

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Atrial fibrillation (AF) is associated with an increased risk of thromboembolic events. Non-vitamin K antagonist oral anticoagulants (NOACs) are effective in preventing thromboembolisms and generally recommended as first-line therapy in preference to warfarin.12 Furthermore, NOACs reduced the risk of major bleeding compared with warfarin in pivotal clinical trials.3456 All NOACs are administered in fixed doses without need for coagulation monitoring and have individual dose reduction criteria. Dose reduction criteria were met by 5–25% of patients enrolled in a pivotal trial. In the Effective Anticoagulation with Factor Xa Next Generation in Atrial Fibrillation-Thrombolysis in Myocardial Infarction 48 (ENGAGE AF-TIMI 48) trial, edoxaban was non-inferior to warfarin for stroke prevention and was superior to warfarin in safety outcome. In higher-dose regimens, the outcomes of a once-daily dose of edoxaban 30 mg in patients who met one of the criteria for dose reduction was investigated. Pharmacokinetic analysis in the ENGAGE AF-TIMI 48 trial showed consistent efficacy and safety of a reduced dose.7 However, a meta-analysis investigating the outcomes of on-label reduced-dose NOACs showed that patients eligible for reduced dose were at a higher risk of both thromboembolism and bleeding complications and were characterized by low body weight, advanced age, and renal impairment.8 These factors increased the risk of major bleeding and other adverse events.
Nevertheless, there are few reports on the outcomes of on-label reduced-dose NOACs. In this study, we aimed to assess safety and efficacy of on-label reduced-dose edoxaban in East Asian patients with AF in real world practice.
METHODS
Study population
The Safety and Effectiveness of Low Dose Edoxaban in Patients with Non-valvular AF (LEDIOS) registry is a multi-center, prospective, non-interventional cohort study to evaluate the safety and efficacy of low-dose edoxaban in patients with AF, who meet any of the dose reduction criteria. We conducted this trial at 51 centers in Korea. Patients who were indicated to receive NOAC for stroke prevention and were prescribed 30 mg of edoxaban and who met the dose reduction criteria were included. The dose reduction criteria for edoxaban are as follows; 1) creatinine clearance (CrCl) 15–50 mL/min, 2) body weight ≤ 60 kg, or 3) concomitant medications with potent P-glycoprotein interactions.
Data collection and study outcomes
The basic demographic data and medical history of each individual were collected, including age; sex; body weight; type of AF; renal function; and history of congestive heart failure, hypertension, diabetes mellitus, vascular disease, or thromboembolism. The primary safety outcome was major bleeding during treatment, as defined by the International Society on Thrombosis and Haemostasis (ISTH) criteria.9 The efficacy outcome was ischemic stroke including transient ischemic attack (TIA) or systemic embolism. The net clinical outcome was defined as the composite of stroke, systemic embolism, major bleeding, or all-cause mortality. Data were collected at baseline and during a follow-up period of at least 12 months. Patients were censored at outcome occurrence, at discontinuation of edoxaban treatment during the observation period, or at the end of the study period. Patients were divided into two groups of those who met one of the dose reduction criteria and those who met two or more dose reduction criteria. The outcomes were compared based on body weight, renal function, and stroke (CHA2DS2-VASc) or bleeding (HAS-BLED) risk scores. Furthermore, the association between the combination of stroke and bleeding risk scores (CHA2DS2-VASc + HAS-BLED) and the incidence of all outcomes was observed.
Statistical analysis
The baseline characteristics are presented as the mean ± standard deviation for continuous variables and as frequency with percentage for categorical variables. Continuous variables were compared using the unpaired t-test, and categorical variables were compared using either the χ2 test or Fisher’s exact test as appropriate. Event rate curves were obtained using a Kaplan-Meier analysis and compared using the log-rank test. The outcomes were assessed using a Cox proportional hazards model adjusted for age and are presented as the hazard ratio (HR). P values < 0.05 were considered statistically significant. Age adjustment was not performed in variables for CHA2DS2-VASc score and HAS-BLED score due to each score already including an age factor. All statistical analysis was performed using R version 3.6.0 (R Foundation for Statistical Computing, Vienna, Austria).
Ethics statement
This study was approved by the local Institutional Review Board (IRB) of Samsung Medical Center in Korea (IRB number: SMC IRB 2017-12-051). All patients provided informed consent and were registered at ClinicalTrials.gov (NCT03554837).
