

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The incidence of cardiovascular diseases (CVDs) has been increasing worldwide. CVDs are one of the leading causes of increased disease burden in the world [1]. In addition, CVDs rank second in mortality in South Korea, posing a significant public health challenge nationwide [2]. In particular, atherosclerosis is a primary pathophysiology contributing to CVDs. It is aggravated by chronic inflammation of blood vessels due to accumulation of lipids [3].
Low serum 25-hydroxyvitamin D3 (25[OH]D) concentration is a known risk factor for arterial calcification [4]. Low serum vitamin D concentration (25[OH]D) is associated with metabolic diseases that can increase the incidence of CVDs with a high mortality rate [5]. Especially, atherosclerosis associated with low serum vitamin D concentration may play an essential role in developing vascular inflammation, thereby increasing the risk of CVDs [56].
Homocysteine is known to be an independent risk for CVDs. It can be modified by nutrition or lifestyle changes [7]. We have recently published a study showing that homocysteine is an independent factor for the increase of coronary artery calcification [8].
Apolipoprotein B (ApoB) is synthesized in the liver and small intestine to transport cholesterol to peripheral tissues. ApoB is a single-molecule component of the low-density lipoprotein (LDL), very-low-density lipoprotein (VLDL), intermediate-density lipoprotein, and lipoprotein(a) that can cause arterial wall inflammation [9]. Although plasma LDL cholesterol (LDL-C) is well established as a predictor of coronary artery disease (CAD), it may not be the best marker for reflecting arterial inflammation. Recent epidemiological studies and statin clinical trials have shown that ApoB is superior to LDL-C in predicting CAD [10].
A meta-analysis research has described that vitamin D deficiency can elevate body mass index (BMI) and serum concentrations of glucose, total cholesterol, triglycerides, and LDL-C which are associated with metabolic syndrome [11]. Korean studies have also reported that vitamin D deficiency may increase metabolic syndrome which is a risk factor for CVDs [1213].
The proposed mechanisms of low serum 25(OH)D associated with cardiovascular events include increased insulin resistance, renin-angiotensin-aldosterone system activation, and increased parathyroid hormone, which can induce inflammation of blood vessels and metabolic disorders [6].
Meanwhile, an intervention study did not prove the preventive effect of supplemental vitamin D on heart diseases or cancer, although many cross-sectional studies showed the relevance [14]. However, this intervention study had a crucial limitation in that the mean baseline serum 25(OH)D level was 30.8 ng/mL, which was a relatively sufficient concentration. Many previous cross-sectional studies have indicated that sufficient maintenance of serum 25(OH)D level can reduce CVD risk, especially in the low serum 25(OH)D level group. [15].
As low serum 25(OH)D level increases CVD risk, we have wondered if there are any other factors contributing to low serum 25(OH)D besides conventional risk factors that define metabolic syndrome such as obesity, diabetes mellitus, hypertension and dyslipidemia. Furthermore, if evidence on the relation between low serum 25(OH)D and factors other than conventional risk factors are accumulated, we can better understand how low 25(OH)D level causes CVDs. Therefore, we tried to find out which factor might be more related to low serum 25(OH)D in our data set (coronary artery calcium score [CACS] Study group), although this study had a cross-sectional design.
SUBJECTS AND METHODS
Data sources
In this cross-sectional study, a total of 777 subjects (CACS Study group) who had coded data of CACS in one health promotion center in Seoul, Republic of Korea, from January 2010 to December 2016 were analyzed [8]. Included subjects were those who were not diagnosed with CVDs (e.g., cardiac arrest, CAD, ischemic heart disease, stroke, and other established diseases of cardiovascular origin). Data of 259 participants who did not have at least one of the following data were excluded: serum 25(OH)D (n = 168), homocysteine (n = 101), and ApoB (n = 239). A total of 518 study subjects were included for analysis. Study group characteristics including sex, age, BMI, blood pressure, and laboratory data such as fasting glucose, triglyceride, high-density lipoprotein cholesterol (HDL-C), LDL-C, homocysteine, 25(OH)D, ApoB, and CACS were reviewed. The Institutional Review Board (IRB) approved this study (No. AJIRB-MED-MDB-16-268, CHAMC-2016-10-020) after obtaining proper informed consent.
