

 PDF
PDF Citation
Citation Print
Print



Takayasu’s arteritis is a chronic granulomatous vasculitis involving the aorta and its branches with characteristic clinical and angiographic features.1 A rare case of hyperaldosteronism due to renal artery stenosis in Takayasu's arteritis has been reported earlier.23 We report a case in which hyperaldosteronism caused by renal artery stenosis due to Takayasu's arteritis was successfully treated with balloon angioplasty.
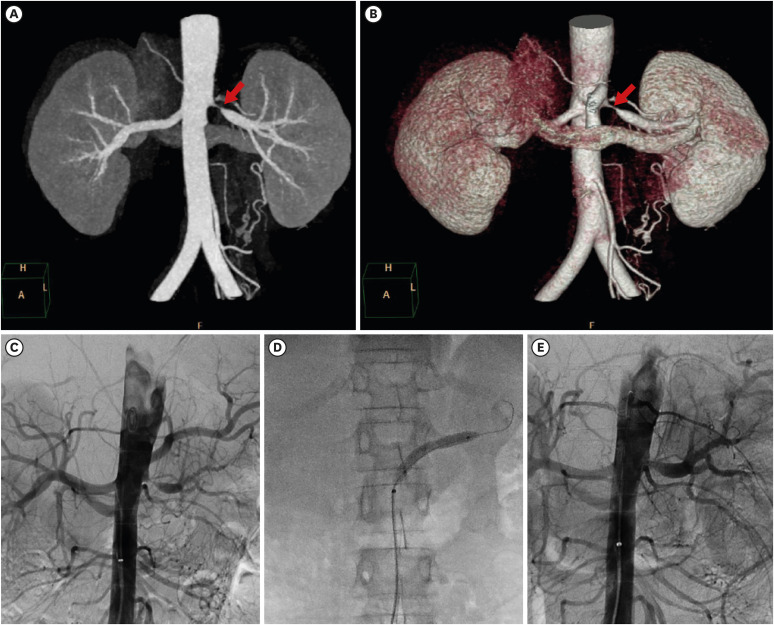
A 15-year-old male patient visited the hospital with intermittent abdominal pain and fever for 2 months. His blood pressure was 162/94 mmHg and body temperature, 38.2°C. There was no difference in blood pressure measured in both arms, and a bruit was auscultated in the abdomen. Left renal artery stenosis was observed on abdominal artery computed tomography angiography (Fig. 1A and B). Blood tests showed a white blood cell count of 8,190/μL, C-reactive protein level of 15.3 (0–0.3) mg/dL, erythrocyte sedimentation rate of 32 mm/hr, serum sodium level of 132 (136–145) mmol/L, and serum potassium level of 2.5 (3.5–5.1) mmol/L. Anti-nuclear antibody and anti-neutrophil cytoplasmic antibody tests performed to differentiate other diseases yielded negative results. Hyperaldosteronism was suspected due to hypertension, hypokalemia, and renal artery stenosis, and additional tests showed plasma renin activity of 8.42 (0.3–2.9) ng/mL/hr and an aldosterone level of 865.43 (1.2–34.0) pg/mL.
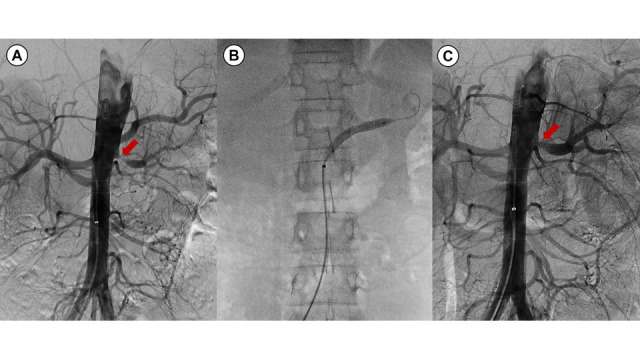
After the diagnosis of Takayasu arteritis (Type IV), high-dose steroid treatment (prednisolone 1 mg/kg) was started, after which fever and inflammation (ESR; 16 mm/hr, CRP; 0.01 mg/dL) improved, but hypertension and hypokalemia persisted; thus, a calcium channel blocker and spironolactone were prescribed. However, as the hypokalemia persisted, balloon angioplasty was performed for left renal artery stenosis (Fig. 1C, D, and E). Balloon angioplasty was first performed using a 4 mm x 4 cm balloon catheter, and then performed again using a 6 mm x 4 cm balloon catheter. The blood pressure gradually improved to normal. And after 5 days of angioplasty, renin activity (1.65 ng/mL/hr), aldosterone (24.3 pg/mL), and potassium (3.7 mmol/L) levels showed improvement to the normal range. Therefore, the calcium channel blocker and spironolactone were discontinued. Blood tests performed 2 months after angioplasty showed that ESR, CRP, potassium, renin activity, and aldosterone were all within normal ranges. Antihypertensive drugs and spironolactone were not added again, and follow-up will be continued.
In patients with Takayasu arteritis, if renal artery stenosis is associated with hyperaldosteronism, balloon angioplasty may be a good option to treat hyperaldosteronism.
 XML Download
XML Download