RESULTS
Clinical characteristics
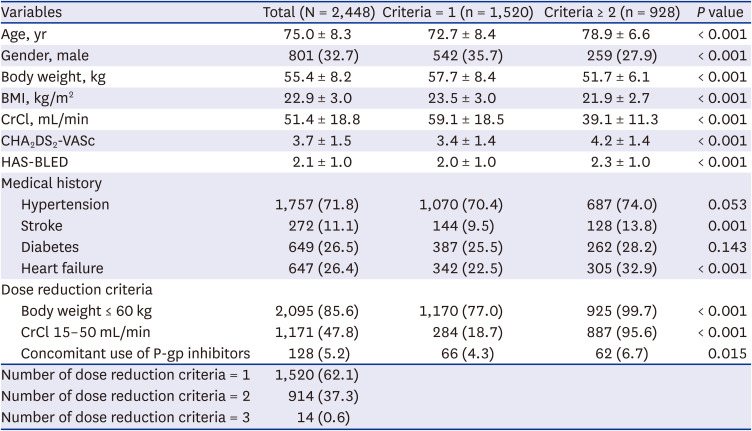
A total of 2,585 patients was screened for study. Among these, 78 patients did not meet the dose reduction criteria, six did not receive 30 mg of edoxaban, and 87 did not complete follow-up visit and did not have available clinical outcome data. 2,448 patients who have received 30 mg of edoxaban for stroke prevention was included in the present study (Fig. 1). The mean age was 75.0 ± 8.3 years, and 801 (32.7%) patients were men. The mean CHA2DS2-VASc score was 3.7 ± 1.5. The mean body weight was 55.4 ± 8.2 kg, and mean CrCl was 51.4 ± 18.8 mL/min. Among the patients, 2,095 (85.6%) experienced dose reduction for body weight 60 kg or lower, 1,171 (47.8%) for CrCl 15–50 mL/min, 128 (5.2%) for concomitant medication with P-glycoprotein inhibitor, and 928 (37.9%) had more than one clinical feature indicating dose reduction. Patients who had more than one dose reduction criteria were older, more likely female, had lower body weight and lower CrCl, and had higher CHA2DS2-VASc score and HAS-BLED score. The baseline characteristics of the patients are summarized in Table 1.
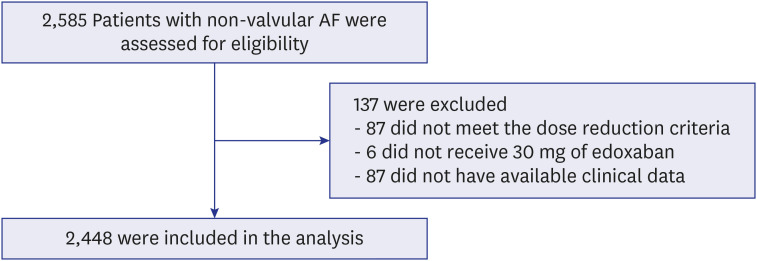
Table 1
Baseline characteristics
Outcomes
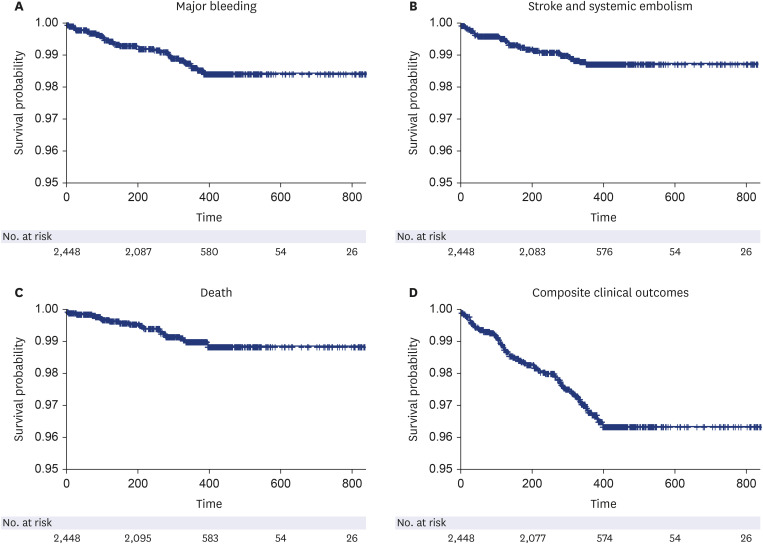
The mean follow-up duration was 344.2 ± 131.9 days. Major bleeding events occurred in 31 patients, and the event rate was 1.34% per year. The event rate of strokes and systemic embolisms was 1.13%/yr. The overall net clinical outcome of composite of stroke, systemic embolism, major bleeding, or all-cause mortality occurred in 73 patients, an event rate of 3.19%/yr (Fig. 2).
Fig. 2
Kaplan-Meier curves of the primary outcome. (A) Freedom from major bleeding. (B) Freedom from ischemic strokes or systemic embolisms. (C) Freedom from all cause death. (D) Freedom from composite clinical outcomes.
