T>C, 4a4b, 894G>T) and tumor necrosis factor-alpha (TNF-α) gene (−863C>A, −857C>T and +488G>A) were also associated with RPL in Korean patients.1516
Genetic analysis based on race is the key to accurate diagnosis because of genetic differences among races.18 Therefore, the purpose of this study was to compare and analyze the various genetic polymorphisms of RPL patients and controls in Korean women to verify the usefulness of any combinations of these polymorphisms as predictive markers of RPL.
METHODS
Subjects
For this prospective study, 103 subjects were enrolled in a tertiary referral hospital and a fertility center in South Korea. Of these, 53 women were enrolled in the RPL group based on the diagnosis criteria and the other 50 women were enrolled in the control group. Only women between 20 and 40 years of age with regular menstrual periods at 21–35-day intervals were chosen for this study. RPL was diagnosed if there were two or more biochemical pregnancies or pregnancy losses before 20th week of gestation. For the control group, we enrolled parous women without any history of spontaneous abortion. They were enrolled at their visit to the outpatient clinic of the gynecology department of the tertiary referral hospital or the fertility clinic. Women who had experienced pregnancy loss within 3 months before their visit to the hospital or clinic were excluded. All subjects were given the option of withdrawing from the study at any time.
Laboratory evaluation
Venipuncture was done to collect 3 mL whole blood from subjects of the RPL group and the control group between menstrual cycle day (MCD) #2 and MCD#5. Serum was analyzed for clinical characterization of the groups and DNA was extracted from the blood samples. For serum analysis, hematologic factors including complete blood count (hemoglobin, platelet, white blood cell [WBC] count), and WBC differential count were assessed. Natural killer cell count was analyzed by flow cytometry. Coagulation variables such as activated partial thromboplastin time (aPTT), prothrombin time (PT), antithrombin III, protein C (functional), and lupus coagulant (LA) were measured by performing clotting assay and chromogenic assay. In addition, antibodies clinically assumed to be related to RPL, such as anti-β2GP1 IgG, anti-β2GP1 IgM, anti-cardiolipin antibody (ACA) IgG, ACA IgA, ACA IgA Quantitation,19 TSH Receptor antibody, thyroglobulin antibody, and thyroid peroxidase antibody were analyzed by either enzyme-linked immunosorbent assay, thin layer immunoassay, or electrochemiluminescence immunoassay. Homocysteine and folate levels were also analyzed by chemiluminescent immunoassay.
Genetic analysis
Genomic DNA was extracted from non-coagulated peripheral blood using the QIAamp DNA Mini Kit (Qiagen, Redwood, CA, USA). Among the target genes, those encoding miRNAs (miR-27a, miR-449b), LEPR, KDR, and eNOS were analyzed by SNP genotyping.13141617 For mutational analysis, we performed the Taqman probe assay on the Applied Biosystems E7500 Fast real-time PCR system (Thermo Fisher Scientific, Waltham, MA, USA). For TNF-α, we used MnlI for polymerase chain reaction (PCR)-restriction fragment length polymorphism (RFLP) to analyze gene fragments. Primer sequences for PCR amplification of TNF-α were: forward-5′-AGGAATGGGTTACAGGAGACCACT-3′, and reverse-5′-TCTACATGGCCCTGTCTTCGTTGAG-3′. Distilled water was used as a negative control for PCR amplification.
Statistical analysis
The clinical variables of the patient and control groups were calculated as mean ± standard deviation, and compared using Student’s t-test. MedCalc Software (MedCalc software, Mariakerke, Belgium) was used for all statistical analysis. P < 0.05 was considered statistically significant. The genotype distribution and allele frequency were analyzed using a Fisher’s exact test or χ2 test. For haplotype analysis, SNPAlyze Ver. 9.0 Standard (DYNACOM Co., Ltd., Yokohama, Japan) software was used. To analyze the association between each SNP marker and RPL risk, odds ratio (OR), relative ratio (RR), and 95% confidence intervals (CIs) were calculated.
Ethics statement
Blood samples were taken after the consent to participate in the study was obtained. This study was approved by the Institutional Review Board (IRB) of the Yonsei University Health System, Severance Hospital (IRB No. 4-2018-0997). This study was performed in accordance with the principles of the Declaration of Helsinki. Written informed consent was obtained from all participants.