Anthropometric measurements and laboratory data
Information on medical history and lifestyle factors were gathered from self-administered questionnaires that subjects filled out during routine health check-up. Smoking history was ascertained by statement such as “I am a current smoker” or “I have never been a smoker or past smoker.” Participants’ height and weight were measured using an automated digital height and a weight scale, respectively. BMI (kg/m2) was calculated by dividing weight in kilograms by the square of height in meters. Blood pressure was measured with an automated sphyngmomanometer in a sitting position. Fasting blood samples analyzed within one day of sampling were drawn in the morning and stored at 4°C. These samples were immediately processed, refrigerated, and transported to the central testing institute (NeoDin Medical Institute, Seoul, Korea), where they were analyzed within 24 hours. Glucose and lipid profiles were analyzed with an automatic analyzer (HITACHI7600, Tokyo, Japan). Specifically, circulating ApoB levels were measured using an enzyme-linked immunosorbent assay (Roche, Basel, Switzerland). Serum homocysteine was measured with a fluorescence polarization immunoassay using an IMx Analyzer (Axsym Abbott, Abbott Park, IL, USA). Serum 25(OH)D concentration was measured with a radioimmunoassay kit (DiaSorin Inc., Stillwater, MN, USA) using a γ-counter (1470Wizard; PerkinElmer, Turku, Finland). CACS, a useful index of subclinical coronary atherosclerosis [16], was measured with a 64-slice computed tomography scanner (GE light speed VCT; GE Imatron, San Francisco, CA, USA). Scan parameters were: slice thickness, 3 mm; tube voltage, 120 kV; and tube current, 110 mAs. CACS was analyzed with a SmartScore software (GE Healthcare, San Francisco, CA, USA).
Statistical analysis
Data are presented as mean and SD. Frequency analysis was performed to determine the prevalence of hypertension, type 2 diabetes mellitus (type 2 DM) and smoking status. Simple and partial correlation analyses were performed to determine relationships of serum 25(OH)D with metabolic parameters including homocysteine and ApoB after sex and age adjustments. Simple linear regression analysis was performed if there was a significant linear pattern among serum 25(OH)D, homocysteine, and ApoB. In addition, multivariate regression analysis was done to know which factor (serum homocysteine or ApoB) was more associated with serum 25(OH)D after sex, age, BMI, hypertension and type 2 DM adjustments. Finally, because serum homocysteine (not ApoB) showed a skewed pattern, it was log-transformed to obtain a linear association. We then compared serum log(homocysteine) concentrations according to tertiles of serum 25(OH)D using a general linear model after sex, age, BMI, hypertension, and type 2 DM adjustments. P-value < 0.05 was considered statistically significant. All sample analyses were performed with SPSS version 25.0 (IBM Corp, Armonk, NY, USA).
RESULTS
Participant characteristics
General information and laboratory data of study subjects are presented in Table 1. Among the 518 subjects included in this study, the number of females was 126 (24.3%). The average age of all included subjects was 55.6 years. Hypertension and type 2 DM were diagnosed in 198 (38.8%) and 103 (20%) patients, respectively. The average serum 25(OH)D concentration was 16.7 ng/mL. Mean serum homocysteine and ApoB levels were 11.3 μmol/L and 108.4 mg/dL, respectively.