According to the dose reduction criteria, patients who had two or more dose reduction criteria showed similar outcomes for major bleeding events (HR, 1.04; 95% confidential interval [CI], 0.50–2.13), stroke and systemic embolism (HR, 1.63; 95% CI, 0.76–3.52), and net clinical outcomes (HR, 1.08; 95% CI, 0.67–1.72) compared with those showing one dose reduction criteria. In patients who met the dose reduction criteria of body weight ≤ 60 kg, the event rate of major bleeding was 1.47%/yr, stroke was 0.96%/yr, and composite clinical outcome was 3.11%/yr. In patients who had CrCl 15-50 mL/min, the event rates of major bleeding, stroke, and composite outcome were 1.28%/yr, 1.84%/yr, and 3.78%/yr, respectively (Table 2).
Table 2
Event rates according to dose reduction criteria

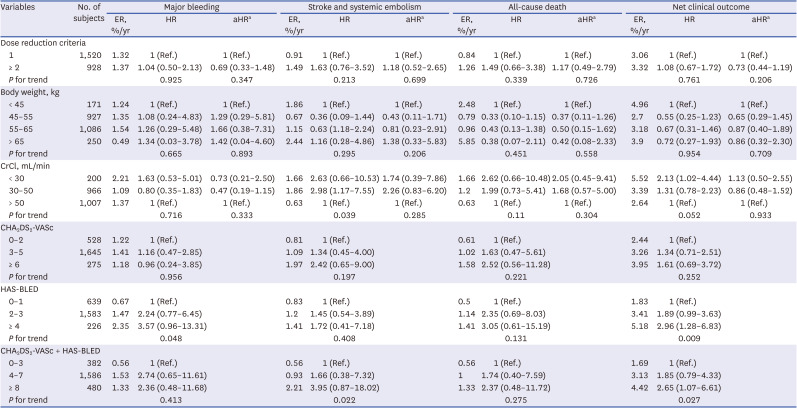
Patients with severe renal dysfunction (CrCl < 30 mL/min) showed no significant difference compared with patients with normal renal function (CrCl > 50 mL/min) after age adjustment in composite clinical outcomes (unadjusted HR, 2.13; 95% CI, 1.02–4.44 and adjusted HR, 1.13; 95% CI, 0.50–2.55, respectively). There were no significant differences in the risks of stroke and systemic embolism, major bleeding, and all-cause mortality according to renal function. The results for all outcomes showed no statistically significant differences according to subgroups of body weight and CHA2DS2-VASc score. A higher HAS-BLED score was associated with an increased risk of composite clinical outcome compared to that in the lower score group (0–1 [reference], 2–3 [HR, 1.89; 95% CI, 0.99–3.63], and ≥ 4 [HR, 2.96; 95% CI, 1.28–6.83]), and a higher combination of CHA2DS2-VASc and HAS-BLED score showed increased risk of composite clinical outcome (CHA2DS2-VASc + HAS-BLED 0–3 [reference], 4–7 [HR, 1.85; 95% CI, 0.79–4.33], and ≥ 8 [HR, 2.65; 95% CI, 1.07–6.61]) (Table 3).
Table 3
HRs of outcomes by variables
DISCUSSION
This study was the largest, prospective real-world study to investigate the safety and efficacy of on-label low-dose edoxaban in Asian patients. The main findings are as follows. First, on-label reduced dose of edoxaban is safe and effective in real-world practice. The clinical event rates for major bleeding, stroke, and net clinical outcome were low. Second, the results were consistent according to the dose reduction criteria or other baseline characteristics, including severe renal dysfunction or extremely low body weight. Third, higher bleeding score or combination of stroke and bleeding score showed unfavorable composite clinical outcomes.
The ENGAGE AF-TIMI 48 trial was a three-group, randomized trial comparing two dose regimens of edoxaban with warfarin, and a higher dose regimen was approved according to the result.4 In a pivotal randomized controlled trial, 1,784 (25.4%) patients were eligible for reduced-dose edoxaban, and the annualized event rate was 1.79% for stroke or systemic embolic event (SEE) and 3.05% major bleeding. Higher rates of thromboembolic events and major bleeding outcomes were observed compared to those in the no dose reduction group.7 Both groups showed better outcomes compared with the warfarin group. These results were consistent in meta-analysis of three pivotal randomized controlled trials (RCTs) comparing reduced dose of NOAC with warfarin in patients with AF.8 The annualized rate of major bleeding was 3.60% and the annualized rate of stroke or systemic embolism was 2.39% for patients eligible for reduced-dose NOACs, who had higher risk of thromboembolic and bleeding complications than those who did not experience dose reduction. In our study cohort, the overall major bleeding event rate was 1.34%, and that of stroke and SEE was 1.13%. In general, real-world studies have fewer events than randomized trials; even considering this, our study results demonstrated the safety and efficacy of on-label reduced-dose edoxaban in the real world.