RESULTS
Patient characteristics
A total of 53 women diagnosed with RPL agreed to participate in the study. For the control group, 50 women who were parous without a history of spontaneous abortion were recruited. The demographic characteristics are listed in Table 1. The mean age of the control group was 39.80 ± 4.54 years and that of the RPL group was 36.42 ± 3.23 years, and the difference was statistically significant (P < 0.05). Other factors of demographic characteristics such as body mass index were not statistically different between the two groups.
Table 1
Demographic characteristics and clinical variables of RPL patients and control subjects
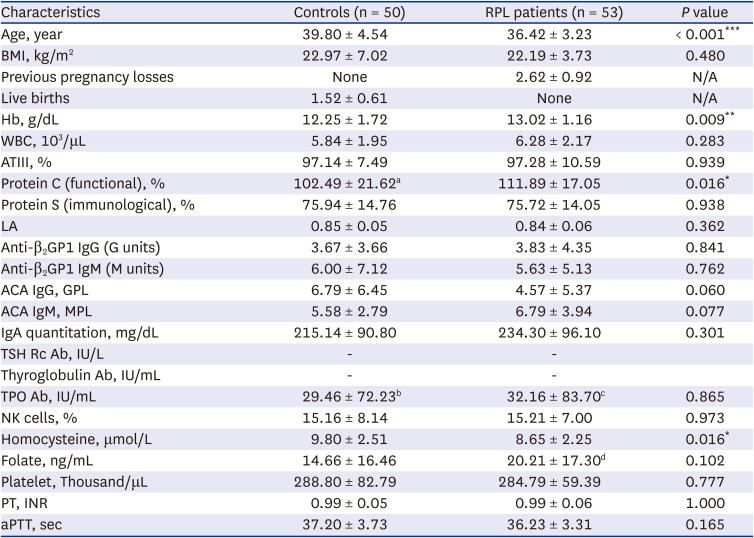
Values are presented as mean ± standard deviation.
RPL = recurrent pregnancy loss, BMI = body mass index, Hb = hemoglobin, WBC = white blood cell, ATIII = antithrombin III, LA = lupus anticoagulant, GPL = IgG phospholipid units, MPL = IgM phospholipid units, ACA = anti-cardiolipin antibody, TSH = thyroid-stimulating hormone, TPO = thyroid peroxidase, NK = natural killer, PT = prothrombin time, INR = international normalized ratio, aPTT = activated partial thromboplastin time, N/A = not available.
aValue for 49 control subjects; bValue for 48 control subjects; cValue for 50 RPL patients; dValue for 51 RPL patients.
*P < 0.05; **P < 0.01; ***P < 0.001.
With respect to clinical variables, only the mean hemoglobin level (g/dL) of the RPL group was significantly greater than that of the control group (13.02 ± 1.16, 12.25 ± 1.72, respectively, P < 0.05). Among the variables related to coagulation, only protein C level (%) differed between the RPL and control groups (111.89 ± 17.05, 102.49 ± 21.62, respectively, P < 0.05), but they were all within normal range. Other factors such as antithrombin, PT, and aPTT did not show any statistically significant difference between the two groups. The primary antiphospholipid antibodies including LA, ACA IgG/IgM, and anti-β2GP1 IgG/IgM were also analyzed. Among the antibodies, levels of only anti-β2GP1 IgG and ACA IgM were elevated in the RPL group, but the values were within normal range and the differences were not statistically significant. Both within the normal range (5.0 μmol/L–15.0 μmol/L), homocysteine (μmol/L), which has been reported to impair implantation as well as to cause fetoplacental insufficiency in pregnant women,2021 was elevated in the control group than in the RPL group (9.80 ± 2.51, 8.65 ± 2.25, P < 0.05).