Table 1
General characteristics of study subjects (n = 518)
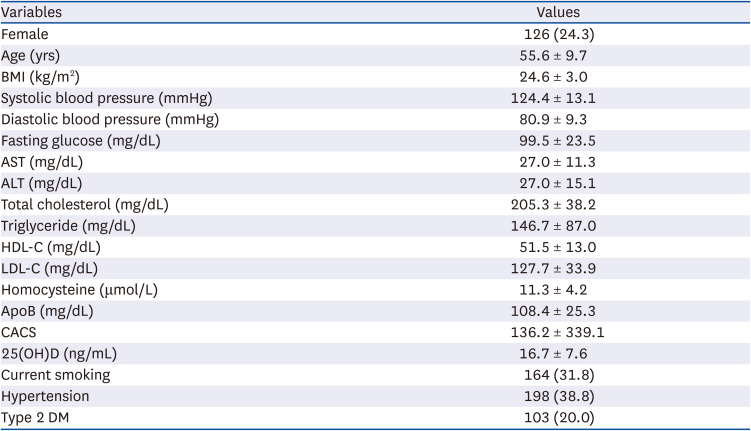
Variables are presented as mean ± SD or number (%) by descriptive method.
BMI, body mass index; AST, aspartate transferase; ALT, alanine transferase; HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol; ApoB, apolipoprotein B; CACS, coronary artery calcium score; 25(OH)D, 25-hydroxyvitamin D3; type 2 DM, type 2 diabetes mellitus.
Associations of serum 25(OH)D with serum homocysteine and ApoB
Serum 25(OH)D showed significant correlations with many metabolic parameters. However, based on partial correlation (r’) after sex and age adjustments, Serum 25(OH)D showed a statistically significant positive correlation with HDL-C (r’ = 0.140, P < 0.05) and negative correlations with homocysteine (r’ = −0.114, P < 0.05), ApoB (r’ = −0.098, P < 0.05), BMI (r’ = −0.121, P < 0.05), and triglyceride (TG) (r’ = −0.188, P < 0.05) (Table 2). Simple linear regression analysis showed that 25(OH)D had a negative correlation with ApoB (P = 0.035). In contrast to our expectation, 25(OH)D showed a negative correlation with homocysteine without statistical significance (P = 0.085) (Table 3). However, multivariate regression analysis revealed a significant correlation of serum 25(OH)D with homocysteine but not ApoB after adjusting for sex, age, BMI, hypertension, and type 2 DM (P = 0.022) (Table 4). In addition, the lowest tertile of 25(OH)D concentration had a higher log homocysteine (P = 0.046) (Table 5).
Table 2
Simple (r) and partial (r’) correlations of serum 25(OH)D with other factors
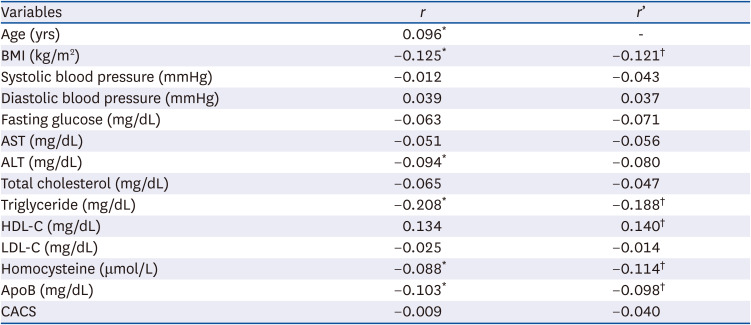
Variables are presented as simple (r) and partial (r’) correlation coefficients.
25(OH)D, 25-hydroxy vitamin D3; BMI, body mass index; AST, aspartate transferase; ALT, alanine transferase; HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol; ApoB, apolipoprotein B; CACS, coronary artery calcium score.
*P-value < 0.05 by simple correlation.
†P-value < 0.05 by partial correlation after sex and age adjustments.
Table 3
Simple linear regression analysis of serum 25(OH)D with homocysteine and ApoB

| Variables | β* | t | P-value |
|---|---|---|---|
| Homocysteine | −0.076 | −1.727 | 0.085 |
| ApoB | −0.093 | −2.113 | 0.035 |
Table 4
Multivariate regression analysis of serum 25(OH)D with homocysteine and ApoB

| Variables | β* | t | P-value |
|---|---|---|---|
| Homocysteine | −0.106 | −2.297 | 0.022 |
| ApoB | −0.065 | −1.374 | 0.170 |
Table 5
Log(homocysteine) concentration according to 25(OH)D tertiles

| Tertile | Mean ± SD | P-value |
|---|---|---|
| T1† | 2.401 ± 0.337 | 0.046* |
| T2‡ | 2.351 ± 0.243 | |
| T3§ | 2.369 ± 0.288 |
P-value among groups is presented by general linear model after sex, age, BMI, hypertension, and type 2 DM adjustments.