In the ENGAGE AF-TIMI 48 trial, 684 patients received 30 mg of edoxaban due to body weight ≤ 60 kg, and 1,306 received reduced dose due to CrCl 30–50 mL/min in the higher-dose edoxaban group.7 Outcomes stratified by dose reduction criteria in that pivotal trial were as follows. The event rate for major bleeding was 3.16%/yr and that for stroke was 2.05%/yr in patients with body weight ≤ 60 kg, and the event rate for major bleeding was 3.26%/yr and that for stroke was 1.74%/yr in patients with renal dysfunction. In our study cohort, we included a larger number of patients, and events rates were 1.47%/yr and 0.96%/yr for major bleeding and stroke, respectively, in low-body weight group, which showed favorable outcomes. In the renal dysfunction group, event rates were 1.28%/yr and 1.84%/yr for major bleeding and stroke, respectively. These results demonstrate the safety of reduced-dose edoxaban and showed comparable efficacy.
According to race, there were 2,909 patients of Asian and 18,195 of non-Asian in the pivotal trial, and Asian race was associated with favorable safety and comparable efficacy to warfarin.10 A similar trend was also demonstrated in subgroup analysis of East Asians.11 This may be due to the lower trough concentration and anti-FXa activity of the Asian race, and the increased risks of major bleeding on warfarin, especially intracranial hemorrhage, in the Asian population.12 Only 294 East Asian individuals were included in the pivotal trial, and event rate for major bleeding was 1.91%/yr and that of stroke was 1.41%/yr.11 Although our study is non-interventional, our results show comparable outcomes in both safety and efficacy, which suggests that reduced-dose edoxaban can be used safely and effectively in the Asian population. Further, the mean body weight and CrCl in pivotal trial was 65 kg and 46 mL/min. In our cohort, the mean body weight and CrCl was 55 kg and 51 mL/min. Our result demonstrated the efficacy and safety in low body weight population. We demonstrated this through large-scale, well-controlled real-world evidence.
Both efficacy and safety are important in oral anticoagulant therapy. The concern of fatal bleeding has resulted in overuse of off-label low-dose NOAC, especially in frail patients. However, off-label underdose of NOACs is associated with a higher risk of stroke in real-world evidence.1314 Recently, there has been a report that compared the effects of lower dose edoxaban regimen (LDER) and higher dose edoxaban regimen (HDER) on the composite net clinical outcomes of stroke, systemic embolism, major bleeding, or all-cause mortality.15 The primary net clinical outcome was reduced with LDER compared with HDER. The higher stroke events in the LDER group were counterbalanced by significantly fewer major bleeding events. The study concluded that LDER of edoxaban might be considered in high-bleeding risk patients. Our study cohort consisted of patients who were indicated for on-label reduced-dose edoxaban (HDER). Severe renal dysfunction or extremely low body weight showed no significant increased risks of all of the outcomes after adjusting for an age factor. Interestingly, a higher HAS-BLED score was associated with increased composite clinical outcomes. Higher combination of CHA2DS2-VASc and HAS-BLED score showed a similar result. The predictive power of both scores combined was significantly enhanced for mortality outcome compared to that of each score alone.16 Therefore, our results support the conclusion of the previous study and indicate the importance of bleeding risk, even in an on-label reduced-dose protocol. Lee et al.17 reported the benefits for edoxaban in real world Asian population. In subgroup analysis, edoxaban 30 mg (n = 2,371) showed similar net clinical benefit compared to warfarin. Our study demonstrated prospectively the benefits of on-label reduced dose edoxaban.
This study had some limitations. This study was a non-interventional single-arm observational study. Therefore, there was no control group, and it was difficult to directly compare the outcomes to those of a randomized control study. Nevertheless, our results indicated the safety and efficacy of on-label reduced-dose edoxaban in the real world. Second, this study included only a Korean population, representing a single ethnic group of East Asian. These results might not represent all races, who may have different characteristics from those of a non-Asian population. However, Asians have a large distribution of low body weight, and there are many Asian patients who are indicated for reduced-dose regimen. Therefore, our study result can be thought of as being applicable to a significant number of patients who need dose reduction. Finally, we were not able to measure the plasma concentrations or anti-factor Xa activity and could not determine a correlation of plasma concentration, anti-factor Xa activity, and occurrence of clinical outcomes.
In conclusion, this study revealed large-scale data on the safety and effectiveness of on-label reduced-dose edoxaban in an Asian population. On-label reduced-dose edoxaban can be used safely even in patients with severe renal dysfunction or extremely low body weight. Our observation suggests that physicians should consider bleeding risks, even in a low-dose regimen.
 XML Download
XML Download