Genotypic analysis
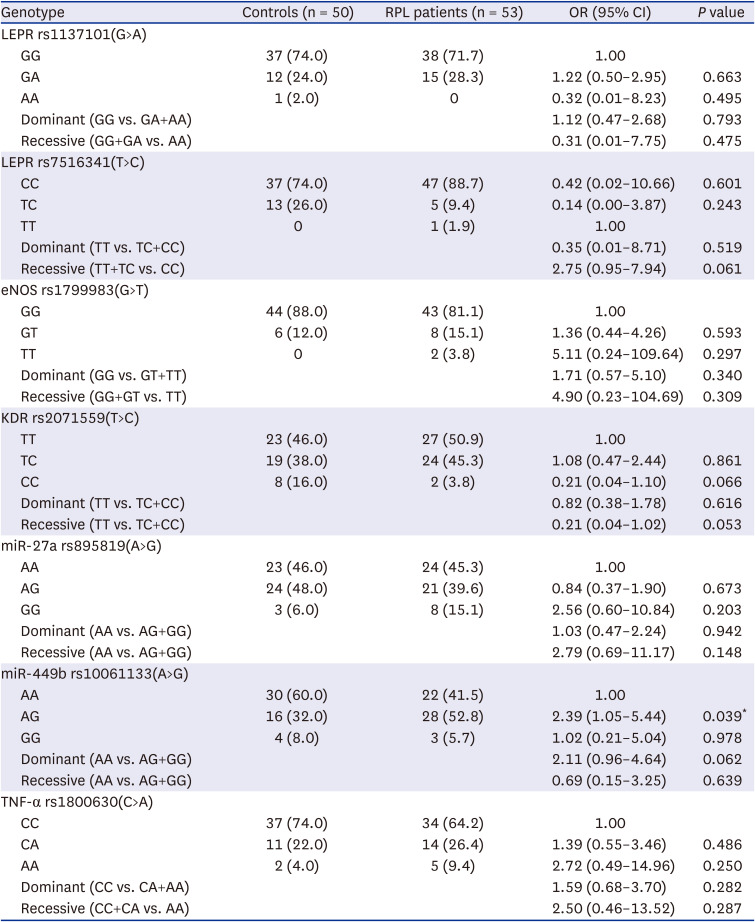
The genotype and allele frequencies of the SNPs of the RPL and control groups are listed in Table 2. We analyzed the polymorphisms in LEPR, eNOS, KDR, miR-27a, miR-449b, and TNF-α to figure out any specific genotype associated with RPL. For LEPR, eNOS, KDR and TNF-α, the different genotypes showed comparable distribution between the control and RPL groups, and statistically significant OR was not calculated. For miR-27a (A>G), the most common genotype in the control group was AG type, while that in the RPL group was AA. However, the OR of AG type, using AA type as the reference, was 0.84 with 95% CIs 0.37–1.90 (P = 0.673). The AG genotype of miR-449b (A>G) polymorphism showed a significant association with the risk of RPL when compared to the AA genotype (AA vs. AG: OR, 2.39, 95% CI, 1.05–5.44; RR, 1.61, 95% CI, 1.01–2.57). However, other genotypes including dominant and recessive genotype models did not show a significant risk of RPL.
Table 2
Genotype analysis of LEPR, eNOS, KDR, miR-27a, miR-449b and TNF-α polymorphisms in RPL patients and controls
The combination analysis of SNPs corresponding to each gene is shown in Table 3 and the combinations with significantly elevated odds are presented in Fig. 1. For combination analysis, the dominant models of eNOS/miR-449b/TNF-α (GG vs. GT+TT, AA vs. AG+GG, CC vs. CA+AA, respectively) were assessed. Among the various genotype combinations, the combined genotype GG/AG+GG/CA+AA for eNOS/miR-449b/TNF-α was associated with a 7.36-fold higher risk of RPL compared to the reference genotype (OR, 7.36, 95% CI, 1.34–40.55; RR, 4.50, 95% CI, 1.11–18.27). When the combination of only eNOS/miR-449b was analyzed, the GG/AG+GG combination still showed a 2.43-fold higher risk of RPL (OR, 2.43, 95% CI, 1.03–5.75; RR, 1.57, 95% CI, 1.00–2.44). The combination genotypes AG+GG/CA+AA of miR-449b/TNF-α also showed a significant association with increased risk of RPL (OR, 7.60, 95% CI, 1.47–39.29; RR, 4.67, 95% CI,1.17–18.63). However, the GG/CA+AA combination and all the other combinations of eNOS/TNF-α did not show a statistically significant association to RPL.