25(OH)D, 25-hydroxy vitamin D3; BMI, body mass index; type 2 DM, type 2 diabetes mellitus.
*P-value < 0.05. †T1: 1st tertile of serum 25(OH)D: 4.2–12.7 ng/mL (mean 9.7 ng/mL); ‡T2: 2nd tertile of serum 25(OH)D: 12.8–19.1 ng/mL (mean 15.7 ng/mL); §T3: 3rd tertile of serum 25(OH)D: 19.2–41.5 ng/mL (mean 25.8 ng/mL).
DISCUSSION
It is well known that vitamin D deficiency is associated with CVDs such as CAD, myocardial infarction, cardiac failure, fibrosis, cardiomyopathy, atherosclerosis, hypertension and peripheral arterial disease [17]. However, the mechanism of vitamin D-mediated protection of CVD remains unclear.
In previous studies based on Korean National Health and Nutrition Examination survey data, BMI and LDL-C were high in a healthy adult group with low serum 25(OH)D concentrations [12]. Also, TG was high while HDL-C was low in an elderly group with low serum 25(OH)D concentrations [1819]. Similarly, in our study, serum 25(OH)D concentration had negative correlations with BMI and TG and a positive correlation with HDL-C after adjustment. This shows that serum 25(OH)D is closely related to metabolic markers including BMI, TG, LDL-C, and HDL-C.
In addition to conventional metabolic markers, serum 25(OH)D also showed negative correlations with homocysteine and ApoB based on simple correlation and partial correlation (Table 2). Thus, further investigation to verify the relationship of 25(OH)D, homocysteine and ApoB is needed to study the mechanism between vascular inflammation and dyslipidemia.
LDL-C has been well established as a pathophysiology of CVD and atherosclerosis [20]. In fact, the ApoB particle surrounding lipoprotein is the basic unit of vascular wall injury. Higher concentrations of ApoB particles floating in the lumen of an artery can cause more trapping of ApoB particles in the arterial wall, inciting further injury to the blood vessel wall [9]. In general, 90% of all ApoB particles are contained in LDL-C. The remaining 10% are in VLDL except for those with familial dyslipoproteinemia [21]. Previous meta-analyses have shown that ApoB is a better predictor of CVD risk than LDL-C [2122]. Another meta-analysis has demonstrated the relationship of metabolic markers with coronary heart disease prevention and concluded that a change in ApoB reflects a decreased risk of CVD better than a change in non-HDL-C or LDL-C [23]. Therefore, ApoB-rich lipoprotein, e.g., LDL-C, can induce atherosclerotic CVD, whereas lipoproteins that are low in ApoB, such as HDL-C, do not cause arteriosclerosis [24]. Furthermore, measuring ApoB is inexpensive and highly accurate. Hence, it is a useful indicator of arteriosclerosis [25].
ApoB is an essential causative factor in arteriosclerosis evidenced by a negative correlation between ApoB and 25(OH)D [2627]. In accordance with our study, serum 25(OH)D had a negative correlation with ApoB after sex and age adjustments (Table 2). It also showed a statistically significant association with ApoB in simple linear regression analysis (Table 3). The mechanism behind this negative correlation remains unclear. However, an in vivo study has shown that cholesterol synthesis in the liver increased in vitamin D deficiency as a result of decreased vitamin D receptor activity, activation of regulatory element-binding protein 2 (SREBP-2; sterol), and increased HMG-CoA reductase is correlated with a decrease in intracellular insig-2 expression (insulin-induced gene) [28].
On the other hand, elevated homocysteine is known to raise CVD risk in many previous studies. A large cohort study has shown the same result [29]. When homocysteine concentration was reduced by 3 μmol/L, the risk of ischemic heart disease was reduced by 16% [30]. Serum homocysteine is an indicator of vascular inflammation. Our previous study has shown that serum homocysteine is a biomarker indicating the coronary artery calcification volume score, which is increased in relation to coronary artery calcification [8]. Serum homocysteine can increase the level of asymmetric dimethylarginine, an endogenous nitric oxide synthase inhibitor, thus inducing endothelial cell dysfunction and reducing maximal vasodilation capacity [31]. Moreover, serum homocysteine can increase the formation of reactive oxygen species that activates LDL-C oxidation, which in turn can induce the formation of foam cells, the primary constituents of atherosclerotic plaques, and the nuclear factor-κB complex that can induce pro-inflammatory gene expression [32]. Thus, LDL-C can accumulate due to dysfunction of vascular endothelial cells, forming an arterial plaque [3132]. Subsequently, plaque calcification and fibrosis can lead to CVD via LDL-C oxidation and persistent inflammatory damage in the arterial intima [29].
As such, many studies have shown that hyperhomocysteinemia can increase the risk of CVD by inducing inflammation of blood vessels [30]. However, the effect of using homocysteine lowering agent such as folic acid or vitamin B complex administration for the prevention of CVD has not been proven [3334]. This suggests that there might be other factors that can reduce the risk of CVD by lowering homocysteine. In previous studies, serum homocysteine was found to be decreased as 25(OH)D level increased [353637]. However, some studies have indicated that serum homocysteine concentration no longer decreases when the concentration of 25(OH)D reaches a certain threshold. [3839]. Similarly, our study showed that serum homocysteine concentrations were relatively high under the lower tertile of 25(OH)D concentration (Table 5), consistent with previously published studies [3839].
An in vitro study has shown that active vitamin D (1,25-dihydroxyvitamin D3) can activate cystathionine-β-synthase, an enzyme involved in decomposing homocysteine, which explains why active vitamin D independently affects homocysteine metabolism that is distinct from the pathway involved in vitamin B complex [40]. Although specific mechanisms underlying the relationship between serum homocysteine and the state of 25(OH)D remain unclear, vitamin D might have indirect or direct effects on homocysteine metabolism. Also, after adjusting for several factors, serum 25(OH)D was significantly associated with homocysteine but not ApoB (Table 4). This suggests that low 25(OH)D might be more associated with high homocysteine, which is related to microinflammation, than with high ApoB, which is a dyslipidemic abnormality. This mechanism cannot be confirmed. It is presumed to be complex. However, although we have a small number of subjects, significant relation of low 25(OH)D with high homocysteine but not with ApoB may indicate small inflammation in blood vessels.
This study has several limitations. First, this was a cross-sectional study. The number of study subjects (n = 518) might not be adequate to suggest a correlation among serum 25(OH)D, ApoB, and homocysteine levels. Secondly, although subjects were relatively healthy, cardiovascular CT could be more recommended to a high-risk group for CVD. Therefore, there might be selection bias because more elderly, hypertension and type 2 DM patients might have been included in the CACS Study group. Third, the average serum 25(OH)D concentration was similar to Korean mean level known in the 2008–2014 National Health and Nutrition Survey [41]. However, data related to effects of vitamin D intake, seasons, and sun exposure time on serum 25(OH)D were unavailable. In addition, levels of vitamin B6, B12, folate, and precise smoking history associated with homocysteine concentration were not fully adjusted. Nonetheless, this is the first study to correlate serum 25(OH)D concentration, ApoB, and homocysteine levels simultaneously.
In conclusion, serum 25(OH)D concentration showed negative correlations with homocysteine and ApoB. In addition, low 25(OH)D concentration was more associated with relatively high serum homocysteine than with ApoB. A further large-scale study is needed to establish the precise relationship.
 XML Download
XML Download