Table 3
Combination analyses of eNOS 894G>T, miR-499b A>G, and TNF-α-863C>A polymorphisms in Korean RPL patients and controls
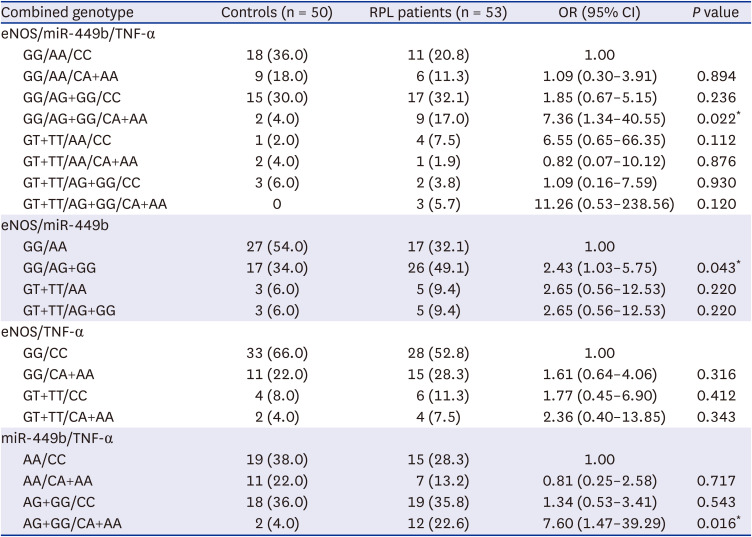
Fig. 1
Odds ratio of genotype combinations with significantly increased odds compared to reference. Odds ratio with 95% confidence interval in log scale.
eNOS = endothelial nitric oxide synthase, TNF = tumor necrosis factor.
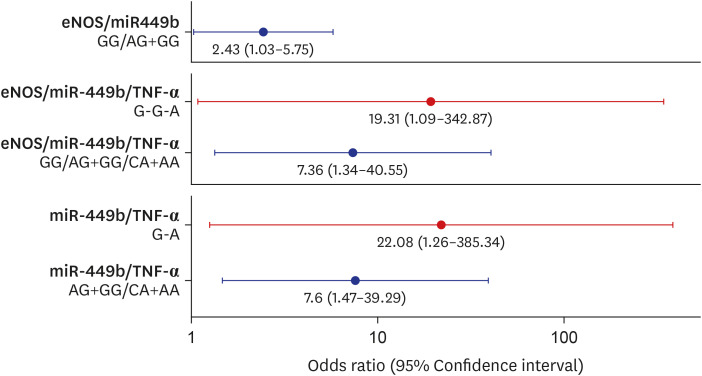
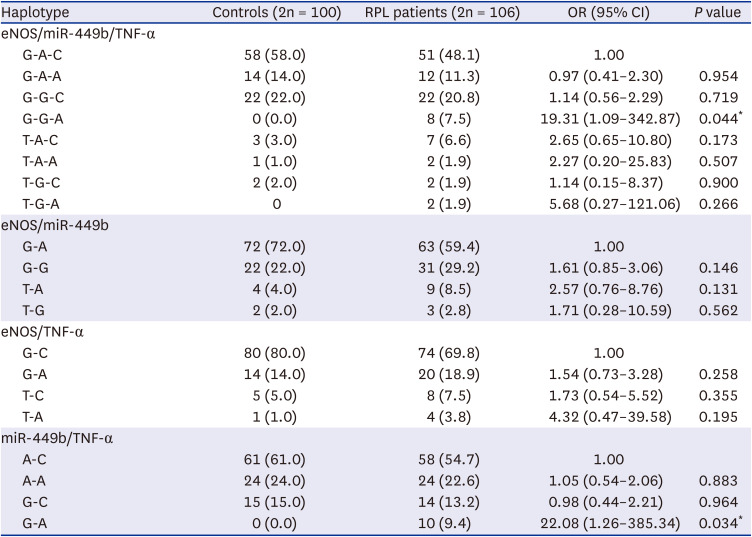
Haplotype-based analysis of the three miRNA polymorphisms (eNOS G>T, miR-499b A>G, and TNF-α C>A) and gene–gene interactions are listed in Table 4 and the haplotype combinations with significantly elevated odds are presented in Fig. 1. Among the models of the three polymorphic loci, the G-G-A haplotype (OR, 19.31, 95% CI, 1.09–342.87; RR, 16.72, 95% CI, 0.99–283.13; P = 0.051) was associated with an increased risk of RPL. Among the models of the two polymorphic loci, only the G-A haplotype of miR-449b/TNF-α was associated with increased RPL risk (OR, 22.08, 95% CI, 1.26–385.34; RR, 18.87, 95% CI, 1.13–315.40; P = 0.041), while none of the haplotypes of eNOS/miR-449b and eNOS/TNF-α showed statistically significant association with RPL risk.
Table 4
Haplotype analysis for the eNOS 894G>T, miR-499b A>G, and TNF-α-863C>A polymorphisms in RPL patients and controls
DISCUSSION
RPL has been one of the most important concerns related to pregnancy, and several studies have explored its etiology and pathogenesis. However, a definitive treatment as well as diagnostic or prognostic markers remain elusive.22 Among various markers with potentials, the polymorphism of miRNAs has garnered attention of researchers and certain miRNA polymorphisms have been shown to interfere with the production of mature miRNAs and, consequently, their target genes.23242526 In this study, we analyzed the association of polymorphisms in specific genes associated with RPL based on previous studies.13141617
In our study, the AG genotype of miR-449b showed an increased risk of RPL. Combination analysis showed that the combined genotypes of eNOS/miR-449b/TNF-α (GG/AG+GG/CA+AA), eNOS/miR-449b (GG/AG+GG), and miR-449b/TNF-α (AG+GG/CA+AA) were associated with an increased risk of RPL, all of which included the dominant genotype of miR-449b (AG+GG). In the haplotype-based analysis of the three miRNA polymorphisms (eNOS G>T, miR-499b A>G, and TNF-α C>A), the G-G-A haplotype among the three polymorphic loci and the G-A haplotype of miR-449b/TNF-α polymorphic loci showed statistically significant association with RPL risk.
While the OR of miR-449b (AG) was only 2.39 (P < 0.05), the OR from the combination analysis was higher. Among the three statistically significant combinations, miR-449b/TNF-α (AG+GG/CA+AA) presented the highest OR of 7.60 (P < 0.05) followed by eNOS/miR-449b/TNF-α (GG/AG+GG/CA+AA) with an OR of 7.36 (P < 0.05). In haplotype analysis, each combination showed a greater OR in which the OR for miR-449b/TNF-α (G-A) was the highest with 22.08 (P < 0.05) followed by that of eNOS/miR-449b/TNF-α (G-G-A) at 19.31 (P < 0.05) compared to the reference of each combination. Based on the OR of certain combinations, we propose that gene panels targeting miR-449b/TNF-α, or eNOS/miR-449b/TNF-α would have higher diagnostic value than any one specific SNP.
Furthermore, our results showed that the miR-449b polymorphism was related to increased risk of RPL. Also, genetic combinations composed of certain polymorphisms of miR-449b and TNF-α showed increased risks despite the fact that all polymorphisms of TNF-α were not individually associated with RPL. Based on a previous study on bovine blastocyst, miR-449b was proposed to be an important factor in the process of embryo implantation, cleavage timing, blastocyst development, and blastomere apoptosis.27 Furthermore, many evidence suggests that miRNAs are one of the potential regulators of hemostatic system; especially miR-449b potentially targets Factor VIII.28 Along with clinical variables such as protein C, miR-449b may be a causative factor for pregnancy loss by inducing implantation failure as well as hypercoagulation of placenta. TNF-α, an inflammatory cytokine, is one of the key factors involved in apoptosis, and autoimmune, endocrine, and neoplastic diseases. Also, an elevated level of TNF-α is related to miscarriage in both humans and animals. Since TNF-α is suspected to cause apoptosis of cytotrophoblasts, a mutation in the TNF-α encoding gene may induce abnormal development of placenta.29
One of the strengths of this study is that the study population consisted of one specific ethnicity (Korean), which minimized other possible confounding genetic variables. We analyzed not only each specific gene related to RPL but also all combinations of SNPs to propose the gene combination with strongest association. However, the limitation of this study is the small sample size, which did not allow the adjustment for confounding variables. Secondly, the analysis for chromosomal abnormality was not included as exclusion criteria in this study and not many cases have performed the chromosomal analysis for every abortion case. Also, the level of protein C and protein S of RPL group was different from that of typical RPL patients. The influence of thrombophilia in various ethnicity can be different, but it is more likely the result of sampling bias. In addition, this study only shows the association between SNPs in miRNAs and RPL development without either functional association or causal relationship. Further studies with better design are required to analyze other factors in the pathogenesis of RPL such as implantation, placental angiogenesis or immunologic profile of the mother.
In conclusion, this study established a significant association between the polymorphisms of miR-449b/TNF-α and the RPL risk. Also, it showed that the genetic analysis of combined genotypes can be a potentially important screening method for RPL in Korean women. A cohort study with a greater number of participants is necessary to further understand the relationship between specific genes and RPL, and the mechanism of the relationship so as to utilize these genes for diagnosis.
 XML Download
XML Download